
Abstract
Flexor tendon rupture in the wrist of patients with rheumatoid arthritis is a rare complication, and there is no standard treatment for the wrist joint. Here, we present the case of a rupture of the flexor digitorum profundus of the left index finger owing to a rheumatoid wrist. Plain radiography and computed tomography showed carpal collapse, especially lunate, and arthrosis between the capitate and lunate. For stability and mobility of the wrist and index finger, resection of the lunate and radiotriquetral (RT) arthrodesis using the distal ulna as a bone graft and arthrodesis of the distal interphalangeal joint of the index finger were performed. At 2 years postoperatively, her wrist was painless and stable on radiography without recurrence of tendon rupture, and the arc of motion of the dorsal-palmar flexion of the wrist joint was 125°. RT arthrodesis could be a surgical choice of “mobile” partial wrist arthrodesis.
Introduction
Rheumatoid arthritis (RA) is a chronic autoimmune disease that is characterized by progressive inflammation. RA generally affects wrist joints and can lead to wrist deformities where the proximal carpal row translates both palmarly and ulnarly and supinates via cartilage degradation, ligamentous laxity, and synovial expansion with erosion. 1,2
Spontaneous flexor tendon rupture in patients with a rheumatoid wrist is a rare complication. 3,4 Flexor tendon rupture commonly occurs at the carpal tunnel owing to the infiltration of tenosynovitis to the tendon and attrition from the bony prominence of the wrist. 3,5 Although treatment options for the wrist joint to prevent further tendon ruptures are resection of the bony prominence and covering with the surrounding soft tissue or partial/total wrist arthrodesis, there are no gold standard procedures. 3,5 To our knowledge, radiolunate (RL), radioscaphocapitate, and radiolunotriquetral (RLT) arthrodesis can be used for partial wrist arthrodesis.
Here, we report a case of a rupture of the flexor digitotum profundus to the index finger owing to severe destructive rheumatoid wrist that was treated by arthrodesis of the distal interphalangeal (DIP) joint of the index finger and radiotriquetral (RT) arthrodesis to obtain a mobile wrist. In addition, we report the clinical results 2 years after the surgery.
Case report
A 64-year-old Japanese, right-handed woman with swelling and pain of the left wrist and inability to flex the left index finger visited our department. Her jobs were displaying and taking inventory at a supermarket and making clothes using a sewing machine at her house. She had past history of RA with a disease duration of 13 years. RA was managed using etanercept (25 mg twice a week), methotrexate (10 mg a week), and prednisolone (5 mg a day), which was prescribed by a previous doctor.
She experienced pain from her left forearm to index finger without trauma for 1 month before visiting our hospital. A physical examination showed swelling of the left wrist, and she could not actively flex the DIP joint of her left index finger. Flexion and extension of the other fingers were normal. There was no evidence of sensory disturbance. Ulnocarpal stress test was positive. The grip strengths for the right and left hands, measured using a dynamometer, were 14.0 and 11.7 kg (84% compared with the uninjured side), respectively. The respective range of motion for the right and left extremities, measured using a standard goniometer, was as follows: wrist dorsal flexion, 80° and 75°; wrist palmar flexion, 75° and 60° with pain; forearm pronation, 90° and 60° with pain; and forearm supination, 90° and 90°.
Plain radiographs of the left wrist revealed severe proximal carpal collapse and palmar and ulnar translation of the carpus; the disintegration type was classified by Flury et al. 6 (Figure 1(a) and (b)). Computed tomography showed extreme lunate collapse, arthrosis between the capitate and lunate and of distal radioulnar joint (DRUJ), and a palmar bony prominence of the radius (Figure 1(c)). Magnetic resonance imaging showed suspected flexor tendon rupture in the carpal canal. A blood examination revealed a C-reactive protein level of 0.20 mg/dl and a rheumatoid factor of 183 mg/dl. The diagnosis was rupture of the flexor digitorum profundus (FDP) of the index finger owing to a rheumatoid wrist. The disabilities of the arm, shoulder and hand (DASH) score was 30 in disability/symptom and 50 in work.
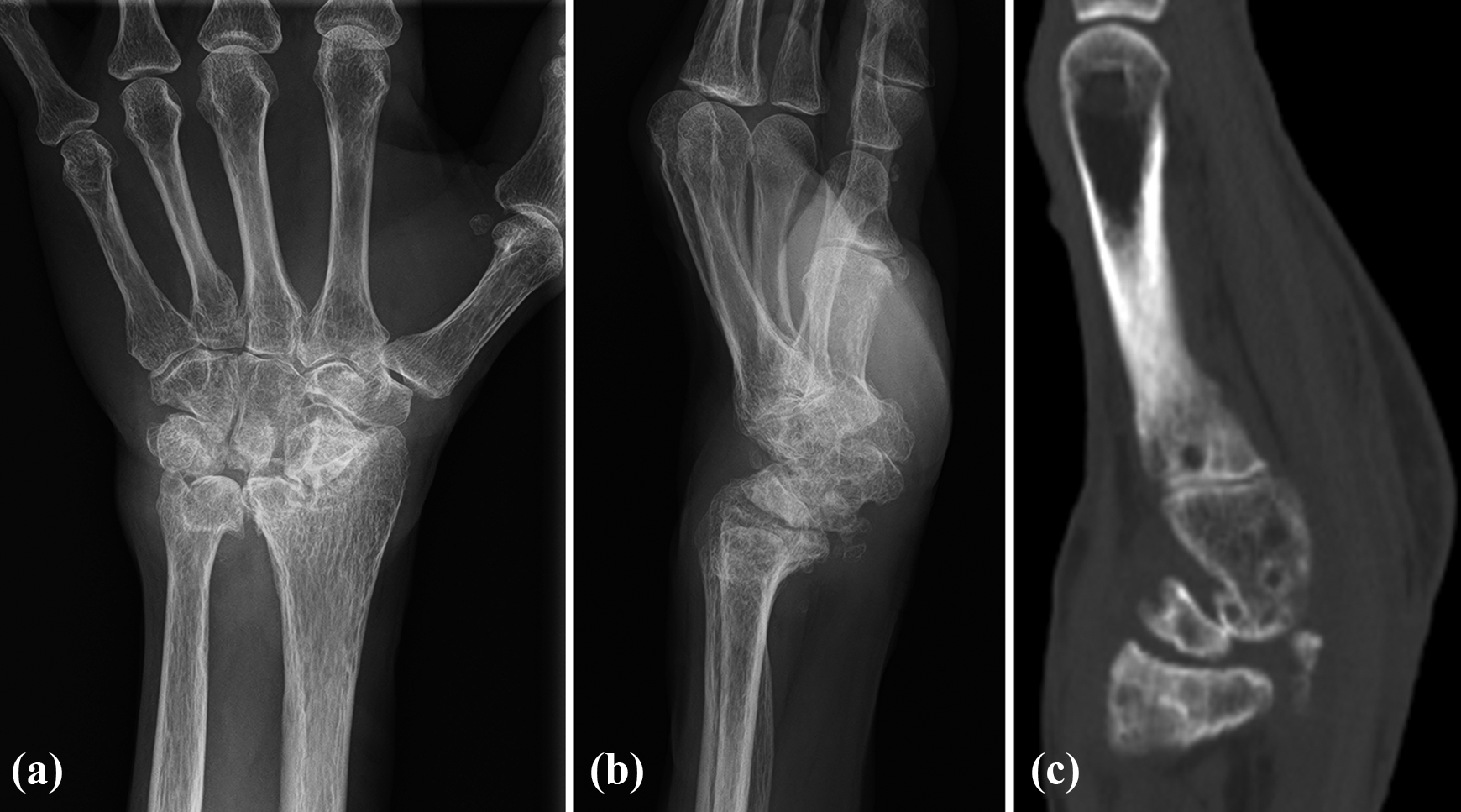
Preoperative plain radiography and CT. (a) Anteroposterior view of the left wrist. Carpal collapse and ulnar shift of the carpus were noted. (b) Lateral view of the left wrist. Palmar subluxation of the carpus was noted. (c) Sagittal CT image. Lunate is collapsed, and arthrosis between the capitate and lunate was found. CT: computed tomography.
Reconstructive operations, such as flexor tendon reconstruction or arthrodesis of the DIP joint in the index finger, total wrist arthrodesis, or partial wrist (RL, RSL, and RLT) arthrodesis using an iliac bone graft in the wrist, were suggested. Resection of distal ulnar (Darrach procedure) was also offered for arthrosis of DRUJ and ulnocarpal impaction syndrome. Arthrodesis of the DIP joint in the index finger and mobile wrist without an iliac bone graft was selected by the patient because she wanted to return to work as soon as possible, have the ability to perform pinching motion using her index finger, and avoid complications associated with harvesting the bone graft. Methotrexate and prednisolone were continued during the perioperative period. Etanercept was discontinued for 1 week preoperatively and 2 weeks postoperatively.
The operation was performed under general anesthesia using a pneumatic tourniquet. With a palmar approach to the wrist, the carpal tunnel was opened. Evidence of tenosynovitis of the flexor tendon resulted in tenosynovectomy being performed. The FDP of the index finger was ruptured, and that of the middle, ring, and little finger showed a partial attrition at the carpal canal. The flexor digitorum sublimis and flexor pollicis longus were intact. The palmar capsule was ruptured, and bony prominence of the radius was found at the site of the carpal tunnel (Figure 2(a)). After resection of the bony prominence, the sliding floor was repaired using the surrounding capsule. Using a dorsal incision, synovectomy of the extensor tendons from the third to the fifth compartment and denervation of the posterior interosseous nerve with a Darrach procedure without stabilization of the ulnar stump were performed. The ulnar stump was meticulously covered with the periosteum and circumferential soft tissue including the pronator quadratus. The dorsal capsule was raised under the periosteum to expose the radiocarpal and midcarpal joints. Synovectomy for both joints was performed, and the condition of the joint was examined. The cartilage of the radioscaphoid (RS) joint was relatively preserved. There was severe collapse of the lunate and it was not feasible to fix using implants. After resection of the lunate and refreshing the lunate fossa of the radius and radial side of the triquetrum, the distal ulna was trimmed into a trapezoidal shape, grafted in between the radius and triquetrum, and fixed with three 1.5-mm wires while performing a reduction of the palmar and ulnar translation of the carpus (Figure 2(b) and (c)). Finally, the arthrodesis of the DIP joint in the index finger was performed using wires via a dorsal approach.

Intraoperative photograph and postoperative plain radiography. (a) Intraoperative photograph. Rupture of the palmar capsule at the carpal canal and partial attrition of the flexors were noted. (b) Anteroposterior view of the left wrist. Darrach procedure and RT arthrodesis using a resected ulna as a bone graft. (c) Lateral view of the left wrist. RT: radiotriquetral.
Postoperatively, bulky dressing and sugar tong splint were applied. Finger motion exercise was started from the next day after surgery. At 2 weeks after surgery, she went back to work. The left wrist was immobilized with a cast until 8 weeks postoperatively when a removable wrist brace was then used. At 3 months postoperatively, the wires were removed. The grafted bone was tilted in the ulnar direction during the postoperative course. After obtaining stability of the grafted bone, free activity was permitted at 6 months postoperatively. RA control was changed to tocilizumab (400 mg per 4 weeks), methotrexate (10 mg a week), and prednisolone (4 mg a day) from 6 months postoperatively.
At the final follow-up, that is, 2 years postoperatively, she was painless without recurrence of flexor tendon rupture. Her grip strengths were 22.3 kg and 15.1 kg (68% compared with the uninjured side) and pulp pinches were 2.6 kg and 1.6 kg (62% compared with the uninjured side) for the right and left hands, respectively. The range of motion of the left extremity was as follows: wrist dorsal flexion, 70°; wrist palmar flexion, 55°; forearm pronation, 80°; and forearm supination, 90° (Figure 3(a) and (b)). The active extension/flexion ranges of motion of the index finger were as follows: metacarpophalangeal joint, 0°/95°; proximal interphalangeal (PIP) joint, 20°/90°; and DIP joint, −10°/10°. The DASH score was 29.2 disability/symptom and 25 in work. Radiographic parameters of the wrist, ulnar shift of the carpus, palmar subluxation of the carpus, and carpal collapse ratio during the perioperative period were measured, as in previous reports, and are shown in Figure 4. 7 –9 Ulnar shift of the carpus was reduced by the surgery but was lost from 3 to 6 months postoperatively and maintained after then. Palmar subluxation of the carpus was reduced until the last follow-up (Figure 3(c) and (d)). The carpal collapse ratio was maintained until the last follow-up.

Clinical photograph and plain radiography at the last follow-up. (a) Wrist dorsal flexion and (b) wrist palmar flexion. (c) Anteroposterior and (d) lateral view of the left wrist. Bone union of arthrodesis was obtained, and palmar subluxation of carpus was well reduced.
The patient was informed that data from the case would be submitted for publication, and she gave her consent for a publication.
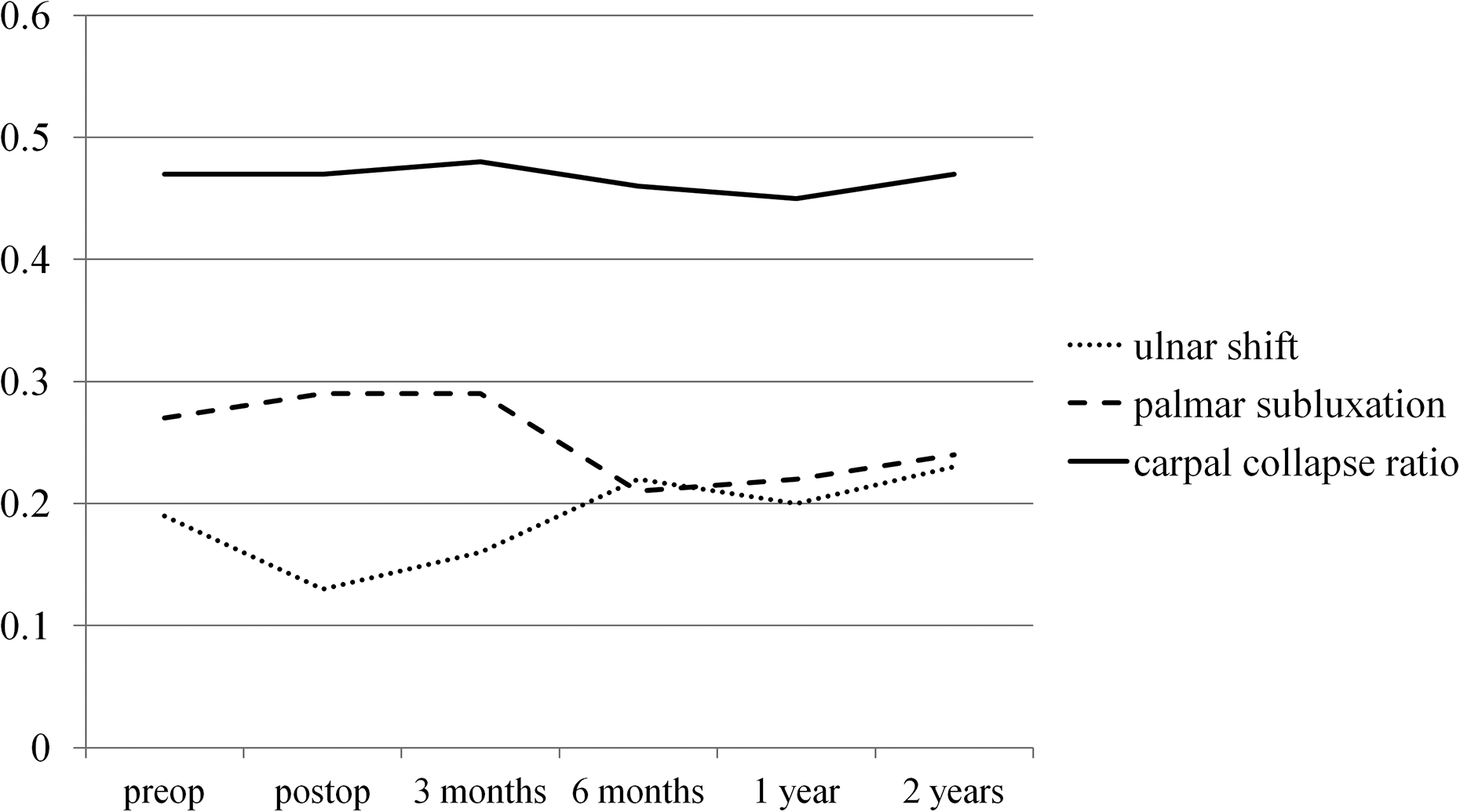
Radiographic parameters of the wrist in the perioperative period. Sequential changes of the ulnar shift of the carpus, palmar subluxation of the carpus, and the carpal collapse ratio are shown. preop: preoperation, postop: postoperation.
Discussion
We report the case of rupture of the FDP to the index finger owing to severe destructive rheumatoid wrist, which was treated by arthrodesis of the DIP joint of the index finger and RT arthrodesis to obtain a mobile wrist. RT arthrodesis maintained the motion of the wrist joint and prevented further rupture of the flexor tendons at 2 years postoperatively.
Tendon rupture is a complication associated with rheumatoid wrist. The frequency of flexor tendon rupture is less than that of the extensor tendon rupture. 3,4 The most common site of flexor tendon rupture is the carpal tunnel, which is caused by infiltration of tenosynovitis to the tendon and attrition by the bony prominence of the wrist. 3,5,10 Procedures to prevent further rupture in the wrist joint are controversial, including resection of the bony prominence and covering with surrounding soft tissue or partial/total wrist arthrodesis. Although total wrist arthrodesis is a good treatment option for patients with a severely destructive joint to acquire a stable and painless joint, daily activities, such as personal hygiene, handling coins, and fastening buttons, become impaired because of the loss of range of motion. 11
Funahashi et al. reported the recurrence of flexor tendon rupture in a patient with rheumatoid wrist treated by reconstruction of the tendon and resection of the bony prominence and covering with soft tissue. 5 Moreover, synovectomy of the wrist joint cannot control the progression of carpal collapse. 12 On preoperative discussion with this patient, she selected a mobile wrist to maintain her ability to perform manual work. Therefore, we hypothesized that partial wrist arthrodesis for a stable, mobile wrist was the most appropriate procedure among those aforementioned because this surgical procedure showed good clinical and radiological results in a long-term follow-up study. 13 Arimitsu et al. showed the kinematics of both stable and unstable types of rheumatoid wrists by using three-dimensional computed tomography. 14 The motion of the midcarpal joint was 67% of the total wrist motion in the unstable type, and wrist motion could be preserved by retaining mobility of the midcarpal joint, such as with RL arthrodesis. However, in this case, preserving the distal articular surface of the lunate was a possible cause of pain because preoperative computed tomography images showed the arthrosis between the capitate and lunate. Moreover, because collapse of the lunate was severe in our case, it was difficult to perform rigid fixation without bone block of the ilium. Therefore, RL, RSL, and RLT fusions were not good options. Regarding other types of partial wrist arthrodesis, RS or RT fusion is an option after resection of the lunate. Because joint space narrowing between the scaphoid and capitate was reported in a radiographic study of the rheumatoid wrist, the clinical outcome of RS fusion in the long term may be unclear. 15 There has been also no clinical report about RS fusion in patients with RA. Taleisnik reported that the joint between the triquetrum and hamate was not impaired in RA. 16 Arimitsu et al. also reported that the articular surface of the midcarpal joint, which has osseous integration and a concave and convex joint surface, could be preserved more than that of the radiocarpal joint. 14 In the natural course of carpal deformity, carpal translation proceeds along the inclination of the radius. 1 The triquetrum itself has radial inclination in the carpal bones, and we used the triquetrum as a wall against the ulnar translation of the distal carpal row. Intraoperatively, ulnar translation of the carpus was reduced, but the grafted bone was tilted postoperatively and ulnar translation was returned to the preoperative condition because the position of the scaphoid was the same between the preoperative and final follow-up periods. For fixation of the triquetrum, grafted bone, and radius, a headless screw or locking plate might have greater stability than wires. Finally, we were able to achieve a mobile wrist using the scaphotrapeziotrapezoid, RS, and triquetohamate joints and a stable wrist after the grafted bone achieved union, and there was no recurrence of flexor tendon ruptures at 2 years postoperatively. Carpal collapse and deformity can occur when medical control of RA is not good, even in a wrist that has been operated on. 17 Therefore, long-term follow-up and appropriate medication are necessary.
For rupture of the FDP tendon with an intact flexor digitorum sublimis tendon of the index finger, there are some surgical reconstruction methods, such as tendon transfer, tendon grafting, tenodesis, and arthrodesis of the DIP joint. 5,10,18,19 Postoperative ranges of motion of the fingers with flexor tendon rupture in RA treated by tendon reconstruction have been reported in previous studies. Funahashi et al. reported average DIP flexion of 23°, DIP extension of −2°, PIP flexion of 42°, and PIP extension of −4°; Kobayashi et al. reported an average DIP flexion of 57° and DIP extension of −17°; and Ertel et al. reported an average PIP arc of motion of 55°. 5,10,19 Based on these reports, the results of tendon reconstruction were not satisfactory in terms of the ranges of motion of not only the DIP joint but also the PIP joint, which is supposed to be affected by tendon adhesion. However, a stable joint instead of range of motion can be obtained by arthrodesis of the DIP joint, although there is a risk of nonunion, infection, and skin complications. 20 Arthrodesis was performed by tension band wiring, and our patient returned to work with use of her index finger at 2 weeks postoperatively. There was no contracture of the MP and PIP joints of the index finger, and good pinch strength was achieved at 2 years postoperatively. These two opposite treatments need to be discussed and decided between the patient and physician during the preoperative period.
Conclusion
We report the case of FDP tendon rupture of the index finger in a patient with rheumatoid wrist of the unstable type. RT arthrodesis maintained the motion of the wrist joint and prevented further rupture of the flexor tendons at 2 years postoperatively.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.