
Abstract
Background:
Fractures of the proximal femur is one of the most frequent human injuries, and most of the patients are treated with osteosynthesis, such as intramedullary nails. These patients often require magnetic resonance imaging (MRI) scans in their further lives due to various reasons. This raises the question of whether complications with implanted osteosynthesis material such as implant loosening, burning, dislocation, or other complications are to be expected or whether an MRI examination is even suitable with regard to imaging artifacts.
Methods:
The aim of this retrospective study was to investigate the rate and type of complications after MRI examinations in patients with inserted intramedullary osteosynthesis device. Furthermore, artifacts in MRI caused by this device were assessed.
Results:
MRI scans of the head (20 of 62), spine (20 of 62), pelvis (10 of 62), and lower extremity (6/62) were performed. Three of the 62 patients received an MRI of the abdomen, and 2 of the 62 patients received an MRI of the thorax and the upper extremity. Of the 62 patients, noneexperienced complications during the immediate examination. Similarly, none of the patients showed early complications within the first 2 weeks after MRI. In our long-term follow-up examination, no long-term complication after MRI was observed in the recorded 15 patients. Artifacts were found in 14 patients: in MRI scans of the pelvis (10/10), of the abdomen (2/3), and of the lower extremity (2/6).
Conclusion:
There were no complications during the MRI scan, in the first 2 weeks after MRI, or in the recorded long-term results. MRI with an enclosed intramedullary nail provided good image quality unless the immediate implant site was imaged. MRI diagnosis is thus possible in patients with an inserted intramedullary nail. The inserted intramedullary nail should therefore not be an exclusion criterion when sectional imaging with MRI is required.
Keywords
Introduction
Fractures of the proximal femur have always been regarded as “problem fractures,” and the adequate therapy of this fracture has always been a focus of research.
It is not only the fracture of the proximal femur that poses new challenges to medicine but also the aging population. Thanks to modern medicine, both the treatment of patients with new therapies and life expectancy are constantly increasing. Fractures of the proximal femur can be treated using an intramedullary nail such as, for example, the gliding nail, so that patients receive optimal care for their fracture, and they can actively participate in life again at an early stage. But, there are also problems in this regard.
However, due to aging in the course of life, further diagnostics are often required because of other diseases. Imaging procedures, in particular magnetic resonance imaging (MRI) scans, have increased in importance in recent years. These imaging procedures often take place without the examiner’s direct knowledge of other diseases or possible closed implants, as in an emergency situation, for example. So far, complications such as overheating, pain, or even dislocations of metallic implants have been described. 1 –3 Imaging artifacts, caused by the disturbance of the built-up magnetic field, are also known to be a drawback of MRI after implantation of metallic protheses. 4 However, literature on the frequency and extent of these complications and on the interaction of implant and MRI are rare. Especially large implants are becoming increasingly common and may bear an even larger risk for complications.
With regard to the body of literature, both immediate complications, such as pain or burning, and long-term complications, such as implant dislocation with consequential fracture or permanent pain, can be considered. 2,3,5
This raises the questions of whether (1) MRI is also possible in patients with closed osteosynthesis material such as the gliding nail, 2) complications such as implant loosening, burning, dislocation, or other events occur, or (3) MRI diagnostics are completely unsuitable.
The following questions will be addressed in this article: – Are there any complications immediately during the examination or during its further course? – Are there any artifacts that stand in the way of a reliable diagnosis?
Patients and methods
In our Center for Orthopedics, Trauma Surgery and Sport Medicine, a collective of 62 patients was recorded from January 1, 2007 to May 1, 2016, and an MRI scan was performed in each patient on a closed intramedullary nail.
Twenty-eight of the 62 patients had died at the time of the follow-up examination in 2018. Nineteen patients could not be included in the follow-up examination. A total of 15 patients could be recorded in the long-term follow-up examination.
The mean follow-up time was 63.67 months (median 56.38; minimum–maximum 15.93–132.63). The mean age of the patients at the time of imaging was 78 years (median 79; minimum–maximum 47–96). The female sex was represented by 44 of 62 patients.
Inclusion criteria were a proximal femoral fracture treated with an implantation of a gliding nail as well as an MRI scan performed during the course of their lifetime, independent of the examined body region.
The data evaluation was based on the collected patient data with anamnesis sheets, findings of the imaging diagnostics, recorded anesthesia protocols, operation reports, ward curve sheets, physiotherapeutic protocols, and the corresponding doctor’s letter. The patients were also contacted again and interviewed using a standardized questionnaire, including questions with respect to their way of life, their daily life activities, walking distance, operations, and pain. Patients were asked to complete standardized questionnaires about their daily activities and capabilities, focusing on strength, coordination, and functionality of the injured extremity. Perceived pain and the overall satisfaction of medical care were also assessed.
The implant used is the INTERCUS Gliding Nail (Intercus GmbH, Bad Blankenberg, Germany), which is used in our clinic for femoral neck fractures, pertrochanteric or subtrochanteric fractures. 6 –8
Radiological examination
All MRI examinations were performed using standard settings according to clinical practice.
The MRI scanners that were used in our department were Philips Healthcare Ingenia 1.5 T MR system (Philips Medical Systems DMC GmbH, Hamburg, Germany). Standard protocols were used for the respective body regions.
In addition to the existing radiological reports, the evaluation of the available MRI images was also carried out independently by two trauma surgeons. All reconstructed images were reviewed on a picture archiving and communication system (PACS) work station (CENTRICITY PACS 4.0; GE Healthcare, Barrington, Illinois, USA). The artifact severity and the feasibility of evaluating the adjacent anatomical structures tissue was graded using a five-point Likert-type scale: 1: major artifacts, no depiction of anatomical structures; 2: marked artifacts, no depiction of surrounding tissue, and considerably impaired image quality of distant tissue; 3: moderate artifacts, nondiagnostic in the surrounding tissue but fair diagnostic image quality of distant tissue; 4: minor artifacts with good image quality; and 5: no artifacts, full diagnostic image. 9,10
Ethics committee approval and evaluation of the data
A positive vote of approval by the institutional review board (IRB, Ethics Commission of the Medical Faculty of Heidelberg) on the conduct of this study is available under No. S-269/2014. Hence, the study was approved by the IRB and conducted according to the guidelines of the IRB and within the bounds of good clinical practice according to the ethical principles that have their origin in the Declaration of Helsinki in its current form. Written informed consent was obtained from all patients.
The data analysis was performed using Microsoft Office Excel® 2016.
Results
MRI localization
Sixty-three magnetic resonance tomography (MRI) examinations were performed on a total of 62 patients. One patient underwent two MRIs, one for the spine and one for the head. There were 20 MRI examinations in the area of the head as well as in the area of the spine. In 10 patients, an MRI of the pelvis was performed after implantation of the gliding nail, and in 6 cases, this was in the area of the lower extremity. Three patients received an MRI in the abdomen area, and four patients received an MRI in the thorax and upper extremity area.
Complications
Of the 62 patients, noneexperienced complications during the immediate examination. Similarly, none of the patients showed early complications within the first 2 weeks after MRI.
During our long-term follow-up examination in 2018, we were able to record 15 patients. Of these, noneshowed long-term complications after MRI.
Artifacts
Artifacts were found in 14 patients. These involved 10/10 pelvis MRI, 2/3 abdomen MRI, and 2/6 lower limb MRI. According to the five-point Likert-type scale (9, 10), we had 11/14 artifacts of category 1 (10/10 pelvis, 1/2 abdomen), 1/14 artifacts of category 2 (1/2 abdomen), and 2/14 artifacts of category 4 (2/2 lower limb).
All the other MRI scans could be categorized as category 5.
Discussion
As the population ages, medicine is constantly facing new challenges. Comprehensive therapies and the associated diagnostics have contributed to great progress in recent years. Diagnostic MRI in particular is becoming increasingly more important, and it is being used increasingly more frequently in the context of diagnostics.
For us, as orthopedic/trauma surgeons, the question therefore arose as to whether diagnostic MRI would have an effect on an implant that we had inserted and/or vice versa.
In our clinic, the gliding nail is used as an intramedullary implant for proximal femoral fractures, but the model and principle can also be applied to other intramedullary implants with the same composition of components.
The body of literature is small with respect to the effects of an MRI scan on the organism and the implant when the implant is inserted.
For example, Muranaka et al. found in the results of their experimental study, using an inserted implant at the hip joint, that there was a heating of the implant in their model. 3
The authors used two types of hip joint implants with a cobalt–chromium alloy and a titanium alloy. These were exposed to a magnetic field corresponding to a 1.5-T MRI in the gel model. The highest temperature increase was measured at the tip of each implant with 9°C for the cobalt–chromium alloy and 5.3°C for the titanium alloy. 3
Also, Ho demonstrated that local warming can occur around an inserted implant. 5
From further work, it is known that in individual cases skin burns can occur, for example, due to (adjacent) monitoring cables and probes. 1,11,12
Another important factor is a possible dislocation of an inserted implant. An implant cannot lose its function only as a result of an implant being dislocated from its intended location, it can also cause serious damage to the patient with the implant in this condition.
Hassepass et al. were able to show in the results of their study that magnetic dislocation can occur when MRI scans are performed on inserted cochlear implants. 2
In the present study, the question arose of whether a patient could feel something of this possible local warming of the implant or whether the MRT had acute or long-term effects on the inserted implant.
In our collective, of the 62 patients, none showed complications during the immediate examination and none complained of a feeling of warmth or local pain. Also, burning or local reaction could not be detected.
Similarly, of the 62 patients, none showed an early complication within the first 2 weeks after MRI.
In our long-term follow-up examination in 2018, of the 15 patients, none showed a long-term complication.
As early as 2016, Sammet propagated the importance of the knowledge and safe handling of MRI scans, implant, and patient and hence formulated some key points in this regard. For example, people working in the immediate field of diagnostic MRI diagnostics should receive intensive training in order to inform their patients correctly and prevent possible dangers. 13
A good image quality is essential for the diagnosis of the MRT and the correct diagnosis.
In our study, imaging artifacts were present in 14 of 63 MRI examinations whereby artifacts could be detected in all cases with imaging of the pelvis (10 of 10). In the case of abdomen, artifacts were found in two of the three cases and in the area of the lower extremity in two of the six cases (Figures 1(a) to (d) and 2(a) to (c)). Thus, it can be shown that image artifacts, predominantly on the ipsilateral side, can only be expected in the immediate vicinity of the inserted implant. All other regions were free of artifacts and a good image evaluation was possible.
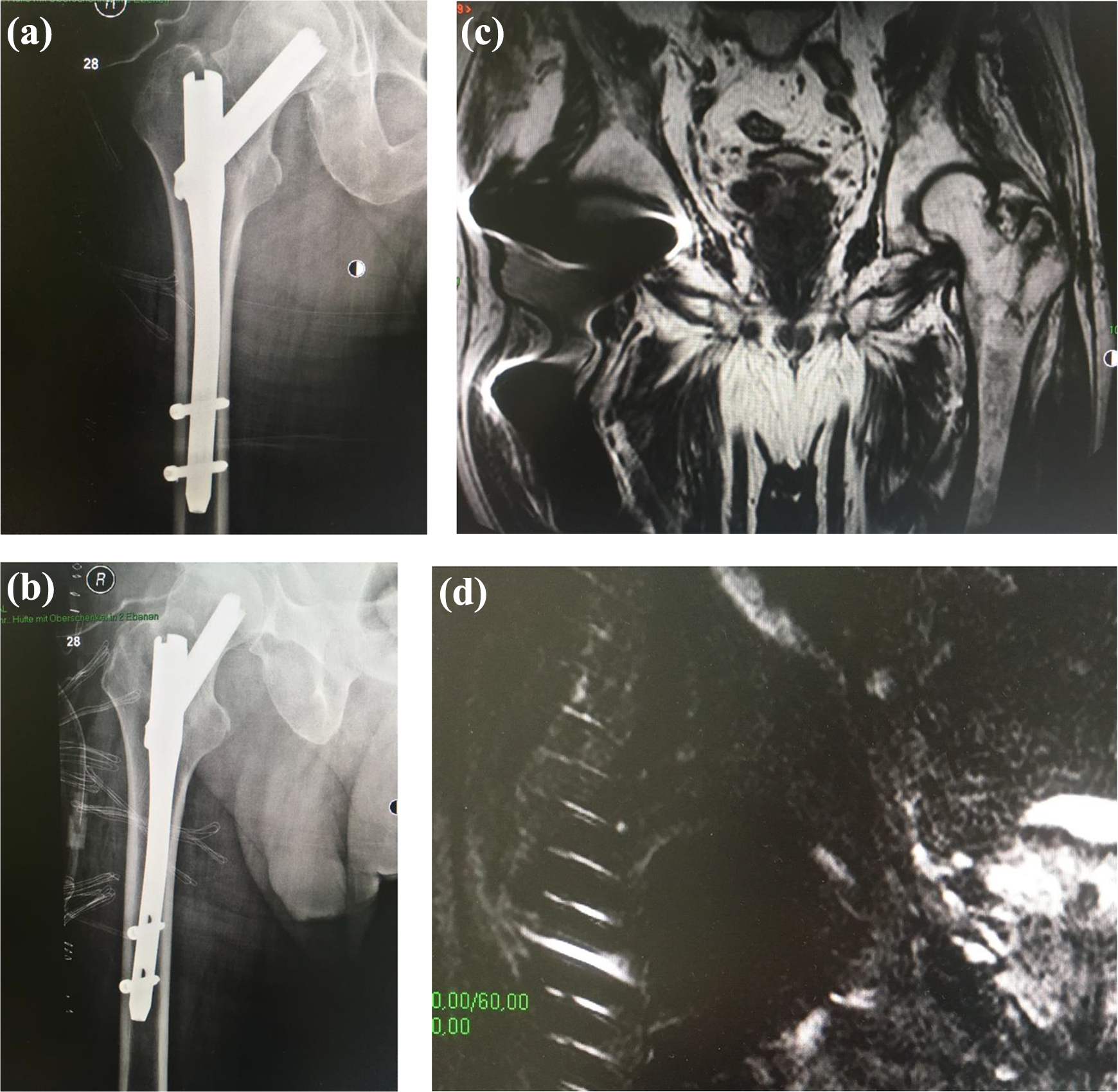
(a) GlidingNail X-ray ap. (b) GlidingNail X-ray axial. (c) Artifacts in an MRI of the pelvis with implanted gliding nail at the right side. (d) Local artifacts in an MRI of the pelvis with implanted gliding nail at the right side. MRI: magnetic resonance imaging.

(a) GlidingNail X-ray ap. (b) Artifacts in an MRI of the abdomen with implanted gliding nail at the right side. (c) Artifacts in the transversal images in an MRI of the pelvis with implanted gliding nail at the right side. MRI: magnetic resonance imaging.
A strength of this study lies in the standardized data collection and detailed documentation. Furthermore, using questionnaires, both short- and long-term results were assessed.
A limitation of this study is the relatively low number of patients. Furthermore, this is a single-center study with retrospective data, potentially limiting the study findings. Another limitation is the lack of a comparative collective of patients.
Conclusion
In relation to our patient collective, our work shows that no complications occurred both during the immediate examination and from the recorded long-term results. The MRI with an intramedullary nail in place allows a good image quality, as long as the immediate implant area is not imaged. MRI diagnostics is therefore also possible for patients with an inserted gliding nail. The intramedullary nail should therefore not be an exclusion criterion when sectional imaging with MRI is urgently required.
Footnotes
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: One of the authors, Prof. Dr. med. Dr. h.c. mult. Wilhelm Friedl, is the inventor of the gliding nail and works as a development consultant for Intercus GmbH.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.