
Abstract
We describe a rare case of sclerosing osteomyelitis of Garré in a 63-year-old woman with uncontrolled right thigh pain. She had suffered from lower back pain and radiating pain on the right lower leg for a year and 4 months and so had spine surgery 8 months ago. But the right thigh pain persisted, and the levels of C-reactive protein (CRP) and erythrocyte sedimentation rate (ESR) remained abnormal. Right femur radiographs showed cortical thickening on the proximal femur. Magnetic resonance images showed T2 hypersignal intensity lesions in the proximal femur. Under suspicion of osteoid osteoma or sclerosing osteomyelitis, surgery was performed with biopsy, bone curettage, and drilling. The culture was negative, and the biopsy showed chronic osteomyelitis. Despite surgery, the levels of CRP and ESR still remained abnormal. After using venous antibiotics, the pain subsided and CRP and ESR levels turned to normal. Followed by 6 weeks of oral antibiotics, pain was relieved after 1-year follow-up.
Introduction
Sclerosing osteomyelitis of Garré is a rare inflammatory disease of chronic nature characterized by thickening of the cortices and loss of the medullary canal. 1,2 It mainly affects young children and adults and the region of the mandible, but in rare cases, the metaphysis of long bones is affected. It is also known as Garré’s sclerosing osteomyelitis, chronic osteomyelitis with proliferative periostitis, ossifying periostitis, or nonsuppurative chronic sclerosing osteomyelitis. 3,4
The clinical feature is characterized by an insidious onset, localized pain with episodic nonprogressive nature. The duration is very variable, which may persist for several months or several years, and it can also affect multifocal sites. In general, the function of the affected bone is preserved. 5 The radiographic features include cortical thickening and loss of medullary canal. 2,6 Acute-phase inflammatory markers such as C-reactive protein (CRP) and erythrocyte sedimentation rate (ESR) may be elevated. 2 The biopsy shows chronic, nonspecific osteomyelitis, and both blood and tissue cultures are generally negative. The differential diagnoses include fibrous dysplasia, syphilis, pustulosis palmoplantaris, rectocolitis, Crohn’s disease, synovitis, acne, pustulosis, hyperostosis and osteitis (SAPHO), chronic recurrent multifocal osteomyelitis, Paget’s disease, osteoid osteoma, Ewing’s disease, osteosarcoma, and eosinophilic granuloma. 3,7,8
The goal of the treatment is symptom relief. Some patients respond to analgesics, and some respond to antibiotics although the exact mechanism is unclear. If symptoms are uncontrolled, surgical treatment can be considered including procedures ranging from debridement of the affected bone with exposure of the medullary canal to resection of the area of chronic osteomyelitis. 6,9 –11
Case
A 63-year-old woman suffered from uncontrolled right thigh pain. She had lower back pain and radiating pain on the right lower leg a year and 4 months earlier and had a spine surgery (lumbar spine 4–5, lumbar spine 5–sacrum 1 posterior interbody fusion) 8 months ago. Her lower back pain was relieved, but pain in the right thigh persisted. The CRP and ESR levels remained at abnormal at 1.13 and 95, respectively (normal ranges 0–0.6 mg/dl and 2–30mm/h, respectively). Lumbar spine magnetic resonance images showed no definite signs of infection. Blood and urine culture were negative. Rheumatologic laboratory tests were negative. Several conservative treatments, including epidural nerve block, did not work.
To rule out femur lesions, such as an atypical femur fracture, which is recently often diagnosed, right femur radiographs were taken. They showed lateral cortical thickening of the proximal femur and several radiolucent lesions inside (Figure 1). An isotope bone scan showed increased uptake in the lateral portion of the right proximal femur (Figure 2). The right femur MRI showed lateral cortical thickening of the proximal femur and T2 hypersignal intensity lesions inside (Figure 3).

Radiographs of the right thigh show lateral cortical thickening of the proximal femur and several radiolucent lesions inside.
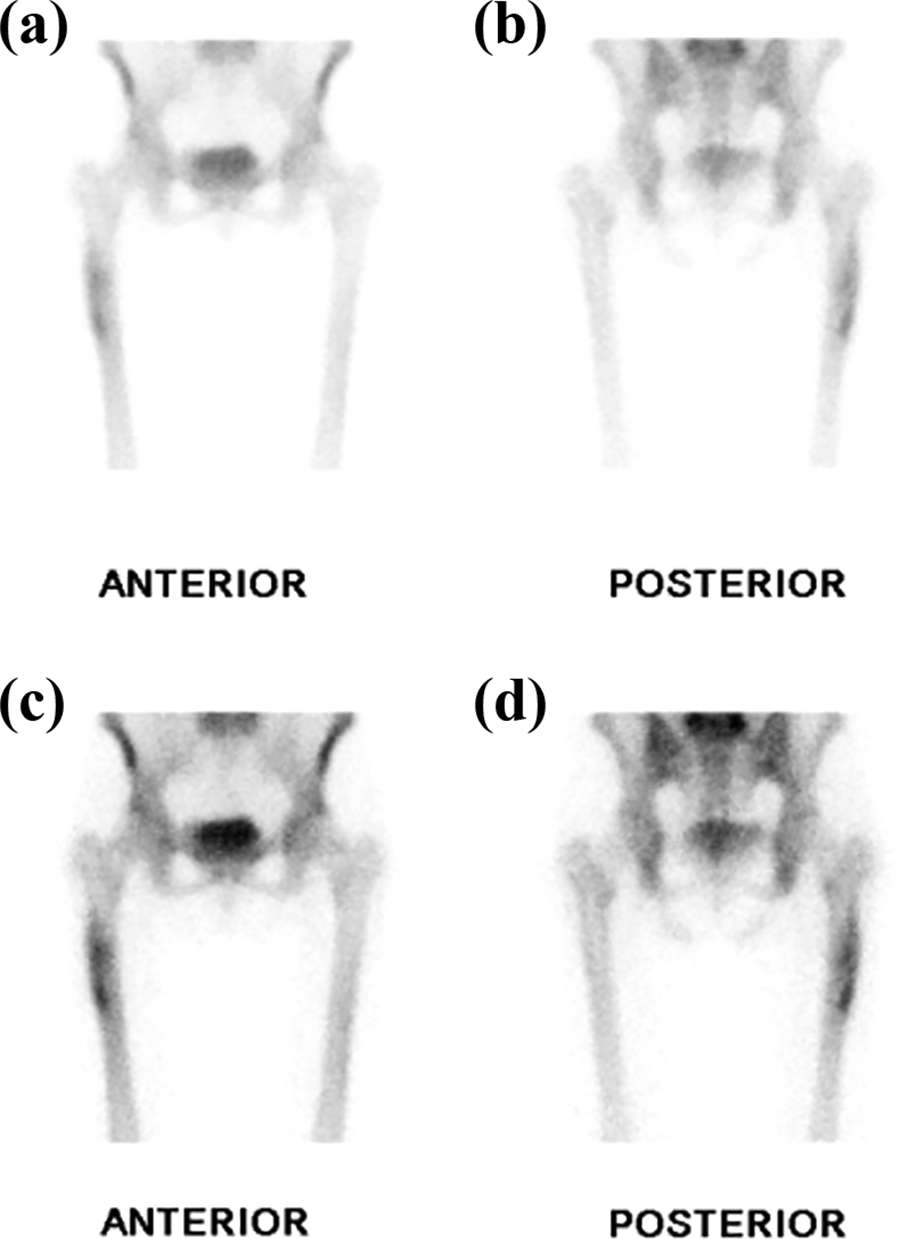
An isotope bone scan shows increased uptake in the lateral portion of the right proximal femur: (a, c) anterior and (b, d) posterior.

Right femur MRI shows lateral cortical thickening of the proximal femur and T2 hypersignal intensity lesions inside.
Under suspicion of osteoid osteoma, the patient was treated with aspirin. But aspirin did not relieve the pain. Therefore, to rule out sclerosing osteomyelitis, a biopsy, bone curettage, and drilling with exposure of the medullary canal were performed on the right proximal femur (Figure 4). Intraoperative findings revealed no destructive bone lesion or gross pus. The cultures were negative. The biopsy showed either chronic osteomyelitis or another infectious lesion, rather than a neoplastic lesion (Figure 5). The surgical pain became tolerable, but the CRP and ESR still remained slightly elevated at 1.31 and 89, respectively (normal ranges 0–0.6 mg/dl and 2–30mm/h, respectively). Because the histological studies were suggestive of an infection, we administered intravenous antibiotics (cefazoline, 3 g/day) and the pain improved dramatically. In addition, CRP and ESR levels turned to normal. Followed by 6 weeks of oral antibiotics (cephalexin, 3 g/day), pain was relieved after 1-year follow-up. And 1-year postoperative radiographs showed no progression of cortical thickening and healing of the drilling site (Figure 6).

Radiographs of the right femur after surgery with biopsy, bone curettage, and drilling with exposure of the medullary canal.

The biopsy shows either chronic osteomyelitis or another infectious lesion, rather than a neoplastic lesion, and was marked by sclerotic cortical bone fragments with fibrotic tissue and some inflammatory cells infiltrations in marrow space (hematoxylin–eosin stain): (a, left) ×100 magnification and (b, right) ×400 magnification.

Postoperative 1-year radiographs show no progression of cortical thickening and healing of the drilling site.
Discussion
Chronic sclerosing osteomyelitis was first described by Garré in 1893, which was characterized by thickening of cortices of long bones without abscess or sequestra. 4 It is very rare and difficult to diagnose, usually mentioned in sporadic case reports. The etiology is still unclear. It is suspected to be a bacterial infection, but cultures are generally negative and chronic conditions may be maintained through a low-virulence infection. 3 The anaerobic bacterium Propionibacterium acnes and fungal infections Actinomycosis naeslundii and Actinomyces israelii have been proposed as causative organisms. 12,13
Tumorous conditions with sclerosing bone reaction such as osteoid osteoma, Ewing’s disease, osteosarcoma, and eosinophilic granuloma should be excluded from the diagnosis. Additional differential diagnoses with multifocal sclerosing bone reaction are fibrous dysplasia, syphilis, pustulosis palmoplantaris, ulcerative rectocolitis, Crohn’s disease, SAPHO syndrome, and Paget’s disease. 3,7
The most appropriate treatment for this chronic condition remains unclear. Some patients respond to nonsteroidal anti-inflammatory drugs or analgesics and some respond to antibiotics. 14 –16 Kuijpers et al. reported clinical and symptomatic improvements with the use of bisphosphonates in diffuse sclerosing osteomyelitis of the mandible. 17 If the symptoms are uncontrollable, surgical treatment should be considered. First, fenestration and curettage of the affected site can be performed. 18 Collert et al. reported successful treatment outcomes of eight patients with intramedullary reaming of long bones. 5 Nicola et al. treated recurrent sclerosing osteomyelitis of femur with intramedullary nailing, achieving good clinical outcome. 18 Nikomarov et al. reported bone resection and transport using a circular external fixator with good functional result in a 15-year-old girl. 19
In our case, the patient had a history of spinal stenosis and consequent spine surgery. Therefore, the origin of the right thigh pain was thought to be the radiating pain from lumbar radiculopathy and that delayed the study of the right thigh. Even after a thorough workup, simple tumorous conditions, such as osteoid osteoma, could not be excluded. We considered image-guided needle biopsy, but we suspected osteoid osteoma, and needle biopsy would not be sufficient for getting tissue of suspected lesions of nidus. So a simple surgical treatment with biopsy and drilling was performed. Bone curettage and drilling relieved symptoms somewhat. And antibiotics were very effective, although the exact mechanism is unclear in the face of negative cultures.
We administered first-generation cephalosporins, cefazolin and cephalexin, for 1 and 6 weeks, respectively, but the use of antibiotics is open to discussion. Although pain was relieved at the 1-year follow-up in this patient, careful observation for symptom recurrence is needed. We recommended the patient to take follow-up MRIs, but in our case report, the patient did not wish to partake, as she was symptom-free and also could not afford the costs of MRIs.
Sclerosing osteomyelitis of Garré is very rare, confusing to diagnose, and its symptom control is difficult. Bone curettage and drilling with biopsy and the use of antibiotics could be considered as treatment options.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.