
Abstract
Purpose:
To present transversal data (demographic and clinical) on isolated humeral shaft fractures (HSFs) in Latin American countries.
Methods:
Patients were enrolled between December 2015 and April 2017 at 11 medical institutions from six Latin America countries.
Inclusion criteria:
Age ≥18 years and a closed, isolated 12A, 12B, or 12C fracture (Arbeitsgemeinschaft für Osteosynthesefragen/Orthopaedic Trauma Association (AO/OTA) classification). The patients’ demographic, comorbidity, and other baseline data were recorded. The outcome measures included the basal results of the research and the associations among the demographic factors, fracture features, and type of treatment applied.
Results:
A total of 123 patients were included. There was a preponderance of men (61.8%), whose mean age was significantly lower than that of the women (31.48 vs. 60.55). Overweight or obesity was present in 61.0% of women; 56.1% of patients were sedentary, 75.6% were nonsmokers, and 74.0% had no chronic disease. The type or treatment (operative/nonoperative) was not significantly associated with the patient’s or fracture’s characteristics. Falls and traffic accidents were the main causes of HSFs. Intramedullary nailing treatment was performed significantly more often in women, elderly patients, patients who did not participate in sports, and patients participating in only home activities. Minimally invasive plate osteosynthesis was performed significantly more frequently in men and in those who were self-employed. Open reduction internal fixation was performed significantly more often when the cause of the fracture was a traffic accident and when radial nerve palsy was present.
Conclusion:
The demographics and etiological differences observed in comparison to the current literature show the importance of regional studies for both preventive measures and educational guidance.
Introduction
Humeral shaft fractures (HSFs) account for 13-25% of all humeral fractures. 1 –4 Epidemiological studies on this topic are scarce. 2 –10 In the PubMed database, a search through September 2018 listed 254,539 references for “multicenter” “studies.” Adding “Latin” “America” “fracture,” we found nine studies. One referred to a recent survey about radial nerve palsy in HSFs, 11 six dealt with osteoporosis and spinal cord injuries, and three with other topics. Epidemiological data could be relevant to support and guide educational and training programs, improve patient care, and reduce complications. The main objective of this article is to present transversal data (demographic and clinical) on isolated HSFs. The specific objectives are to present data on the distributions of age, sex, causes, types, locations, and treatment types of isolated HSFs from a sample from Latin American countries. The associations among the demographic factors, fracture features, and the type of treatment applied will be determined.
The treatment outcome data will be presented in a future paper.
Materials and methods
Registration and ethics
Ethical approval was obtained from all local authorities. The study was conducted according to the ethical principles outlined in the Declaration of Helsinki and based on the laws and regulations of the individual countries in which the research was conducted. The Institutional Review Board, located at Unicamp College of Medical Sciences, Campinas, Sao Paulo, Brazil, approved the project with the following identifier: CAAE Approval 1.142.071, July 2, 2015. All the patients or their legally authorized representatives have given their written informed consent for the article to be published.
Study design
The principal investigator led a research group of orthopedic surgeons from various countries, who participated in AO Trauma Latin America (AOTLA).
This study enrolled patients between December 2015 and April 2017 at 11 medical institutions from six Latin American countries: Argentina (n = 1), Brazil (n = 4), Colombia (n = 2), Guatemala (n = 1), Uruguay (n = 1), and Venezuela (n = 2). Among the 11 participating institutions, 10 were dedicated to public patients (5 were university hospitals) and 1 was a military hospital. The web-based electronic data capture system was sponsored by AOTLA.
Inclusion criteria
Age ≥18 years; the presence of a closed, isolated 12A, 12B, or 12C fracture (AO/OTA classification) confirmed by radiographic evaluation; fracture treatment initiated within 20 days after injury without previous treatment; patient’s ability to understand and sign the informed consent form (or be represented by a legally authorized person who could do so); and patient’s agreement to participate in the study according to the study protocol. All subjects were recruited from emergency departments by the participating authors at their respective workplaces.
Exclusion criteria
The presence of an articular fracture with diaphysis extension; open fracture, multiple fractures, or pathological fractures; neurological and/or psychiatric disorders; limited freedom (e.g. in prison), previous implant in the fractured limb; fractures whose treatment was initiated three or more weeks after injury.
Intervention
Patients underwent treatment according to the standard practice of the individual clinics. The treatment was chosen according to the routine treatment protocol at the clinic and the treating surgeon’s preference. Postoperative care was carried out according to the standard practice of the institution.
Data collection
Each surgeon previously registered with their assigned log-in and password credentials to be able to add to the patients’ records. Each patient received a number to ensure that the data remained anonymous.
Age, sex, body mass index (BMI), occupational status (self-employed or employed in the private or public sector), home activities, level of education, participation (or not) in regular sports activities, chronic diseases, smoking, alcoholism, and the use of illicit drugs were documented.
Fracture data, including date of occurrence, date of treatment, AO/OTA classification, fracture level, and the presence of primary radial nerve palsy, were recorded. Each fracture was classified only by the orthopedic surgeon who treated the case and the classification was not changed later. The trauma mechanism was classified as a simple fall, meaning a fall from a person’s height; a traffic-related accident (car, motorcycle, or bicycle accident or being run over); a sports-related injury; or another cause.
Treatment
The treatment (nonoperative or operative) was selected by the attending physician at each hospital and was based on the surgeon’s best judgment, knowledge, and expertise. The operative treatment options included minimally invasive plate osteosynthesis (MIPO), closed reduction and fixation with a locked intramedullary nail (NAIL), and open reduction and internal fixation with a plate (ORIF).
Outcome measures
The outcome measures include the basal results of the research and the associations among the demographic factors, fracture features, and the type of treatment applied.
Statistical analysis
The demographic data and data related to the fracture are presented according to the type of treatment. Data were analyzed using the χ 2 test or Fisher’s exact test when n < 5. Student’s t-test was used to compare the patients by age. All results were considered significant at p < 0.05. The statistical software used was SPSS 15.0 for Windows (SPPS Inc., Chicago, Illinois, USA).
Results
Altogether, 138 patients were enrolled between December 01, 2015, and April 02, 2017: 2 were excluded because they were under 18, 8 refused to participate, and 5 lost the follow up, leaving the final study group with 123 patients. The final contributions of each country in the series were as follows: Brazil (n = 43), Guatemala (n = 22), Venezuela (n = 22), Argentina (n = 20), Colombia (n = 12), and Uruguay (n = 4).
Figure 1 shows the distribution of cases according to the patients’ sex and age. There was a preponderance of men (61.8%), whose mean age was significantly lower than that of the women (31.48 ± 11.71 vs. 60.55 ± 19.42; p = 0.00).
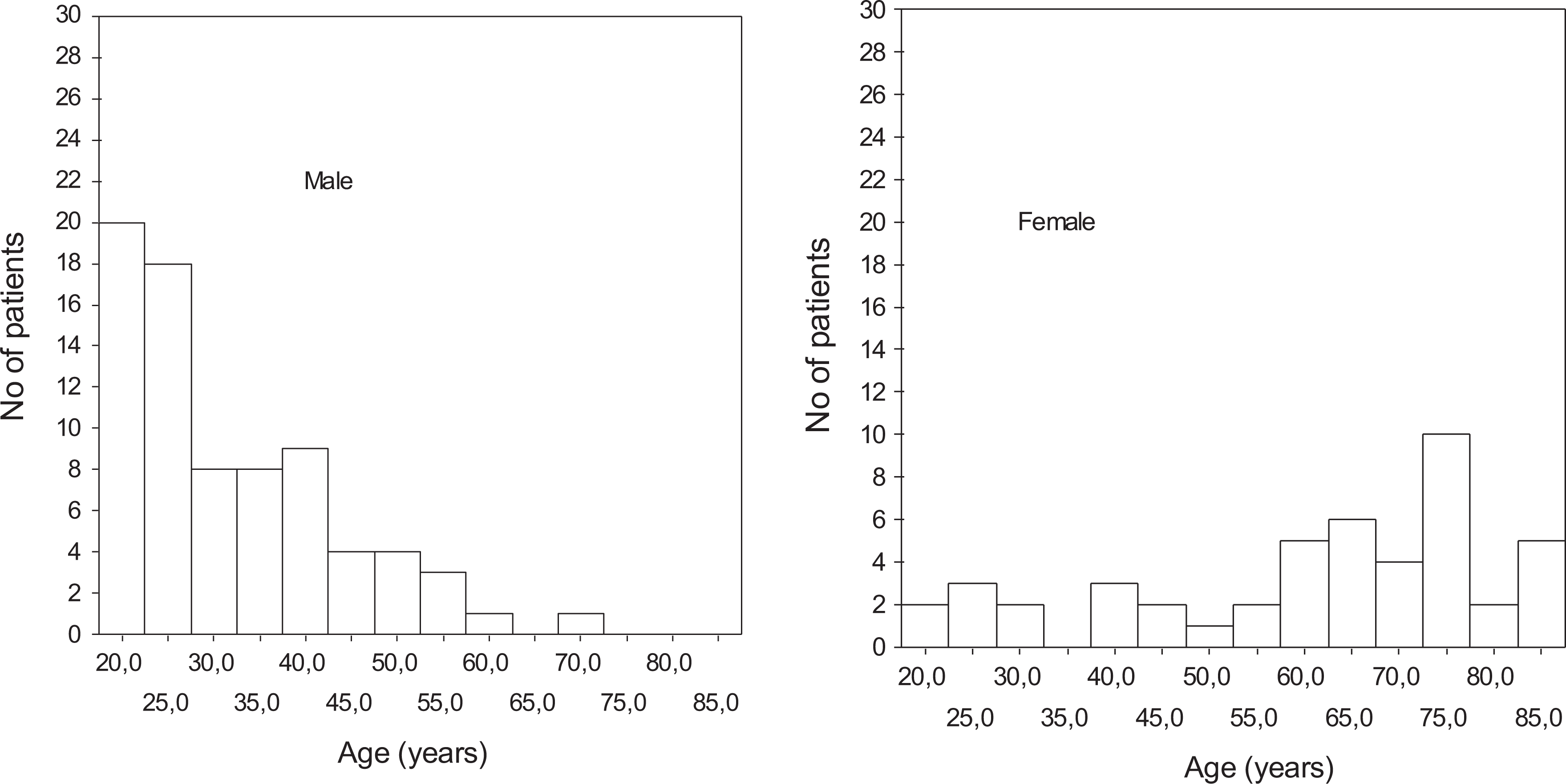
Histogram of the age distribution of the male and female patients.
Table 1 shows that there was a preponderance of patients with low education levels (84.6%) and patients who were overweight or obese (61.0%). The distribution among the occupational categories was almost homogeneous, with the lowest percentage of patients in the private sector category. In all, 56.1% of the patients did not participate in regular physical activity. There was a low frequency of patients who smoked (24.4%) or who had a chronic disease (26.0%). The choice of treatment type (operative/nonoperative) had no significant association with the patients’ sex, age-group, educational level, BMI, smoking status, or the presence of chronic disease. There was a significantly higher prevalence of overweight and obese women than of overweight and obese men (p = 0.02; Figure 2).
Demographic and clinical factors of the group of 123 patients with humeral shaft fractures according to the type of treatment (operative vs. nonoperative).
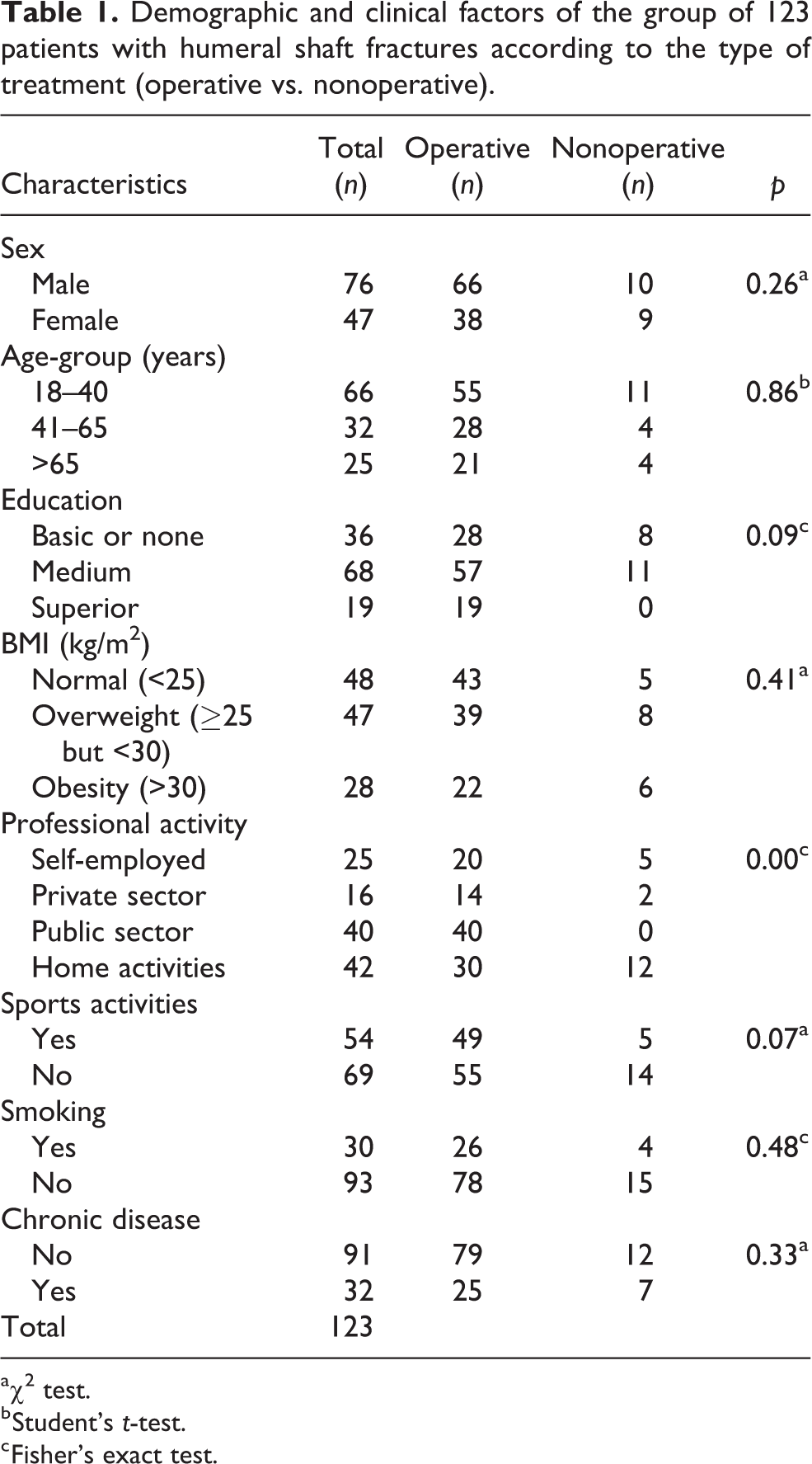
aχ2 test.
b Student’s t-test.
c Fisher’s exact test.

BMI values according to age and sex. Horizontal line inside the figure represents maximum normal value and vertical lines reflect the age groups (18–40 years; 41–65 years; >65 years). Circles represent women and triangles represent men. BMI: body mass index.
Table 2 shows that falls (44.7%) and traffic accidents (43.1%) were responsible for a similar proportion of the fractures and were the main causes of fractures. Most of the fractures occurred at the middle level (65.9%) were type A and transverse (A3). The type of treatment (operative or nonoperative) was not significantly different in relation to the cause of the fracture, the AO/OTA classification, or the fracture level. The NAIL treatment, however, was applied significantly more often in older patients (Figure 3). Among the 11 patients with primary radial nerve palsy, 10 patients received surgical treatment for the fracture.
Fracture-related factors of the 123 humeral shaft fractures according to the type of treatment.

a Fisher’s exact test.
bχ2 test.

Box-plot of the ages of the patients according the type of treatment. From bottom to top: minimum value, first quartile, median, third quartile, and maximum value. NO-OP: no operation; NAIL: closed reduction and fixation with a locked intramedullary nail; MIPO: minimally invasive plate osteosynthesis; ORIF: open reduction and internal fixation.
Table 3 presents the associations between demographic and clinical data and the types of surgical treatment (MIPO, NAIL, and ORIF). The frequency of the three types of surgical treatments was not significantly different (p = 0.12).
Associations among demographic and clinical data and the types of surgical treatment.

aχ2 test.
b Fisher’s exact test.
Considering only the surgical treatments, NAIL was performed significantly more often in women (p = 0.00), elderly patients (p = 0.00), those who did not participate in sports (p = 0.00), and those carrying out only home activities (p = 0.00). MIPO was performed significantly more frequently in men (p = 0.00) and in those who were self-employed (p = 0.04). ORIF was undertaken significantly more often when the cause of the fracture was a traffic accident (p = 0.00) and when radial nerve palsy was present (p = 0.01).
Nonsurgical treatment was undertaken significantly more often in patients who were obese, those carrying out only home activities, those who did not participate in regular sports activities, nonsmokers, and those without a chronic disease (Table 4).
Associations among demographic and clinical data and nonoperative treatment.

a Fisher’s exact test.
bχ2 test.
Table 5 shows that Radial nerve palsy (RNP) was significantly more frequent in younger persons (age-group 18–40 years; p = 0.00) and when traffic accidents caused the fracture (p = 0.04), the patient’s sex, AO classification, and fracture level were not significantly associated with RNP.
Demographic and clinical factors associated with radial nerve palsy.

Discussion
The percentage of HSFs is not high, accounting for only 13–25% of all humeral fractures, thereby justifying the small number of patients included in most of the studies in the literature. 4,6,9,10 Except for a study published in 2016, 5 the present casuistic is in agreement with the previous studies related to humeral fractures.
Epidemiological data on HSFs are infrequent in the literature, and most of them have been retrospective. 2,4 –6,8 –10 The most referenced epidemiological study was performed in Sweden in 2006. 3 Those authors found a bimodal distribution with respect to age and sex, with a shorter peak around the third decade in men and a taller peak during the seventh decade in women. The main trauma mechanism was falls (67.2%), with traffic accidents being the cause of only 7.7% of humeral fractures. In 2017, the same group published an update with similar results. 5 In the present study, the distribution by sex was opposite, with a taller peak in the 20s for men and a shorter peak in the 60s for women (Figure 1), and traffic accidents—motorcycle, car, bicycle, and pedestrian accidents (41.42%)—were responsible for a proportion of HSFs similar to that associated with falls (44.71%). Other studies also found falls to be the principal cause of HSFs. 1,2,7 Sweden has one of the lowest rates of car accidents in the world, which may represent a bias when its sample is compared with that of other countries. According to the latest data released by the World Health Organization, 12 in 2016, Sweden had an estimated road traffic death rate of 2.8 per 100,000 inhabitants, whereas in Argentina, it was 14.0, in Brazil, it was 19.7, in Colombia, it was 18.5, in Guatemala, it was 16.6, in Uruguay, it was 13.4, and in Venezuela, it was 33.7.
Indeed, the higher incidence of HSFs in men in their 20s was due to the high incidence of traffic accidents and represents a severe public health problem in Latin America. This finding has enormous implications for future preventive and educational measures regarding HSFs. The frequency of sports-related HSFs was small and similar to that reported in other studies. 5,7 –9
The factors that were associated with being female—less regular participation in sports, higher prevalence of being overweight/obese, and falling as the principal trauma mechanism—in some ways reflect the less favorable social position of girls and women in developing countries. 13,14 Hallal et al. 15 reported that some Latin American countries are among those with a higher proportion of sedentary people in the world, with more than 40% of those >15 years of age classified as inactive. Additionally, the prevalence of obesity in Latin America is among the highest in the world. 14
In this study, surgery was the most common treatment option, although it has also been accepted that isolated HSFs can be successfully treated nonsurgically. 1,16 –18 The principal decision-making factors associated with choosing surgical treatment were sex, age, occupational status, presence of RNP, and a traffic accident as the cause of the fracture. Known factors that could influence the treatment choice—trauma mechanism, fracture type, and fracture location—were not statistically significant in terms of the decision to perform nonoperative or operative treatment. Furthermore, according to recent publications, 16 –19 nonunion is more frequent following conservative treatment, supporting the tendency toward choosing surgical treatment for this type of fracture.
MIPO (n = 41) and ORIF (n = 38) were the preferred surgical treatments, which are in agreement with a recent meta-analysis of HSFs according to which MIPO was the preferred treatment. 19 NAIL technique was indicated mainly for women (21/25) and the home activities group (33/42). The known preference for NAIL for osteoporotic fractures could justify, at least partially, the frequency of its use in women, as observed in the current study. 20 RNP was associated with ORIF, suggesting that more severe trauma may have influenced the decision to perform this technique, although this concept falls short of scientific support.
The literature recommends that HSFs with primary RNP be addressed via nonoperative treatment. 21,22 In a recent survey, however, an operative procedure was the first choice in Latin America and Asia. 11 This option was confirmed in this study, in which most (10/11) of the patients with RNP were treated surgically.
Most of the patients treated via ORIF or MIPO were young men, in public jobs, and regularly engaged in sports activities, requiring faster rehabilitation. In a recent publication that compared MIPO with conservative treatment, MIPO was superior in all aspects, especially regarding the rehabilitation time and the Murley–Constant score. 23 The high frequency of cases treated by MIPO can also be justified because it was first described in Latin America 24 and its popularity spread quickly in this region and around the world. 25,26
One limitation of this study is the underrepresentation of the Latin American countries (six countries among more than two dozen). Another limitation is the small number of patients included by country in proportion to their population. These problems can be justified by the lack of the tradition of epidemiological studies in our region and the unfavorable conditions for research in many workplaces. Obtaining ethics committees’ approval was very difficult for almost all centers. Many institutions did not have a proper ethics committee, took too long for analysis, or had different legal processes—all markedly hampering project development. This obstacle particularly impacted the number of cases included by Uruguay. Although the patient enrollment for the study has started in December 2015, the Uruguayan center only managed to get ethical approval about a year later.
The major strengths are its prospective design, its pioneering objective of addressing a little-explored topic in the literature, and its conduction in Latin America.
Conclusion
The differences between our results and the literature show the importance of regional studies to provide background for the planning of preventive measures and to educate population and health services.
The experience should encourage more robust studies.
Footnotes
Acknowledgement
The authors acknowledged the support by the AO Trauma Latin America Board.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the AO Trauma Latin America Board.