
Abstract
Purpose:
The aim of this study was to evaluate the relationship between soft tissue laxity and kinematics of the normal knee using a navigation system.
Methods:
Fifteen cadaveric knees from 11 fresh frozen whole-body specimens were included in this study. The navigation system automatically recorded the rotation angle of the tibia as the internal–external (IE) kinematics and the coronal alignment of the lower limb as the varus–valgus (VV) kinematics. These measurements were made with the joint in maximal extension, at 10° intervals from 0° to 120° of flexion, and at maximal flexion during passive knee motion. For evaluation of laxity, the examiner gently applied maximum manual IE and VV stress to the knee at 0°, 30°, 60°, and 90° of flexion.
Results:
The measurements showed almost perfect reliability. The mean correlation coefficient between the intraoperative tibial rotation angle and the intermediate angle of IE laxity was 0.82, while that between the coronal alignment of the lower limb and the intermediate angle of the VV laxity was 0.96. There was a statistically significant correlation between kinematics and laxity at all degrees of knee flexion.
Conclusion:
The present study revealed that the rotation angle of the tibia was correlated to the intermediate angle of IE laxity at 0°, 30°, 60°, and 90° of knee flexion and the coronal alignment of the lower limb also correlated to the intermediate angle of VV laxity. These findings provide important reference data on soft tissue laxity and kinematics of the normal knee.
Introduction
Total knee arthroplasty (TKA) is a valuable and beneficial surgical alternative used to treat pain, disability, and limited motion associated with osteoarthritis. Although previous studies have indicated good long-term outcomes, 1,2 patients have reported being less satisfied with the outcomes of TKA than those after total hip arthroplasty. 3 This dissatisfaction could be explained partly by the changes in kinematics after TKA. 4,5 Nishio et al. reported that intraoperative medial pivot kinematics with external rotation of the femur relative to the tibia resulted in larger flexion angles and better patient-reported outcomes 6 and stated that restoring more normal and predictable kinematics possibly improved both knee flexion angle and subjective outcomes after TKA.
To restore the normal knee kinematics after TKA, considerable research concerning the surgical technique has been performed. In some previous reports, the relationship between intraoperative soft tissue balancing and postoperative kinematics was evaluated. 7 However, Ferle et al. stated that there were no objective target parameters describing the soft tissue tension of the normal knee and revealed that normal knee laxity was dependent on the flexion angle, using a meta-analysis of the data from previous studies on normal knee laxity. 8 Therefore, to create a guide for restoring normal knee kinematics after TKA, it is necessary to investigate the relationship between soft tissue laxity and kinematics in the normal knee in detail.
The aim of this cadaveric study was to evaluate the relationship between the soft tissue laxity and kinematics in the normal knee using a navigation system.
Materials and methods
We evaluated 15 cadaveric knees from 11 fresh frozen specimens stored at −20°C (six male, five female; mean age at the time of death 82.8 years, range 70–96 years). All the cadaveric specimens were macroscopically intact without gross deformity, arthritic changes, contracture, or evidence of prior knee surgery. Preoperative computed tomography confirmed that none had osteoarthritis. An image-free knee navigation system (Stryker Navigation version 1.0, Stryker, Kalamazoo, Michigan, USA), infrared cameras, and light-emitting diodes were used to evaluate the kinematics and laxity of the knee.
The knee joint was dissected in each cadaveric specimen using the standard medial parapatellar approach. Soft tissue release was not performed. The navigation system was registered for each case according to the manufacturer’s protocol. The femoral rotational axis was set as the surgical epicondylar axis. The tibial rotational axis was directed along a line from the medial edge of the attachment of the patellar tendon to the middle of the posterior cruciate ligament. 9 Intraoperative kinematic analysis was performed once for each knee by a single examiner using the navigation system after registration. The navigation system automatically recorded the angle of rotation of the tibia (internal rotation as positive) as internal–external (IE) kinematics. The system also recorded coronal alignment of the lower limb (varus alignment as positive) as the varus–valgus (VV) kinematics, at maximum extension, at 10° intervals from 0° to 120° of flexion, and at maximum flexion, during passive knee motion. An earlier study demonstrated that the repeatability and reproducibility of this methodology was statistically sufficient. 10 After the intraoperative kinematic analysis, the laxity of the knee joint was evaluated twice by a different examiner using the navigation system. For IE laxity, the examiner gently applied maximum manual internal and external stress to the knee at 0°, 30°, 60°, and 90° of flexion. The navigation system automatically recorded the rotation angle of the tibia at each knee angle. For VV laxity, the examiner applied maximum manual varus and valgus stress to the knee at 0°, 30°, 60°, and 90° of flexion. The coronal alignment of the lower limb was measured at each angle. The dissected fascia was sutured with nylon thread during the intraoperative evaluation of kinematics and laxity.
The institutional review board of our hospital approved this prospective study (No. 2068). All procedures involving human participants were conducted in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Declaration of Helsinki and its later amendments or comparable ethical standards. Written informed consent was obtained from all individual participants included in the study.
Statistical analysis
The statistical analysis was performed using IBM SPSS statistical software (SPSS v.21.0 for Mac OS X; IBM Corp., Armonk, New York, USA). Intraclass correlation coefficients (ICCs) were used to evaluate the intra-examiner reproducibility of measurements of IE and VV laxity. Pearson’s product correlation coefficients for the intraoperative tibial rotation angle and the intermediate angle of IE laxity were assessed at 0°, 30°, 60°, and 90° of knee flexion. The correlation coefficients for the intraoperative coronal alignment of the lower limb and the intermediate angle of VV laxity were also assessed at 0°, 30°, 60°, and 90° of knee flexion. The value of p < 0.05 was considered statistically significant. Given the small number of subjects, a post hoc calculation of statistical power was performed using G*power statistical software (version 3.1.9.2, Dusseldorf, Germany). A sample size calculation based on the calculated correlation coefficient demonstrated that nine specimens would be sufficient to detect statistically significant kinematic differences with a power of 0.8.
Results
The mean intra-rater ICC for IE laxity was 0.99 (range 0.97–0.99), and the mean intra-rater ICC for VV laxity was 0.99 (range 0.98–0.99). All measurements showed almost perfect reliability (Table 1).
Intra-rater intraclass coefficients for internal–external tibial rotation and varus–valgus laxity.

The results for the internal rotation angle of the tibia and the coronal alignment of the lower limb during knee flexion are summarized in Figures 1 and 2. The IE kinematics indicated sharp internal rotation of the tibia in the early stage of knee flexion and mild internal rotation of the tibia from 60° to maximum knee flexion. The VV kinematics showed mild changes in varus until 60° of knee flexion and in valgus over 70° of knee flexion.

Angle of internal rotation of the tibia during knee flexion. Error bars indicate standard error.
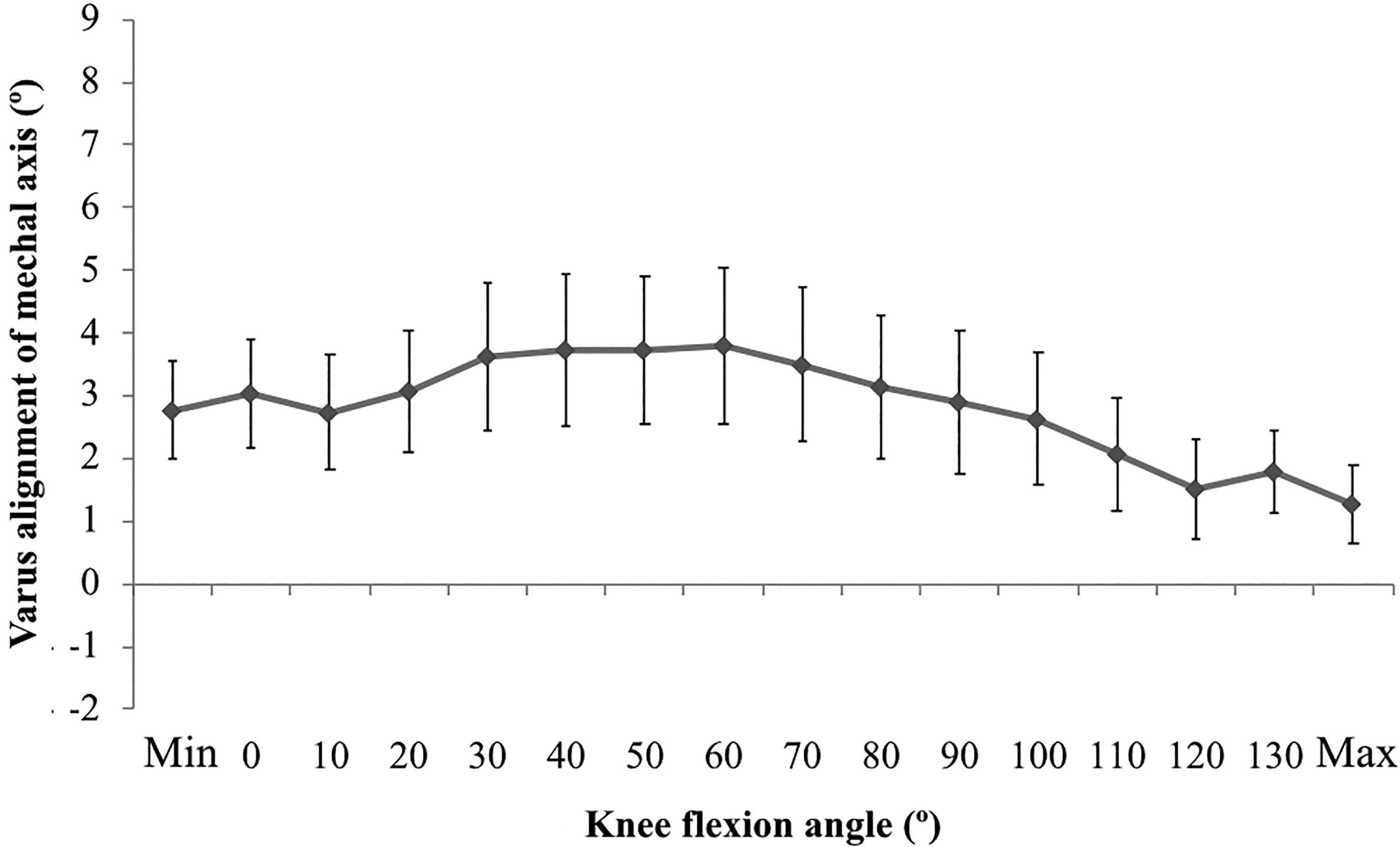
Coronal alignment of the lower limb during knee flexion. Error bars indicate standard error.
Correlation coefficients for kinematics and laxity during flexion of the knee are summarized in Figures 3 and 4. The mean correlation coefficient for the rotation angle of the tibia and the intermediate angle of IE laxity was 0.82, while the mean correlation coefficient for the coronal alignment of the lower limb and the intermediate angle of VV laxity was 0.96. There was a statistically significant correlation between kinematics and laxity at each angle of knee flexion (Table 2).

Comparison of the tibial internal rotation and mean angle of IE laxity. Cross mark indicates the intermediate angle of IE laxity. Error bars indicate the range of IE laxity. IE: internal–external.

Comparison of the coronal alignment of lower limb and the mean angle of VV laxity. Cross mark indicates the intermediate angle of VV laxity. Error bars indicate the range of VV laxity. VV: varus–valgus.
Correlation coefficients for kinematics and laxity during knee flexion.
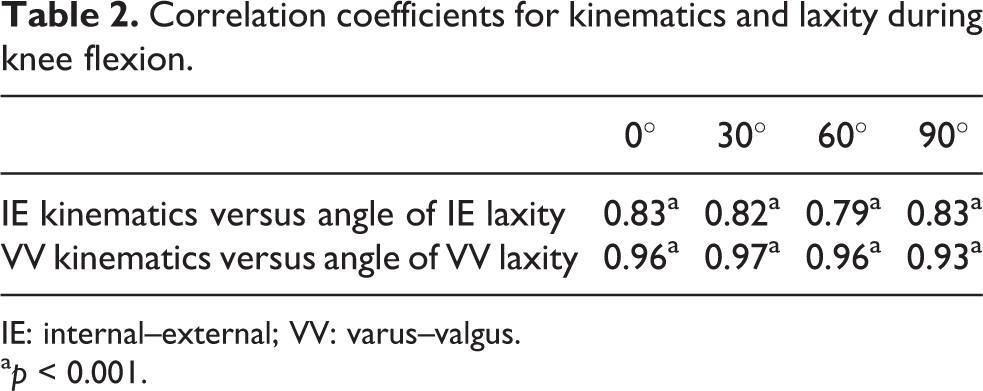
IE: internal–external; VV: varus–valgus.
a p < 0.001.
Discussion
The most important finding of this study was a statistically significant correlation between kinematics and laxity at 0°, 30°, 60°, and 90° of knee flexion. The present data suggested that both the rotation angle of the tibia and the coronal alignment of the lower limb might be similar to the intermediate angle of laxity at each knee flexion angle. To the best of our knowledge, this whole-body cadaveric study is the first to report on the relationship between kinematics and laxity in the normal knee using a navigation system. These findings provide important reference data on soft tissue laxity and kinematics of the normal knee.
Manual stress testing during intraoperative measurement of laxity using a navigation system has been used mainly in studies of knees with anterior cruciate ligament (ACL) injury. Miura et al. reported that evaluation of laxity in the contralateral stable knee is useful during reconstruction of a knee with ACL injury. 11 Martelli et al. demonstrated that this method has acceptable reliability. 12,13 Similarly, the intra-observer reliability for most measurements was almost perfect in the present study despite the use of manual stress testing.
The kinematics of the normal knee has been widely investigated, 14,15 and several movements unique to the normal knee have been reported in terms of axial rotation. Sharp external rotation of the femur near extension has been identified and is known as the “screw-home” movement. 16,17 Bicondylar rollback has also been found to occur at mid-flexion during various activities 18 and a medial pivot motion has been identified during deep knee bends. 19,20 In the present study, IE kinematics data indicate that sharp internal rotation of the tibia occurs in the early stage of knee flexion and that mild internal rotation of the tibia occurs between 60° and maximum flexion of the knee. The present data of cadaveric knees are similar to those in previous kinematics studies, possibly because we evaluated the kinematics of the normal knee in whole-body cadaveric specimens. In terms of VV kinematics, the present data were also similar to those of a previous cadaveric study by Siston et al. using a navigation system. 21 However, there were some discrepancies in comparison with previous in vivo kinematic results. 15,22 These discrepancies may be due to a difference in the reference point of the axis. Further research is necessary to identify the reason for the discrepancies in kinematic measurements.
The relationship between soft tissue laxity and kinematics in TKA has been studied. Watanabe et al. evaluated soft tissue balance using a tensor device in posterior-stabilized TKA and concluded that the intraoperative joint gap in deep flexion and soft tissue balance play important roles in kinematics after TKA. 23 Matsuzaki et al. evaluated the influence of intraoperative soft tissue balance parameters on knee kinematics in cruciate-retaining TKA and reported that lateral laxity at mid-to-deep knee flexion plays a significant role in internal rotation of the tibia. 24 Furthermore, it has also been reported that several factors affect both soft tissue laxity and kinematics. Wada et al. conducted a cadaveric study and revealed that tibial internal rotation during knee flexion was reduced by extensive medial collateral ligament release in posterior-stabilized TKA. 7 According to Matsumoto et al., kinematically aligned cruciate retaining TKA maintained more tibial internal rotation and lateral laxity during flexion than mechanically aligned TKA. 25 Even though meticulous TKA studies have been conducted, it is necessary to understand the relationship between the soft tissue laxity and kinematics in normal knee. In this study, the rotation angle of the tibia was correlated to the intermediate angle of IE laxity at 0°, 30°, 60°, and 90° of knee flexion, and the coronal alignment of the lower limb also correlated to the intermediate angle of VV laxity. The present results would be important data for further assessment of the knee laxity and kinematics.
This study had several limitations. First, we assessed only the rotation angle of the tibia and the coronal alignment of the lower limb. There is a lack of kinematic data for the anteroposterior, mediolateral, and superoinferior dimensions because the kinematics of the knee includes six degrees of freedom. Anteroposterior translation should be examined to evaluate the kinematics of knee flexion but could not be assessed by our navigation system. Second, the reproducibility of the kinematic analysis was not evaluated; this may be questionable because the analysis was performed manually. Nevertheless, in a previous study, Wada et al. demonstrated that intraoperative analysis of kinematics was highly reproducible. 10 Therefore, we believe that our present data, which were obtained using the same method, have acceptable reproducibility. Third, the mean age of knees included in this study is 82.8 years, which is relatively old for studies of normal knees. In the present study, all the cadaveric specimens were evaluated as macroscopically intact and preoperative computed tomography confirmed that none had osteoarthritis. Thus, these knees seem to be suitable to be evaluated as normal knees.
Conclusion
The present study revealed that the rotation angle of the tibia was correlated to the intermediate angle of IE laxity at 0°, 30°, 60°, and 90° of knee flexion and the coronal alignment of the lower limb also correlated to the intermediate angle of VV laxity. These findings provide important reference data on soft tissue laxity and kinematics of the normal knee.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and publication of this article.