
Abstract
Purpose:
The purpose of this article is to investigate the outcomes after anterior cervical discectomy and fusion (ACDF) surgery with stand-alone tricortical iliac crest autograft and to determine predictive factors for poor neurological recovery, non-union, graft collapse and loss of C2–C7 sagittal alignment.
Methods:
This was a retrospective study involving patients with cervical myelopathy who underwent ACDF surgery with stand-alone tricortical iliac autograft between 2006 and 2016, with a minimum 2-year postoperative follow-up. Outcomes included the change in Japanese Orthopaedic Association (JOA) scores clinically and timing of fusion, graft height and C2–7 angle measured on lateral radiographs. Any complication such as neurological deterioration, non-union, graft collapse or loss of angle was recorded. Delayed union was considered as radiological union identified only beyond postoperative 6 months. Risk factors including age, smoking, drinking, comorbidities and operative levels were analysed through a multivariate regression for their respective influences on the various outcomes.
Results:
Of the 69 patients studied, none of the patients had non-union, while 33 (47.1%) achieved fusion in 6 months. The most common complications were anterior protrusion of graft (5.8%) and hoarseness (2.9%). The 1-year mean change in JOA score was 3.9 ± 2.7. The C2–7 angle gradually became more kyphotic, despite an initial lordosis correction intraoperatively. The graft height also gradually collapsed during subsequent follow-ups. Multivariate regression model suggested that diabetics (cumulative odds ratio 7.4) and drinkers (cumulative odds ratio 8.6) were associated with delayed union.
Conclusion:
ACDF using tricortical iliac crest autograft has satisfactory outcomes with low occurrence of complications. Diabetics and drinkers were predictors of delayed union.
Introduction
Anterior cervical discectomy and fusion (ACDF) is a well-established anterior surgical strategy for management of cervical myelopathy since its introduction. 1 Successful ACDF surgery requires satisfactory neurological recovery and radiological outcomes without complications. For cervical myelopathy, the Japanese Orthopaedic Association (JOA) score is commonly used and a two-point score improvement is reported as the minimum clinically important difference (MCID). 2,3 Radiological evidence of fusion and maintenance of sagittal alignment are also important outcomes of surgery. 4 ACDF is commonly adopted for single- or double-level diseases 5 but less so for multilevel fusions due to significantly lower fusion rates. 6,7 Complications in ACDF surgery are not uncommon and may have severe sequelae. More commonly observed complications include graft collapse and subsidence, dysphagia and respiratory difficulties, hoarseness and pseudoarthrosis. 8
Several methods for ACDF have been reported including isolated tricortical iliac crest autograft, allograft, with or without plating and polyetheretherketone (PEEK) cages. 6,9,10 Decisions may be based on familiarity, perceived better fusion rates, immediate stability with early mobilization and earlier return to activities of daily living. 9,11 –14 Plating, in particular, may reduce graft-related complications and lead to improved fusion rates and less postoperative kyphosis. 4 Although stand-alone tricortical iliac crest autograft is one of the earliest ACDF techniques, there is limited information regarding its treatment outcomes. One study suggested that tricortical iliac crest autograft resulted in higher fusion rates and lower complication rates as compared to allograft or PEEK cages for single or multilevel ACDF, 11 while another suggested that autograft and PEEK cages provide comparable JOA scores, alignment and maintenance in intervertebral height. 15 It is important to note that these studies included plating procedures. A study comparing the use of tricortical graft alone or with plating suggested that stand-alone grafts lead to higher risk of pseudoarthrosis, graft collapse and kyphotic deformity postoperatively. 10 Nevertheless, the predictive risk factors for poor neurological and radiological outcomes in patients undergoing stand-alone tricortical iliac crest autograft have yet to be identified. Determining these risks is crucial for patient selection and optimizing surgical outcomes. Thus, this study aims to investigate the outcomes of stand-alone tricortical iliac crest autograft for ACDF surgery and to determine the factors influencing neurological outcomes, timing of fusion, graft collapse and resultant sagittal alignment.
Materials and methods
Study design
This was a retrospective study of all patients who underwent ACDF for cervical spondylotic myelopathy using stand-alone tricortical iliac crest autograft from October 2006 to September 2016. All patients with ACDF performed in the cervical spine (C2–7) with at least 2-year postoperative follow-up were included. Patients with insufficient follow-up duration of 2 years or missing data at specific time points (preoperatively; immediate postoperatively; and 6 months, 1 year and 2 years postoperatively) were excluded (Figure 1). A total of 31 patients with plating were excluded as our objective was to determine the outcomes of stand-alone tricortical iliac crest autograft for ACDF surgery. These patients underwent plating due to radiological instability which was defined as hypermobile spondylolisthesis with displacement of 3.5 mm or more and angulation of 11° or more on dynamic flexion–extension radiographs. Ethics approval was obtained from the local institutional review board.

Flow chart of patients included in the study.
Surgical technique
As all patients were managed under a single university unit, the surgical procedure was standardized. All patients underwent either one-level or two-level ACDF based on correlated clinical findings of cervical myelopathy and imaging findings of anterior compression due to disc herniation. All three-level or four-level compressions underwent laminoplasty. Moreover, we performed ACDF for any patient with a kyphotic sagittal alignment. During surgery, all patients were supine with arms by the side and a roll placed behind the scapulae to extend the neck and open up the space for incision. All patients adopted a right-sided Southwick–Robinson approach with the intended incision marked using the image intensifier. After marking the disc level, a complete discectomy including removal of the posterior longitudinal ligament (PLL) was performed. A spreader could be used at this stage for better visualization. After the disc material was removed, a cylindrical burr was used to remove any osteophytes and the usual cranial overhang. This was performed to create two parallel vertebral edges for insertion of the tricortical graft. The cartilaginous endplates were cleared, and the PLL was visualized and excised to expose the dura. Any remaining posterior osteophytes were removed. Removal of the posterolateral aspect of the uncovertebral joints was done if foraminal decompression was required. An assistant performed manual traction of the head underneath the drapes and the maximum disc space gap under traction was measured. A same-sized rectangular tricortical iliac crest autograft was harvested at the ipsilateral iliac crest, which was then fit into the disc space, slightly inset from the anterior border of the vertebral bodies. Finally, the graft was checked for its stability and its position with X-ray. No postoperative steroids were given. Patients were encouraged to sit out of bed, mobilize and walk on postoperative day 1. Patients were provided a rigid cervical collar for 8 weeks postoperative use before allowed free mobilization of the cervical spine.
Study parameters
Clinical information including gender, age at surgery, smoking habits and drinking habits were collected at presentation. Smokers were defined as someone who smoked any tobacco product at least one pack a day. Drinkers were defined as someone who drank at least one standard drink 16 a day. Comorbidities including hypertension, type 2 diabetes mellitus, hyperlipidaemia, ischaemic heart disease, cerebrovascular accident, gout, depression and osteoarthritis were also recorded. Intraoperative details included the operation level, blood loss volume (ml) and operative time (min). The preoperative and 1-year postoperative JOA scores 17 and erect lateral cervical spine radiographs at preoperative; immediate postoperative; and postoperative 6 months, 1 year and 2 years were obtained. On imaging, the sagittal alignment was measured by C2–7 angle and the disc height (graft height postoperatively) of the operated level was also measured from the midpoint of the lower end plate of the cranial vertebrae to the midpoint of the upper end plate of the caudal vertebrae. Once trabeculation have crossed the graft, the height could not be accurately measured since it had assimilated into the adjacent vertebral body. All measurements were performed by an investigator who was blinded to the clinical information during data collection.
Outcome parameters
The outcome measures included the changes in JOA, timing of fusion, C2–7 sagittal alignment changes and complications (neurological deterioration, non-union, graft collapse and protrusion, hoarseness, difficulty in breathing and dysphagia). The change in JOA score was calculated by preoperative JOA − 1-year postoperative JOA. Fusion was considered successful when the radiolucent gap between the graft and the end plate was absent, indicating there was bridging of trabecular bone 18 (Figure 2). Presence of radiolucent gap and mobility on flexion–extension radiographs indicated that fusion was incomplete (Figure 3). Delayed union was considered if no fusion was observed at the 6-month postoperative images. The change in C2–7 angle and disc/graft height was calculated for the immediate correction (immediate postoperative − preoperative) and postoperative correction (subsequent follow-up measurements − immediate postoperative measurement).

Illustrative case showing (a) a patient who underwent an ACDF at C4/5 with (b) satisfactory fusion at 6-month follow-up radiograph. The condition was (c) stable even at 2-year follow-up. ACDF: anterior cervical discectomy and fusion.

Illustrative case showing (a) a patient who underwent ACDF at C5/6 with (b) delayed union identified at the 1-year follow-up radiograph. Complete fusion was confirmed (c) at the 2-year follow-up radiograph. ACDF: anterior cervical discectomy and fusion.
Statistical analysis
Patient demographics and continuous data were presented as mean ± standard deviation, and categorical data were presented as percentage. Poor surgical outcomes were defined as worsened JOA score, delayed union, loss of C2–C7 alignment and graft collapse. Bivariate analysis included Pearson correlation or Spearman’s rank-order correlation tests for investigating any relationship between patient demographic factors, presentation of comorbidities with unfavourable changes of graft height, C2–C7 angle or JOA score as well as for the relationship between changes of graft height and C2–C7 angle at specific time points. Time for fusion at three postoperative follow-up time points and its potential risk factors were tested for association. Measures of association based on the χ 2 test of significance, Cramer’s V, were found to indicate the strength of the relationship. A Cramer’s V value of greater than 0.25 is considered a very strong relationship. 19 To avoid exclusion of any clinically important variable, any associated factor at p < 0.15 was purposefully selected for the multivariate analysis. 20 For unfavourable delayed union postoperatively, ordinal logistic regression was used to explore the association between significant predictors and the ordinal level of outcome of fusion occurring at postoperative time point 1 (at 0.5 years), time point 2 (between 0.5 year and 1 year) and time point 3 (between 1 year and 2 years). The test of multicollinearity for the identified risk factors and the test for proportional odds were performed to assess the validity of the one-equation model created and must be found satisfactory in order to proceed. Logistic regression allowed the parameter estimates to be generated and significant predictors to be identified in terms of how they were predictive of the defined outcomes. There was the calculation of the predictors’ cumulative odds ratios, which itself did not depend upon the response category (time for fusion).
Statistical analyses were performed using SPSS version 24.0 (IBM SPSS Inc., Armonk, New York, USA). The values of p < 0.05 were regarded as statistically significant.
Results
Baseline data
Of the 69 patients studied, 23 (33.3%) were females and 46 (66.7%) were males. Mean age of patients was 59.0 ± 12.0 years. Mean duration of surgery was 158.0 ± 39.6 min, and mean blood loss was 133.5 ± 76.2 ml. Up to 66.7% of patients had significant comorbidities (Table 1) including hypertension (36.2%) and type 2 diabetes mellitus (23.2%) being the most common. Fifty-nine (85.5%) patients underwent ACDF surgery on a single disc level, while 10 (14.5%) patients underwent two-level surgery. The most common operated level was C4/5 (33.3%), followed by C5/6 (24.6%).
Comorbidities, operated levels and intraoperative surgical parameters of study cohort.

%: percentage of the study population.
Clinical outcomes
The mean preoperative JOA was 10.4 ± 2.9, and the mean postoperative 1-year JOA was 14.1 ± 2.0. The average change in JOA score was an improvement of 3.9 ± 2.7. Only one patient had JOA deterioration after surgery (1.4%). Ten patients in the study (14.5%) had complications after surgery. The most common complication was anterior protrusion of graft (n = 4, 5.8%), followed by hoarseness (n = 2, 2.9%), tetraparesis (n = 1, 1.4%), difficulty in breathing (n = 1, 1.4%) and difficulty in swallowing (n = 1, 1.4%). There was one patient (n = 1, 1.4%) with persistent donor site iliac crest pain beyond 1-year follow-up. Regarding time for fusion, 33 (47.8%) occurred within postoperative 6 months, 28 (40.6%) occurred between postoperative 6 months and 12 months and 8 (9.6%) occurred between postoperative 1 year and 2 years. There were no iliac crest complications during follow-up.
Radiographic parameters
In all, 33 (47.8%) patients achieved fusion at 6 months, 28 (40.6%) achieved fusion at 1 year and 7 (10.1%) achieved fusion only at 2 years. One patient (1.4%) only achieved fusion at 3 years postoperatively. Hence, this contributed to a non-union rate of 0% and delayed union rate of 52.2%. The mean sagittal C2–C7 angle was 0.7° ± 6.0° (−12.0 to 11.4) immediate postoperatively, −0.2° ± 6.6° (−17.7 to 12.9) at postoperative 6 months, −0.5° ± 6.9° (−15.0 to 12.5) at postoperative 1 year and −0.3° ± 6.4° (−13.7 to 6.7) at postoperative 2 years. The change in C2–C7 angle was thus 1.4° ± 5.2° (p = 0.030) with surgery, −0.9° ± 2.7° (p = 0.009) at 6-month follow-up, −1.7° ± 3.8° (p = 0.001) at 1-year follow-up and −2.2° ± 3.8° (p < 0.001) at 2-years follow-up. The mean immediate postoperative graft height was 9.6 ± 1.7 mm (4.1–13.6), postoperative 6 months was 6.6 ± 1.8 mm (3.1–9.5), postoperative 1 year was 6.0 ± 2.0 mm (3.1–8.3) and postoperative 2 years was 3.0 mm (n = 1). The change in graft height was thus 3.6 ± 2.0 (p < 0.001) with surgery, −2.9 ± 1.7 (p < 0.001) at 6-month follow-up, −3.1 ± 2.3 (p = 0.006) at 1-year follow-up and −5.9 mm (n = 1) at 2-year follow-up. On average, patients developed graft collapse and further overall kyphosis deformity with each subsequent postoperative follow-up interval.
Correlation between risk factors and outcomes
Studied risk factors did not correlate significantly with other outcomes, including complication rate, immediate correction of C2–C7 angle and graft height and postoperative correction of C2–C7 angle and graft height at postoperative 6 months, 1 year and 2 years (all p > 0.1; Table 2). The exception was the correlation between change in JOA scores and smoking (r = 0.266, p = 0.027).
Test of correlation of patient demographics, comorbidities and continuous outcomes: Changes of JOA, graft height and alignment.a

JOA: Japanese Orthopaedic Association score.
a The number of graft collapse patients at postoperative 2 years is 1.
b Statistical significance at p < 0.05.
The change in C2–C7 angle did not correlate with graft height changes (Table 3). The graft height change between postoperative 6 months and immediate postoperatively (−0.374, p = 0.027) and between postoperative 1 year and postoperative 6 months (−0.729, p = 0.040) were significantly correlated with changes between immediate postoperatively and preoperatively. Up to 45.7% of graft collapse occurred in patients with an immediate postoperative graft height greater than the preoperative disc height. No correlation was observed between JOA changes postoperatively and C2–C7 alignment or graft height changes.
Bivariate analysis of graft collapse and alignment changes.a

a The number of graft collapse patients at postoperative 2 years is 1.
Predictors for outcomes
Associations (Table 4) were observed between timing of fusion and patients who were drinkers (Cramer’s V = 0.298), were diabetic (Cramer’s V = 0.246), underwent multilevel surgery (Cramer’s V = 0.247) and had two or more comorbidities (Cramer’s V = 0.240). These were important covariates to improve the final regression model with statistical significant effect: Wald χ 2 (df = 5) = 12.998, p = 0.023, −2 log likelihood: 120.665. The test for proportional odds was found satisfactory. The Wald test statistics in Table 5 suggest that diabetes mellitus (p = 0.039) and drinking (p = 0.038) are the significant factors, with multilevel/single-level surgery being marginally below the level of significance (p = 0.074). The cumulative odds ratio for drinkers having increasing time for fusion was 8.6 times compared to nondrinkers, whereas diabetic patients were 7.4 times more likely to have delayed fusion beyond postoperative 0.5 years as compared to those without diabetes.
Test of association of patients’ demographics, comorbidities and time of fusion.

a Statistical significance at p < 0.05.
b Statistical significance at p < 0.15.
Outcome prediction of time for fusion using ordinal logistic regression.
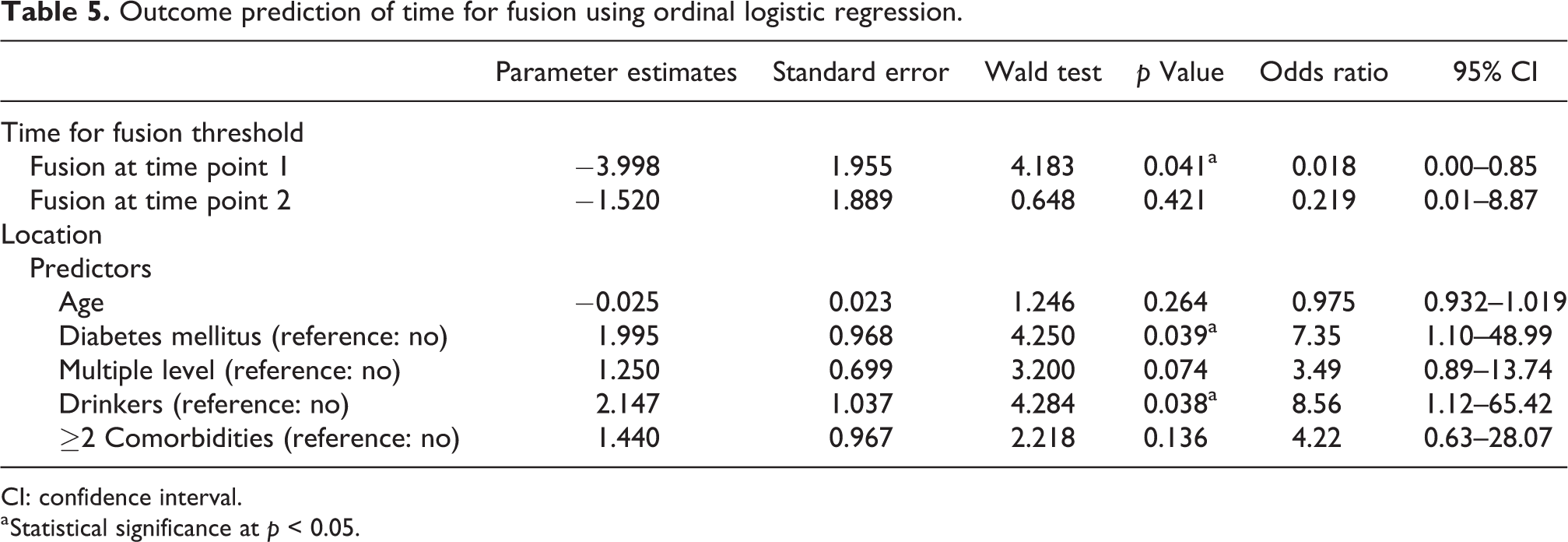
CI: confidence interval.
a Statistical significance at p < 0.05.
Discussion
ACDF surgery is a commonly adopted surgical procedure to manage cervical myelopathy. Despite its long history, tricortical iliac crest autograft is only studied in limited context. 10,15,21 In our centre, our standardized approach to performing ACDF is with stand-alone tricortical iliac crest autograft, and it is important to study the predictive factors for poor outcomes in this study population to improve our patient selection and preventive measures prior to cervical surgery. It was found that none of the patients who underwent this surgical procedure developed non-union although a fair percentage had delayed union. Improvement in JOA was satisfactory and complication rates were low. Diabetics and drinkers were predictors of delayed union.
First and foremost, the most important outcome to consider is neurological recovery after surgery. The average JOA improvement was observed to be 3.9, suggesting satisfactory improvement beyond the MCID. 2,3 It is also important to note that the deterioration rate was only 1.4%, which is similar to what has been traditionally reported in the literature for discectomies without fusion (3.3%) 22 and for ACDF (0.4%). 23 Interestingly, despite graft collapse in the majority of patients and progressive kyphotic alignment, there was no correlation with neurological deterioration. Our method of decompression to the dura with removal of the PLL is likely the main reason. Complete decompression to dura safeguards against buckling of the posterior annulus or PLL recurrent compression of the spinal cord. It is difficult to gauge this relationship in the literature as most studies have not presented the surgical technique in such detail. Future comparative studies with PLL and/or posterior annulus retention should be performed to highlight the impact of decompression down to dura.
As no patient suffered from non-union or required revision surgery, our reported union rates are by far higher than reported. Sharma et al. 10 found a non-union rate of 4.3% and 24% for one- and two-level stand-alone tricortical autografts for ACDF, respectively. Other studies showed similar poor results with stand-alone tricortical iliac autograft (fusion rate of 83%) 24 or even with plating (fusion rate of 90%). 12 These rates are likely overestimations, as their follow-up assessments were only performed up to 1-year postoperative follow-up. If we only consider the 1-year mark to indicate non-union, nine (13%) of our patients would have non-union. We have shown that 1-year follow-up is too short as 98.6% of our patients achieved radiological evidence of fusion at 2-year follow-up. Despite our reported inferior fusion rate of 87% at 1 year compared with plating, the patients were able to maintain the alignment, achieve satisfactory neurological improvement and avoid any need for revision surgery. It is important to note, however, that we advocate postoperative collar immobilization to maintain graft stability, while plating may allow for earlier mobilization. 25
The majority of patients experienced delayed union (52.2%) based on our strict definition of 6-month findings of cross-trabeculation on radiographs. Our analysis found that drinking and diabetes mellitus are significant predictors for delayed union and multilevel surgery is a possible predictor. Alcohol consumption has been noted to interfere with the innate ability of the body to heal wounds, increasing the time needed for cells and tissues to undergo effective proliferation and remodelling. 26 Type 2 diabetes mellitus has also been shown to lead to poorer quality of bony fusion due to adverse bone metabolism. 27 Poorer outcomes have been reported for multilevel surgery as the pathological processes are more severe and may require longer time for fusion to occur. 28 These risk factors should be considered in future planning for ACDF surgery whereby adjunctive measures such as plating may be warranted to improve fusion outcomes.
Our complication rate was low, and there was no correlation with neurological outcomes. As compared to a previous report, our rates of dysphagia (1.4% vs. 9.5%), clinically significant haematoma causing respiratory difficulties (1.4% vs. 5.6%) and hoarseness (2.9% vs. 3.1%) are much less prevalent. 29 The most common complication was anterior protrusion of the graft, which may be a by-product of graft collapse or resorption. Fortunately this did not have any effect on the fusion rates and all remodelled during follow-up. Although more commonly observed than with a plate whereby the graft is blocked from protrusion, these complications are less of a concern considering the avoidance of severe sequalae like oesophageal perforation with prominent plating. 30 Graft collapse was noted in many patients and could be related to the overdistraction achieved intraoperatively since 45.7% of patients with graft collapse had an immediate postoperative graft height greater than the preoperative disc height. Graft collapse may also indicate subsidence and as such, another risk may be violation of the endplates during preparation of the recipient site. The use of a high-speed burr to prepare the endplates is commonly adopted, and this may violate the stability and integrity of the endplates to receive the grafts. 31 Despite this, graft collapse appears to have no effects on the neurological outcome. Hence, the clinical implications of this phenomenon are uncertain. It is also important to note that our donor site pain was low with only one reported case beyond the 1-year follow-up. The likely rationale for this is preservation of the periosteum of the iliac crest during dissection and after obtaining the tricortical graft to repair the periosteum over the defect.
There is a trend of postoperative kyphosis which is independent of age or preoperative alignment. The kyphotic change is definitely a postoperative event rather than intraoperative correction as the mean immediate correction for C2–C7 angle was 1.3° in lordosis. The rectangular grafts were inserted under maximal manual longitudinal traction and hence may have contributed to the minimal changes in cervical lordosis. Despite a trend of increasing graft collapse consistent with kyphotic changes, no significant correlation between these events was observed. The lack of relationship has been similarly identified in a previous study. 10 The location of the graft collapse may be a reason for such phenomenon. Kyphosis occurs only with anterior graft collapse, while a posterior graft collapse may lead to lordosis. In tricortical grafting, the thick cortical portion of the iliac apophysis is usually placed just inset from the anterior column which also exists the stronger cortical bone of the vertebral body. Hence, the lack of positive relationship is not unexpected. A more likely cause for the kyphotic changes may be due to the biomechanical effects of the ACDF surgery itself, altering the inherent spine stability and increasing load and stress at the fused and adjacent segments. 32
There are some inherent limitations to this retrospective study. Due to the study design, some patients were excluded due to absent data which may have reduced our sample size. Validation should be performed in larger prospective studies. Our dates for assessing fusion were crude, as radiographs were only assessed at 6 months with some patients having earlier or later fusion not identified. Furthermore, our method of fusion assessment using radiographs may not be as accurate as computed tomography. 33 Nevertheless, our report should not be an overestimation of the fusion rates as we already used a strict definition of delayed union.
Conclusion
ACDF surgery with stand-alone tricortical iliac crest autograft has good fusion rates and satisfactory neurological recovery. Complications do occur occasionally, but they are vastly transient and self-limiting. Although fusion rates may be higher with plating within 1 year of surgery, stand-alone grafts can produce good results while reducing the cost of implants. Thus, this is still a viable option for surgeons to consider. Drinkers and diabetics are prone to delayed union with multilevel surgery as a potential predictor. These are risk factors that should be identified during preoperative assessment and are key considerations when selecting patients for ACDF with stand-alone tricortical iliac crest autograft.
Footnotes
Author contributions
Kenneth Kam Leung Yeung and Jason Pui Yin Cheung contributed equally to this article.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the AOSpine East Asia Research Grant: A quantitative study of gait and stance characteristics for patients with cervical spondylotic myelopathy.