
Abstract
Objective:
The purpose of our study was to determine whether there is a correlation between the lower limb rotational profile and tibial tuberosity-trochlea groove (TT-TG) distance.
Design and patients:
The computed tomography cross-sectional imaging on 50 patients’ lower limbs (100 limbs) was investigated at our institution. The TT-TG distance was measured along with rotational measurements including femoral version (FV), tibial torsion and knee joint rotation angle (KJRA). Patients were divided into two groups. Group 1 had a TT-TG ≥ 20 mm which was considered pathological and group 2 with a non-pathological TT-TG (≤19 mm). Rotational angles were compared between groups. Statistical analysis was performed using the t-test and Mann–Whitney U analysis.
Results and conclusions:
Our results demonstrated a statistically significant difference in the mean KJRA (p = 0.026) between the pathological (mean = 10.6, standard deviation (SD) = 7.79°) and the non-pathological TT-TG groups (mean = 6.99, SD = 5.06°). A higher mean value for FV and tibial torsion was also demonstrated in patients with a pathological TT-TG (18.2 vs. 13.7, 32.8 vs. 30.9, p > 0.05, respectively). In conclusion, there was a statistically significant higher mean value for the KJRA in patients with a pathological TT-TG. Hence, a lateralized tibial tubercle as demonstrated by an increase in the TT-TG distance may be associated with a coexisting lower limb rotational malalignment.
Introduction
Anterior knee pain and patella instability is a common orthopaedic problem. It is estimated that the overall incidence of primary patella dislocation in the population is approximately 5.8 per 100,000, with a fivefold increase in incidence between the ages of 10–17 years. Patellofemoral joint (PFJ) dysfunction is multifactorial, 1 which includes the soft tissue constraints around the knee, the osseous architecture and the overall rotational limb alignment (femoral version (FV), tibial torsion and knee joint rotation angle (KJRA). All of these principles contribute to the normal workings of the joint. 2
A lateralized tibial tubercle is a recognized cause for lateral subluxation of the patella. 3 Clinically, this lateral offset may be evaluated through measuring the Q angle (angle between the vector of action of the quadriceps and the patellar tendon). Alternatively, the tibial tuberosity-trochlear groove (TT-TG) distance allows quantitative assessment of the lateral offset of the tibial tubercle using radiological evaluation. Goutallier et al. first described the measurement in 1978 4 as the line between the ‘summit of the tibial tuberosity and the bottom of the trochlear groove’ measured on radiographs taken with the knee in 30° flexion. More recently in 1994, Dejour et al. published their findings on the use of computed tomography (CT) to evaluate patients with symptomatic PFJ instability. They concluded that a TT-TG distance equal to or greater than 20 mm was pathological, warranting surgical intervention in a symptomatic patient. 1 This technique of measuring the TT-TG distance is currently considered the gold standard (Figure 1).

Illustration of the calculation of the TT-TG distance. This is measured as the distance between a line bisecting the tibial tuberosity and a line bisecting the sulcus of the trochlear groove. TT-TG: tibial tuberosity-trochlear groove.
With relation to lower limb rotational alignment, deformities of increased femoral neck anteversion, torsional deformities of the femoral shaft and external tibial torsion increase the risk of PFJ dysfunction. Although there have been a number of studies that have been published on the methodology of measuring lower limb alignment, 5 –10 few studies quote a normal range for the various rotational parameters in a control population. Those that do, appear to have a wide variance and standard deviation in the values calculated, likely due to limited sample size. 11,12 The potential correlation between a pathological TT-TG and lower limb rotational malalignment in patients with anterior knee pain and patellar instability remains poorly established in the literature.
Our study aims to assess for a correlation between the TT-TG distance and lower limb rotational alignment. Our hypothesis was that rotational abnormalities of the lower limb have no correlation with TT-TG distance.
Methodology
Following review by the local ethics committee, ethical approval was obtained in accordance with the ethical standards laid down in the 1964 Declaration of Helsinki.
Sample
We retrospectively evaluated all axial CT scan images of patients who had presented to our outpatient clinic between 2009 and 2011. Patients with incomplete scans that failed to capture the hip, knee and ankle were excluded. Similarly, patients with prior history of a lower limb fracture, surgical realignment of the patella or underlying arthroplasty were also excluded from the study.
Image acquisition was obtained using 1 mm intervals using a multidetector CT scanner (Siemens four-channel MDCT, Siemens, Erlangen, Germany) using a standardized protocol. Each patient was placed supine with hip, knee and ankle joints in a neutral position. Each limb was simultaneously scanned at the level of the femoral neck, distal femoral condyle, proximal tibia and ankle joint.
Measurement
Picture archiving and communication technology software was used to analyse cross-sectional CT images of the hip, knee and ankle joints by two observers independently. Both observers are co-authors in this study have experience in analysing CT imaging for lower limb rotational profile assessment. Both were blinded with relation to the TT-TG distance, which was also measured by a fellowship trained musculoskeletal radiologist.
The axis for which measurements were taken included: the femoral neck axis (a), dorsal condylar line of the distal femur (b), dorsal condylar line of the proximal tibia (c) and the transmalleolar axis (d) (Figures 2 –5).
Femoral neck axis, as described by Hernandez et al., as the axis created by a line passing through the centre of the femoral head and midpoint of the femoral neck in a cross-sectional CT cut where the femoral head, isthmus of the femoral neck and superior border of the greater trochanter are evident. CT: computed tomography.

Dorsal condylar line of distal femur referenced as the axis line drawn along the most posterior aspect of the dorsal femoral condyle. Here, this is measured as 20.4° internal rotation on the right.

Dorsal condylar line of proximal tibia referenced as the axis line distal to the articular surface of the tibial plateau and proximal to the fibula head, measured at 10.6° internal rotation on right.

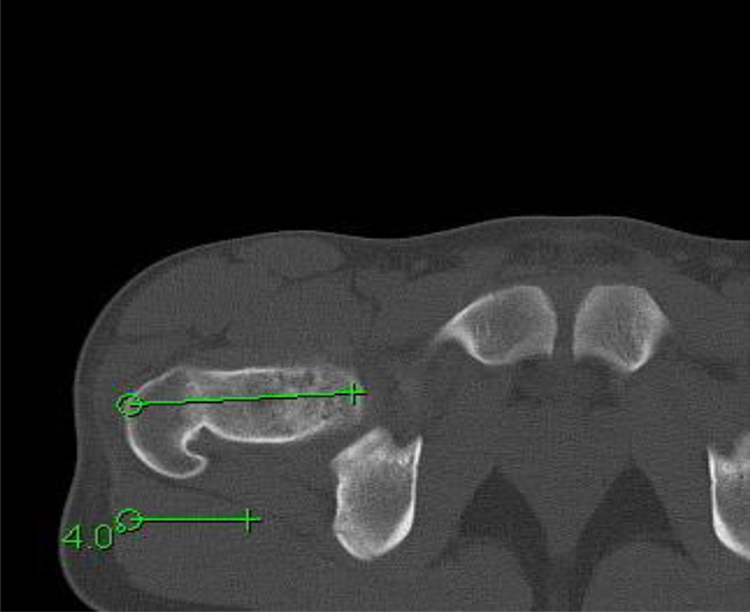
Transmalleolar axis referenced as the axis created by a line drawn from the centre of the medial and lateral malleoli, in this case 33.3° external rotation on right.
The femoral neck axis was measured as described by Hernandez et al., as the axis created by a line passing through the centre of the femoral head and midpoint of the femoral neck in a cross-sectional CT cut where the femoral head, isthmus of the femoral neck and superior border of the greater trochanter are evident. 10 The transmalleolar axis 7 was measured as the axis created by a line connecting the centres of medial and lateral malleoli. Both these measurements have been advocated as being reliable methods of measurement by Liodakis et al. as they are associated with lower inter- and intra-observer variability. 9 The dorsal condylar line of the proximal tibia was taken as the axis line just distal to the articular surface of the tibial plateau and proximal to the fibular head. 7 Finally, the distal femur reference was taken as the dorsal condylar line as described by Jend. 5
Internal rotation or retroversion was represented as a negative (−) value and external rotation/anteversion was represented as a positive (+).
Using these measurements, values for femoral torsion, tibial torsion and KJRA were calculated as follows: Femoral torsion (FV): angle between the dorsal condylar line of the distal femur and the femoral neck axis; KJRA: angle between dorsal condylar line of the proximal tibia and dorsal condylar line of the distal femur; Tibial torsion: angle between the transmalleolar axis and the dorsal condylar line of the proximal tibia.
In addition, the TT-TG distance for each limb was assessed as the distance between the most anterior aspect of the tibial tuberosity and the deepest bony point of the trochlear groove as described by Dejour et al. 1
Statistical analysis
The intraclass correlation coefficient (ICC) and their 95% confidence intervals (CIs) were used to summarize the inter-observer reliability in a single measurement. The ability of a test to show intra- and inter-observer reliability was evaluated using the two-way random effects model assuming a single measurement and absolute agreement using the R Program (R version 2.14.1, Copyright (C) 2011 The R Foundation for Statistical Computing ISBN 3-900051-07-0). An ICC of 1 means perfect reliability and an ICC of 0 means the opposite. Mini tab 16 software was used to perform statistical analysis on the data.
Statistical analysis in the form of the t-test was used to assess for any statistical significant difference in the means of the FV and tibial torsion between the pathological and non-pathological TT-TG groups. Due to the non-parametric distribution of the KJRA measurements, a Mann–Whitney U analysis was performed to evaluate for a similar trend in this data set. Furthermore, logistic regression analysis on the continuous data set was performed to assess for a correlation between the TT-TG and the various rotational parameters measured.
In addition, a post hoc power analysis using nQuery Advisor software was also performed.
Results
A total of 100 lower limb scans (50 patients) were included in our study. The average age of the patients was 32 years (range 15–55 years). There were 36 female and 14 male patients. The data set was then separated into two study groups: Group 1 (n = 21) representing patients with a pathological or abnormal TT-TG distance (≥20 mm) and group 2 (n = 79) with a non-pathological or normal TT-TG distance (<20). There was no significant difference in the mean age between the pathological and non-pathological groups (31 years vs. 32 years, respectively). A statistically significant difference was noted in the mean TT-TG distance between the two groups (24 vs. 15, p < 0.05).
Data for the various rotational parameters were analysed for normality. Kolmogorov–Smirnov Z test showed significantly non-normality (p ≤ 0.010) of the KJRA data set. Contrary to this, the data set for FV and tibial torsion demonstrated a normal distribution. In addition to this, a paired t-test was applied to evaluate for a relationship between the left and right knee joints of each patient for FV and tibial torsion. Similarly, a Wilcoxon matched pairs rank test was used to evaluate this relationship for the KJRA (due to non-normal distribution). The results demonstrated a lack of independence in the variables between left and right knees and this was subsequently accounted for in further statistical analysis.
As a result, a Mann–Whitney U test demonstrated a statistically significant difference in the KJRA between the pathological and non-pathological TT-TG groups (mean 10.6 vs. 7.0, p = 0.026). Furthermore, a higher mean FV and tibial torsion were observed in the non-pathological TT-TG group as compared with the pathological group. However, this difference was not appreciated as statistically significant (Table 1).
Comparison of the mean values of the rotational parameters between the pathological and non-pathological TT-TG groups.

TT-TG: tibial tuberosity-trochlear groove distance; KJRA: knee joint rotational angle; FV: femoral version; SD: standard deviation; group 1: pathological TT-TG; group 2: non-pathological group.
a p = 0.026.
Using the results published by Seitlinger et al., mean ranges for a normal range of FV, tibial torsion and KJRA were established as 3–17°, 19–33° and 0–6°. Based upon these normal ranges, further subgroup analysis of our data set demonstrated that 71% of patients with a TT-TG ≥ 20 had an abnormal FV and KJRA and 33% of individuals in this group had an associated abnormal tibial torsion. In the non-pathological TT-TG group, 52% of individuals had an abnormal FV, 42% an abnormal tibial torsion and 60% an abnormal KJRA.
We went on to perform a post hoc power analysis which demonstrates that assuming α = 0.05, our study was sufficiently powered with a 1−β of 82% for the KJRA data, however, insufficiently powered for FV and tibial torsion.
The intra-class correlation coefficient for both intra- and inter-observer variability showed an overall excellent level of agreement for all measurements taken (please see Table 2 (ICC > 0.94)).
Inter-observer reliability measurements.
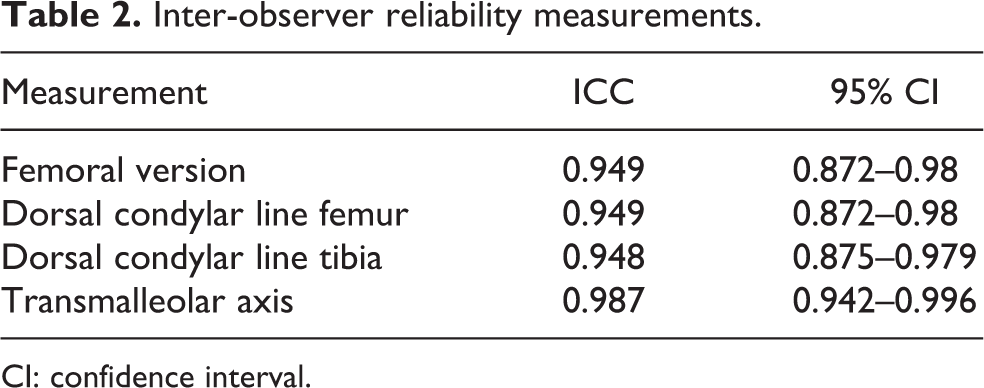
CI: confidence interval.
Discussion
Our results demonstrate a statistically significant higher mean value for the KJRA in patients with a pathological TT-TG distance as compared with patients with a non-pathological distance. These findings are supported by Seitlinger et al. 12 They primarily looked at the tibial tubercle-posterior cruciate ligament distance on magnetic resonance imaging with the aim of identifying a new measurement to determine true lateralization of the tibial tubercle. As part of their methodology, the authors also evaluated lower limb rotational profile in their patient cohort. They concluded a similar trend of a higher KJRA in patients with TT-TG ≥ 20. In this study, they found that only 43% of individuals with a pathological TT-TG distance have a normal position of the tibial tubercle, suggesting that the pathology may arise more proximally. The results from our study suggest that KJRA plays a role in TT-TG distance, with external rotation at the knee joint increasing the TT-TG and relative internal rotation decreasing it.
There was a trend towards a higher mean value for FV and tibial torsion in the pathological TT-TG group versus the non-pathological group. However, these results were not demonstrated as statistically significant. This may be attributed to a small sample size and subsequently, the study was found to be underpowered for these variables. Cameron and Saha described the contribution of lower limb rotational malalignment to instability with good outcomes following de-rotation osteotomy 13 ; however, the relationship between rotational malalignment and TT-TG remains poorly documented in the literature.
We therefore propose that a raised TT-TG distance in the presence of symptoms of anterior knee pain and instability may be secondary to two different pathologies. As reported by Seitlinger et al., 12 57% is due to a truly lateralized tibial tubercle with the remainder potentially secondary to an increase in external rotation of the proximal tibia relative to the distal femur. TT-TG is thus an amalgamated measure between the two variables, raising the possibility that patients with a raised TT-TG may not have true pathological lateralization of the tibial tubercle but a combination of lateralization and external rotation at the knee joint. The effects of tibial tubercle medialization are unknown in patients with increased KJRA and it is possible that this may be one of the factors contributing to the variation in results seen in patients with a raised TT-TG who undergo corrective surgery.
On this basis, when investigating patients for patellofemoral disorders, we propose that assessment of the rotational profile should be part of a patient’s examination. It has been suggested in the literature that if a significant lower limb rotational abnormality coexists, then surgical correction to restore normal mechanical alignment may improve clinical outcomes. Paulos et al. in 2009 retrospectively compared the clinical outcomes of high tibial rotational osteotomy versus Elmslie–Trillat–Fulkerson proximal–distal realignment for patella instability in patients with tibial torsion (foot thigh angle > 30°). They concluded that a better clinical outcome with a return to a more normal gait was observed in patients who underwent simultaneous correction of lower limb torsional deformity as compared with those who had conventional proximal–distal alignment procedure. 14
A limitation of our study is the absence of a control group of normal individuals. As a result, it is not possible to confidently ascertain the incidence of lower limb malrotation in a normal population, nor has it been possible to identify normal cut-off values for the various elements of lower limb rotational alignment in our patient population. There is very limited published literature evaluating the lower limb rotational profile in the normal adult population. One such study by Yagi in 1994 looked at the lower limb rotational profile in patients with knee osteoarthritis. This study consisted of a control group of 12 patients (24 knees) with no lower limb symptoms. The mean KJRA reported was of 9.2°, FV was 15.6° and tibial torsion was 23.5°. 11 Seitlinger et al., more recently, however, reported a much lower mean KJRA of 2.6°, although their FV and tibial torsion were of a similar magnitude (10.1° and 26.3°) in the study control group. Their control population included a larger cohort of 60 patients. In addition, we also acknowledge that while our sample size was sufficiently powered for evaluation of KJRA, this was not the case with regards to FV and tibial torsion. On this basis, we cannot completely exclude a correlation between a pathological TT-TG distance and FV and tibial torsion. This therefore gives potential scope for expansion of this study in the future when a larger population sample size may be available.
Conclusion
In conclusion, our results demonstrate that there was a statistically significant higher mean value for the KJRA in patients with a pathological TT-TG distance as compared with patients with a non-pathological distance.
Thus, patients with lateralization of the tibial tubercle may have coexisting rotational abnormalities of the femur and tibia contributing to their symptoms. Further clinical investigation is required to investigate the effects of this rotational malalignment on the outcome of distal realignment surgery.
Footnotes
Acknowledgements
The authors of the study would like to thank Mr Roger Holder (Primary Care Clinical Sciences, University of Birmingham) and Mr Justin Harvey (Centre for Statistical Consultation, University of Stellenbosch) for their support with the statistical analysis of the study data.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.