
Abstract
Purpose:
Tibial bowing in valgus knees with arthritis can lead to component malplacement during total knee arthroplasty (TKA). Incidence of valgus knees with medial tibial bowing, its effect on tibial component placement during primary TKA and methods to improve accuracy of the component placement were studied.
Methods:
Full-length weight-bearing alignment radiograph was taken in 117 patients (149 knees) with valgus deformity undergoing TKA. In these cases, the proximal tibial reference for extramedullary jig placement was planned preoperatively with reference to the tibial spines and classified as four zones.
Results:
The mean preoperative hip–knee–ankle (HKA) angle was 192.9° (180.3–234.5°). Bowing >3° was considered significant (p < 0.001) and at this level of bowing, the proximal tibial reference was shifted from centre to medial. Tibial bowing <3° was considered straight and >3° as tibia valga. Tibia was bowed in 70 knees (46.97%). Severity of valgus deformity had strong positive correlation with the tibia valga (p < 0.001). The post-operative medial proximal tibial angle (MPTA) and HKA angle were 91.63° (87.9–95.7°) and 182.6° (178.1–189.7°), respectively. The mean MPTA and post-operative HKA angle in bowed and straight tibiae were 90.35° versus 89.78° (p = 0.547) and 181.5° versus 180.7° (p = 0.5716), respectively, and the difference was not statistically significant.
Conclusion:
Medial tibial bowing is very common in valgus knees. Tibia valga has a strong positive correlation with the severity of valgus deformity. Accurate tibial component placement can be achieved with a medialized reference point for extramedullary tibial cutting jig in knees with significant tibia valga. The study has been registered in clinical trials registry – India (CTRI/2018/03/012283).
Keywords
Introduction
Degree of lower limb malalignment influences the rate of structural progression of degenerative changes in an arthritic knee. 1 An important measure of lower limb alignment is the hip–knee–ankle (HKA) angle, which corresponds to the lower limb mechanical axis. In neutrally aligned limbs, the medial compartment bears 60–70% of the force across the knee during weight bearing. 2 Deviation from neutral mechanical axis can arise from intra-articular or extra-articular deformities of the femur, the tibia or both. Coronal bowing of femur and tibiae in varus knees has been well described in literature and it can lead to component malplacement. 3 Valgus knees tend to have medial tibial bowing and are frequently associated with distal metaphyseo-epiphyseal femoral deformities. 4
Primary valgus deviation of the tibial meta-diaphysis (not associated with any pathological cause or surgery) could be present in many total knee arthroplasty (TKA) patients performed for degenerative valgus knees. 1 The effect of this phenomenon on tibial component placement has not been well studied. Ideal alignment of tibial component is perpendicular to the mechanical axis of the tibia in the coronal plane with a range of ±3° of either varus or valgus alignment. Tibial medullary canals of Asian patients are often bowed and can result in unacceptable tibial cut. 5 If there is lateral tibial bowing as in the cases of varus knees, chance of the tibial component placement in varus is high. 5 In cases of valgus knees, medial tibial bowing is common and tibial component placement tends to be in valgus with respect to the mechanical axis. Also it can cause cortical impingement in cases where tibial stem is used (Figure 1). In such patients, preoperative planning should include assessing the severity of tibial bowing and the intended position of the tibial component and change in surgical technique to achieve a well-aligned TKA. The literature review shows only one study regarding tibial bowing in valgus knees; and no study analysing the tibial component placement in tibia valga. Hence the aim of this study is to assess the incidence and severity of tibial bowing in patients with valgus knees, its implications on the tibial component placement in TKA and to analyse the post-operative limb alignment in those knees in which tibial component placement has been adjusted according to the preoperative planning.

(a) Medial coronal bowing of tibia 4.9°, (b) post-operative HKA angle of 183°, (c) medial proximal tibial component placement angle of 93° with valgus position, (d) post total knee replacement with medial collateral ligament insufficiency with a bowing of 4.8°, and (e) revision total knee replacement with hinge knee, arrow showing medial overhang of tibial tray and tibial stem impinging the medial cortex due to tibia valga. HKA: hip–knee–ankle.
Materials and methods
This is a prospective study involving patients with valgus knees undergoing TKA from January 2014 to September 2016 in our hospital. Ethics committee approval was taken from the institutional review board (IRB No. 2013/12/04). Well informed written consent was taken from all the patients and the nature of the study was explained. Preoperative full-length standing alignment X-ray was taken for all the patients who underwent TKA in our hospital.
Inclusion criteria
All patients undergoing primary TKA of any age or gender with a hip-to-ankle preoperative radiographs with HKA angle >180° and those who signed the informed consent were included in the study. The radiographs were taken without any rotation with patella centred over the femoral condyles.
Exclusion criteria
Patients with preoperative and post-operative radiographs not fulfilling the standardization criteria, those with post-traumatic pathology causing tibial bowing, congenital or dysplastic bowing, previous femoral or tibial osteotomy or previous fracture of the tibia with or without internal fixation were excluded from the study. Also, patients requiring tibial stem extension or wedges for defect augmentation during surgery were excluded as this might bias the component placement.
Standardization of radiographs
All patients had full-length weight-bearing radiographs of both lower limbs in true anteroposterior (AP) position. Radiographs were studied using PACS software (CE-0124, Version 7.2 Revision 13677). The following radiological parameters were documented.
Preoperative HKA angle
This is the angle measured in a full-length alignment radiograph of the lower limb between the line joining the centre of femoral head to the centre of the femoral intercondylar notch with the line joining the centre of the talus to the centre of the tibial plateau (Figure 2(a)).

Measurement of (a) preoperative HKA angle, (b) coronal bowing of tibia, (c) post-operative HKA angle and MDFA, and (d) MPTA. HKA: hip–knee–ankle; MDFA: medial distal femoral component angle; MPTA: medial proximal tibial component angle.
Tibial bowing angle
The entire tibia shaft is divided into three equal parts. A vertical line describing the midpoint of the endosteal canal was drawn in the proximal and distal third. The angle formed between these two lines showed the tibial bowing angle (Figure 2(b)).
Post-operatively, standing alignment radiographs were obtained at 6 weeks follow-up. The following parameters were assessed.
Post-operative hip knee ankle angle
As measured in the preoperative setting, HKA angle was measured in full weight-bearing lower limb alignment radiographs. Ideal angle is 180 ± 3° (Figure 2(c)).
Medial proximal tibial component angle
Medial proximal tibial component angle (MPTA) was defined as the angle between the mechanical axis of the tibia and the tangent to the tibial component drawn at the component–cement interface of the base plate, measured on the medial side of the knee. It shows the accuracy of placement of tibial component (Figure 2(d)). Ideal angle should be 90° in AP view with respect to the mechanical axis of tibia and a range of 90 ± 2° is considered acceptable.
Medial distal femoral component angle
This is the angle formed between the mechanical axis of femur and the line drawn tangential to the femoral component. This represents the femoral component placement angle and ideal placement is 90 ± 3°.
Preoperatively, the placement of tibial extramedullary jig in the proximal tibia was decided using the distal tibial axis as reference. The distal tibial axis was drawn as a line from the centre of the talus, passing through the middle of the distal one-third of the medullary canal of tibia. This line was extended proximally to the point of exit in the tibial plateau. The reference points were marked as four zones: (1) lateral tibial spine (L), (2) central (C), (3) medial tibial spine (M), and (4) medial to medial tibial spine (MM) (Figure 3). The same reference was used intraoperatively for tibial jig placement.

The four zones on the tibial plateau for tibial jig placement: (a) lateral tibial spine, (b) central, (c) medial tibial spine, and (d) medial to medial tibial spine.
Surgery was performed using conventional jigs. Correctability of valgus deformity was assessed under anaesthesia. The residual valgus was considered as surgical valgus. Surgical valgus >15° was approached through lateral parapatellar arthrotomy. Mild valgus or correctable valgus was approached through a medial parapatellar arthrotomy. Tibial cut was made perpendicular to the tibial mechanical axis with the extramedullary jig with 3 degrees posterior slope. The reference point for jig positioning was based on the preoperative planning (Figure 3). After the tibial cut was made, extramedullary alignment rod was used to check the accuracy of the cut and the drop rod has to be aligned to the centre of the talus (Figure 4). The distal femoral cut was made at a valgus correction angle individualised for each patient measured from preoperative long film with the intramedullary jig. Mild to moderate valgus was corrected by inside-out technique – posterolateral capsulotomy, pie crusting of iliotibial band. Severe valgus was corrected by the release of posterolateral capsule, iliotibial band, followed by either lateral epicondylar osteotomy and using a posterior stabilized knee, or release of popliteus and lateral collateral ligament and the level of constraint was determined intraoperatively depending on the integrity and functionality of the medial collateral ligament. Contained tibial defects in the lateral tibial condyle were reconstructed with bone grafts. Figure 5 shows a typical cases of severe valgus knee with tibia valga managed with medialized tibial reference resulting in accurate component placement and limb alignment.
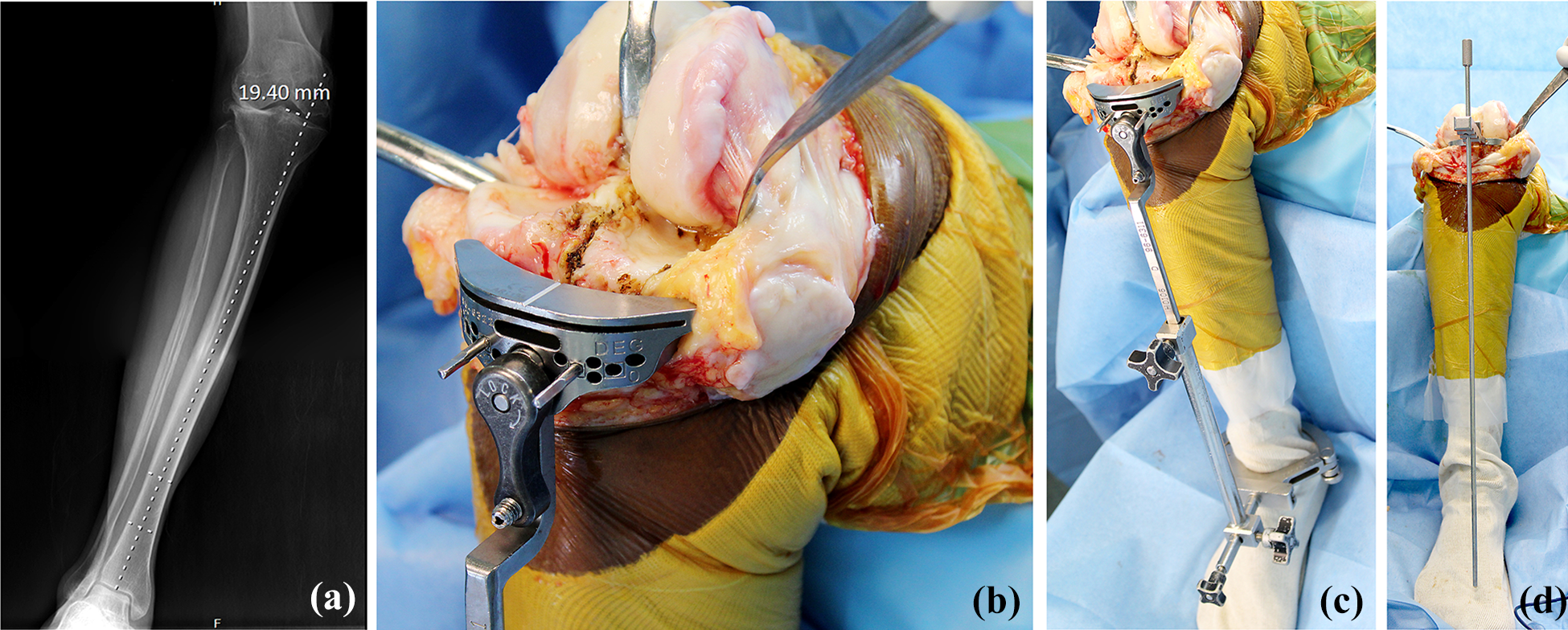
(a) Preoperative planning X-ray showing the reference point medial to medial tibial spine and its distance from the centre of the intercondylar eminence, (b) tibial jig placement centred on medial tibial spine, (c) extramedullary jig being used, and (d) accuracy of the tibial cut assessed with tibial trial and drop rod and tibial cut revised to achieve perpendicular cut with drop rod centred over the ankle.

Measurement of (a) preoperative HKA angle 209.7°, (b) coronal bowing of tibia 8.1°, (c) the tibial component appears to be in 2° varus, (d) medial proximal tibial placement angle 90° measured in long leg radiographs, and (e) post-operative HKA angle 181°. HKA: hip–knee–ankle.
Statistical analysis
Numerical variables were expressed as mean and standard deviation and categorical data were expressed as frequency and proportion. Karl Pearson correlation coefficient was used to assess correlation between the numerical variables. Independent two-sample t-test was used for comparing the numerical variables with sex and etiology. The p value for each of the anatomical variations was calculated and the p value <0.05 was considered statistically significant. Outliers of post-operative HKA angle (180 ± 3°) and MPTA (90 ± 2°) were noted.
There are no previous studies which look exactly into the tibial component placement in valgus knees with tibial bowing. Based on the previous studies on tibial bowing with 95% confidence level and 10% allowable error, the minimum sample size comes to 93. We took 149 samples in our study, which will give more than 95% confidence level and less than 10% allowable error.
Results
One hundred and seventeen patients (male: 31 (26.5%) and female: 86 (73.5%)) were enrolled and 149 knees were analysed. Major causes of arthritis in these patients were primary osteoarthritis (79) followed by rheumatoid (34), post-traumatic arthritis (3) and ochronotic arthritis (1). All the TKAs were done with posterior stabilized prosthesis. Two different prostheses were used (PFC, DePuy, Inc., Warsaw, Indiana, USA and Genesis II, Smith and Nephew, Memphis, USA). Six patients had lateral femoral augments, and seven patients had femoral stems. Thirty-three patients had lateral parapatellar arthrotomy and 116 had medial parapatellar arthrotomy. Lateral epicondylar osteotomy was done in four patients. Two patients had constrained implant (PFC TC3, Depuy, Inc., Indiana, USA).
Table 1 shows the statistics of variables in the study group. The mean preop HKA angle was 192.9° (180.3–234.5°). Bowing >3° was considered significant (p < 0.001) and at this level of bowing, the proximal tibial reference was shifted from centre to medial. Tibial bowing <3° was considered straight and >3° as tibia valga, as shown in Table 2. Correlation study of different variables with the severity of bowing revealed that the severity of bowing had a strong positive correlation with the severity of the valgus deformity expressed in HKA angle (p < 0.001). Tibia was bowed in 70 knees (46.97%) and straight in 79 knees (53.02%).
Statistics of study variables in the study group.
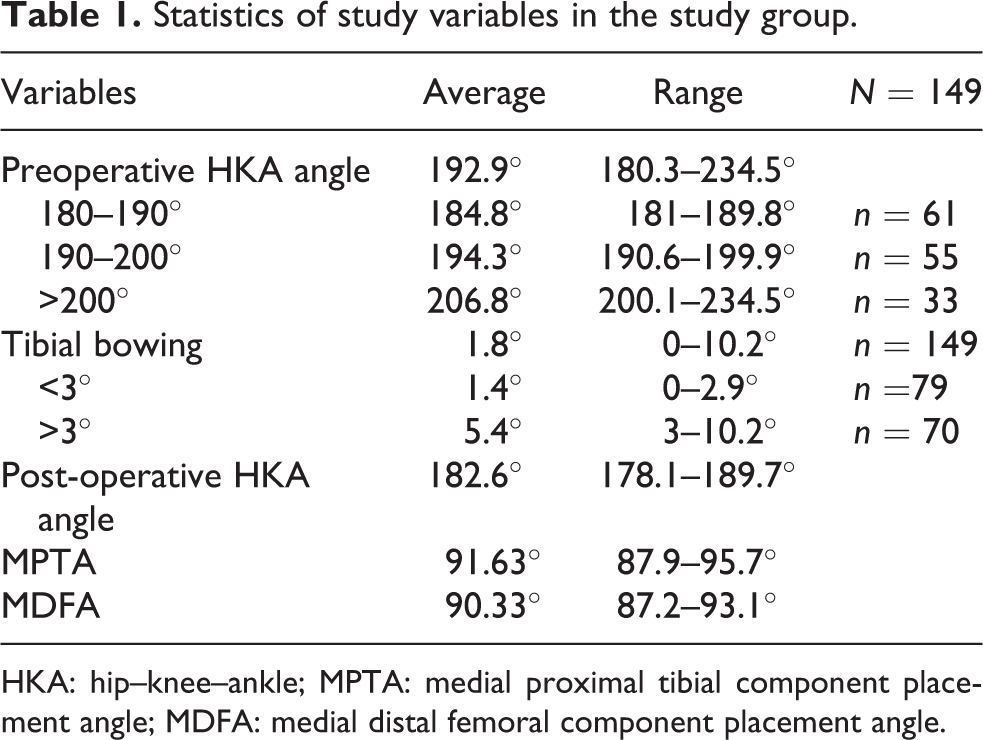
HKA: hip–knee–ankle; MPTA: medial proximal tibial component placement angle; MDFA: medial distal femoral component placement angle.
Correlation of bowing with the severity of valgus deformity.

HKA: hip–knee–ankle; R: right; L: left; M: male; F: female; OA: osteoarthritis; RA: rheumatoid arthritis.
No statistically significant correlation was seen between bowing and preoperative diagnosis (p = 0.228), age (p = 0.349), side (p = 0.656) or sex (p = 0.798). We observed that among the 149 knees, the tibial mechanical axis passed through lateral tibial spine in 19 (12.75%) knees, central zone in 48 (32.21%) knees, through medial tibial spine in 67 (44.97%) knees and medial to medial tibial spine in 15 (10.06%) knees (Figure 6).

The correlation between the degree of tibial bowing and the proximal tibia zones used is shown. L: along lateral tibial spine; C: central interspinous region; M: along medial tibial spine; MM: medial to medial tibial spine. Bowing >3° correlates with medial tibial spine as reference (p < 0.001).
All the cases in which the axis passed through or medial to medial tibial spine had tibial bowing more than 3°. The correlation between the zones and the severity of tibial bowing was statistically significant (p < 0.001).
The mean post-operative HKA angle was 182.6° (178.1–189.7°). The mean tibial component placement angle (post-operative MPTA) was 90.35° in bowed tibiae group (88.3–93.5°) and 89.78° (87.1–94.3°) in straight tibiae group, which was not statistically significant (p = 0.547). There were 16 outliers (MPTA > 90 ± 2°) in bowed group and 11 in straight tibiae group (Table 3).
Correlation between severity of bowing with post-op HKA angle, MPTA & MDFA.
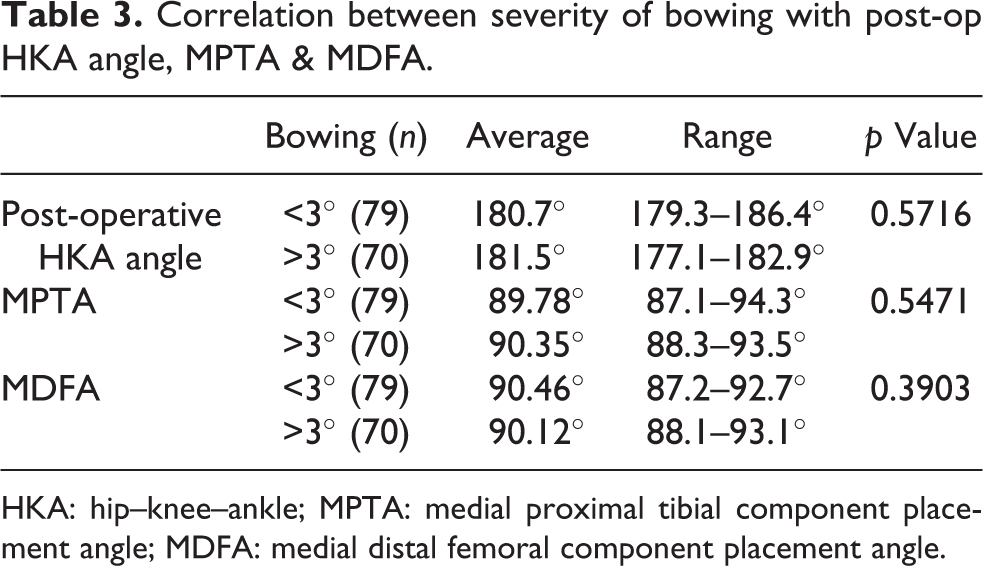
HKA: hip–knee–ankle; MPTA: medial proximal tibial component placement angle; MDFA: medial distal femoral component placement angle.
The analysis shows that MPTA, medial distal femoral component angle (MDFA) and post-operative HKA angle are not influenced by the severity of bowing. The average post-operative HKA angle in bowed tibiae and straight tibiae was 181.5° (177.1–182.9°) and 180.7° (179.3–186.4°) respectively, which was not statistically significant (p = 0.571). The average MDFA was 90.12° (88.1–93.1°) in the bowed tibia group and 90.46° (87.2–92.7°) in the straight tibia group (p = 0.390) and the difference was not statistically significant.
Discussion
The survivorship of TKA depends on the correct restoration of the mechanical axis of the leg and the accuracy of bone cuts. 6 The cuts of the femur and tibia should be made perpendicular to their respective mechanical axes in the coronal plane. Bone cut errors should be within 3° from the ideal position. 5 Accuracy of component positioning relies on appropriate use of cutting jigs and alignment guides for making precise and accurate bone cuts. Bargren et al. reported a 91% failure rate for TKAs with varus tibio-femoral alignment and 11% for valgus alignment. 7
Valgus malalignment in osteoarthritic knee is rarer when compared to varus deformity. The intra-articular sources of valgus malalignment are usually evident and are rectified intraoperatively. But, other possible extra-articular sources of valgus malalignment, such as tibial and femoral bowing, are usually concealed clinically and are easily overlooked during surgery. Primary tibia valga has been reported as a frequent anatomic pattern in patients with arthritis knee with valgus deformity. Studies done in different races of population have shown high incidence of tibial bowing with the incidence reaching up to 50%. 1 There have been studies which state that almost 50% of the extra-articular deformities at the knee were not recognized in routine short radiographs. 1 As the severity of valgus deformity correlates with that of tibial bowing, full-length radiographs are indicated in patients with preoperative severe valgus deformity. The incidence of tibial bowing in the coronal plane was high in our population and also with end-stage osteoarthritis of the knee.
On extensive literature search, we could not find a single study which looks into the incidence of tibial bowing and also its effect on tibial component placement in valgus knees. The only study that reports tibial bowing in valgus knee is a radiographic analysis of patients with valgus deformity in a wide range of population. 1 Femoral bowing in varus and valgus knees due to osteomalacia changes has been well described. These findings have implications in deciding the optimum valgus angle at which the distal femoral resection has to be done. 3,8 Ranawat has recommended distal femoral resection with 3° valgus to compensate for remodelling in severe valgus deformity. 4
In the normal knee, the articular surface of the proximal tibia angle is at an average of 3° varus to the mechanical axis. However, it is recommended that the position of the tibial component should be perpendicular to the mechanical axis of tibia to provide a uniform distribution of load across the implant–bone interface and to optimize the prosthesis survival. 1,7,9,10 Conflict exists in the choice of either extramedullary or intramedullary alignment system for the tibial cut. Reed et al. concluded that the use of intramedullary jigs is superior to extramedullary jigs. 11 Dennis et al. emphasized that extramedullary guides should be distally positioned over the centre of the talus, 3 mm medial to the midpoint of the ankle rather than right at the midpoint to avoid varus tibial resection. With this technique, 88% of tibial components were aligned within 90 ± 2°. 12 While most patients are suitable for the use of either alignment system, patients with a large soft tissue envelope can preclude the use of an extramedullary guide while tibial deformity, previous fracture or retained hardware can prevent the use of an intramedullary guide. Such patients may require the use of extramedullary guides and intraoperative radiographic control or navigation-based surgery. 13 Among the 149 knees included in our study, 46.97% had tibial bowing >3°. Our study showed using extramedullary jig with careful preoperative planning gives good component placement, as shown in case examples (Figures 7 and 8). Some patients had severe bowing in which the passage of intramedullary rod might be impossible. But the use of extramedullary cutting jig and confirming the cut using an alignment drop rod negates the effect of coronal tibial bowing in reconstructing the mechanical axis of the limb.

The preop and post-op angles in a bowed tibia are shown. (a) Preoperative HKA angle 193.3°, (b) tibial bowing of 8.1°, (c) reference point taken was medial tibial spine, (d) post-operative HKA angle 180° and MDFA 90°, and (e) MPTA 90°. HKA: hip–knee–ankle; MDFA: medial distal femoral component angle; MPTA: medial proximal tibial component angle.
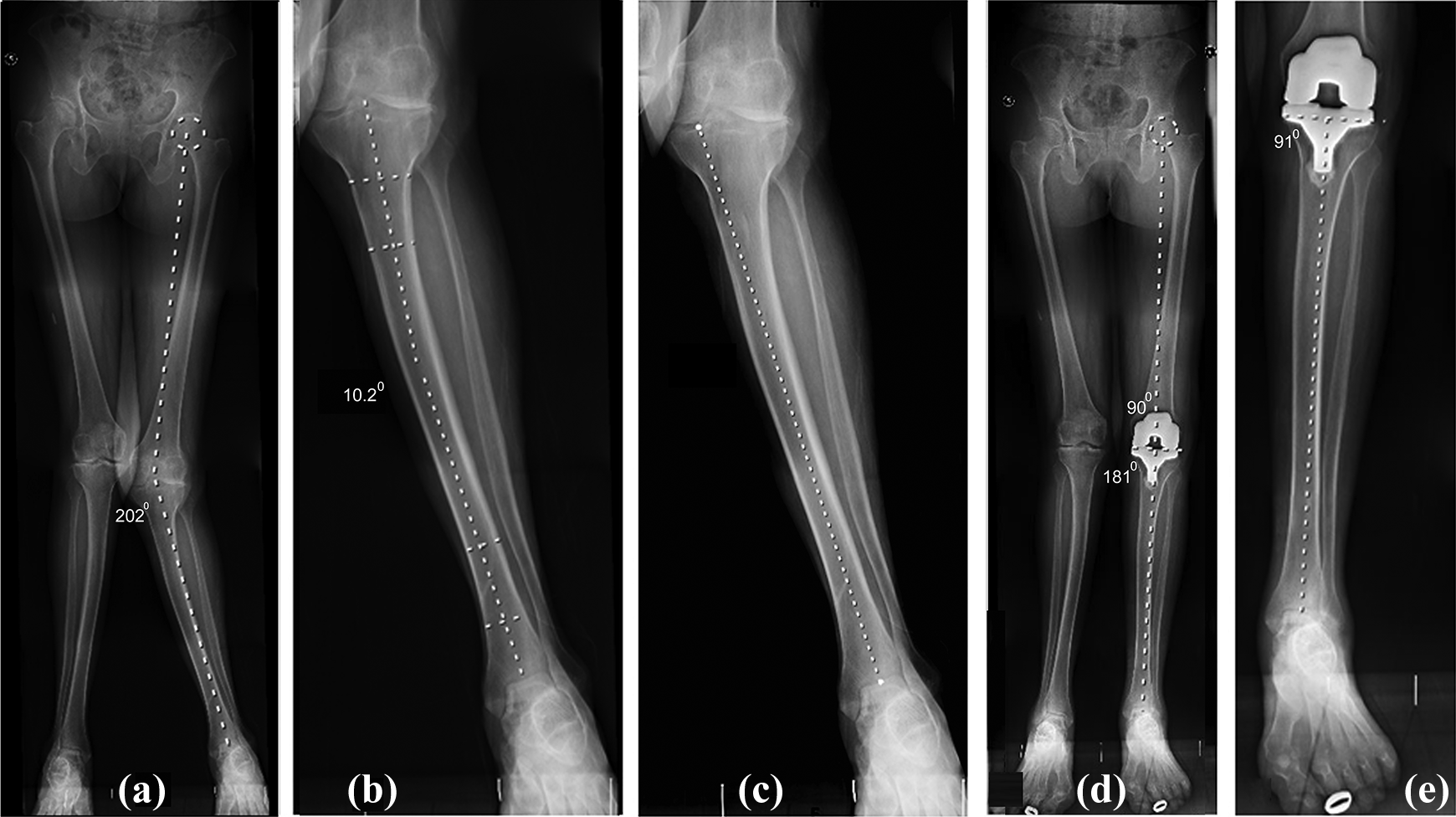
The preop and post-op angles in a bowed tibia are shown. (a) Preoperative HKA angle 202°, (b) tibial bowing of 10.2°, (c) reference point for tibial jig placement was medial to medial tibial spine, (d) post-operative HKA angle 181° and MDFA 90°, and (e) MPTA 91°. HKA: hip–knee–ankle; MDFA: medial distal femoral component angle; MPTA: medial proximal tibial component angle.
Yau et al. 14 and Ko et al. 15 observed that the use of tibial intramedullary alignment guide for proximal tibial resection resulted in unacceptable tibial cut in the presence of tibial bowing because the deformity made the passage of the intramedullary rod parallel to the tibial mechanical axis impossible. Also, the placement of tibial jig should be based on the tibial bowing. In our study population, we observed a statistically significant correlation between the degree of tibial bowing and the reference point used for tibial jig placement. Patients with tibial bowing >3° had their mechanical axis of tibia passing through medial tibial spine or even medial to it. Hence we recommend that the severity of metaphyseo-diaphyseal tibial bowing should be critically looked into during preoperative planning and the tibial jig centred over medial tibial spine may be deemed appropriate in patients with significant tibial bowing (>3°) to restore the limb alignment.
This study has few limitations. As the intervention is based on radiographic assessment errors in assessment of tibial mechanical axis due to rotation of limb can lead to wrong jig placement. We tried to minimize this error by standardizing the technique of taking full-length hip-to-ankle and knee radiographs at our institution. Alignment in sagittal and axial planes are equally important for long-term implant survival and function after TKA.
Conclusion
Medial tibial bowing is very common in valgus knees. Tibia valga has a strong positive correlation with the severity of valgus deformity. Accurate tibial component placement can be achieved with a medialized reference point for extramedullary tibial cutting jig in knees with significant tibia valga.
Footnotes
Acknowledgement
We thank Mrs. Preethi Selvaraj for helping us out with the statistical part of the study.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.