
Abstract
Purpose:
The purpose of this study was to define the fracture type and investigate the injuries related to single medial, intermediate, or lateral cuneiform fracture.
Methods:
From January 2008 to December 2018, 30 consecutive patients (30 cases) who were treated in the single institution for the single cuneiform fractures were reviewed retrospectively. Each fracture was categorized by location and type (intra- or extra-articular avulsion, axial compression, and direct blow). We also investigated the related foot bone fractures or dislocations on the affected side.
Results:
Twenty-one, one, and eight cases with single medial, intermediate, and lateral cuneiform bone fractures, respectively, were identified. More than two-thirds of the single cuneiform fractures were observed in the medial cuneiform bone. The single medial cuneiform fracture was associated with various types of foot injuries including Lisfranc injury, naviculo-cuneiform joint dislocation, or calcaneo-cuboidal dislocation. Single lateral cuneiform fractures were more frequently observed than single intermediate cuneiform fractures.
Conclusion:
More than two-thirds of the single cuneiform fractures were observed in the medial cuneiform bone. Most intra-articular avulsion fractures were associated with high-energy trauma.
Level of Evidence:
4
Introduction
Midfoot bones are secured by several ligaments and are highly constrained. Medial, intermediate, and lateral cuneiform bones, along with the base of the second metatarsal bone, provide firm support to the transverse midfoot arch. Between the medial and lateral cuneiform bones, the intermediate cuneiform bone has a strong attachment to the first metatarsal base. Therefore, fracture of the isolated cuneiform bone is an extremely rare injury. In the past, scattered case reports 1 –5 have presented a combination of injuries including Lisfranc or midfoot fracture/dislocation. Although the incidence of isolated medial cuneiform fracture is 1.7% of all tarsal fractures, 6 intermediate or lateral cuneiform fractures have been only presented as case reports. 7
In this study, we use the term “single” cuneiform fracture separately from the term “isolated.” While isolated cuneiform fractures refer to solitary cuneiform bone fractures without any further surrounding injuries, a “single” cuneiform fracture refers to not only the fracture of one of the three cuneiform bones but also a possible relation to other foot injury except those of the cuneiform bones. To reveal the pattern of each cuneiform bone fracture, we decided to analyze a single cuneiform fracture. To the best of our knowledge, there are no previous reports presenting the fracture pattern and related injuries for the single cuneiform fracture. We hypothesized that single cuneiform fracture would have its unique fracture pattern. The purpose of this study was to define the fracture type and investigate the related injuries for single medial, intermediate, or lateral fracture.
Materials and methods
Patient selection
From January 2008 to December 2018, 30 consecutive patients (30 cases) who were treated in the single institution for single cuneiform fractures were reviewed retrospectively. Twenty-one, one, and eight cases with single medial, intermediate, and lateral cuneiform bone fractures, respectively, were identified. Mean patient age was 47.1 ± 18.2 years (range 18–85) and 22 were male. The most common cause of injury was slipping while walking (13 cases), followed by being hit by a car on the road (6 cases), traffic accident while driving a motorbike (5 cases), and traffic accident while driving a car (2 cases). As a rare cause of injury, there was one case each of fall from a 2-m height, passenger traffic accident, metal-cutter injury, and direct blow injury by another player’s kick while playing soccer.
Fracture type and related injury investigation
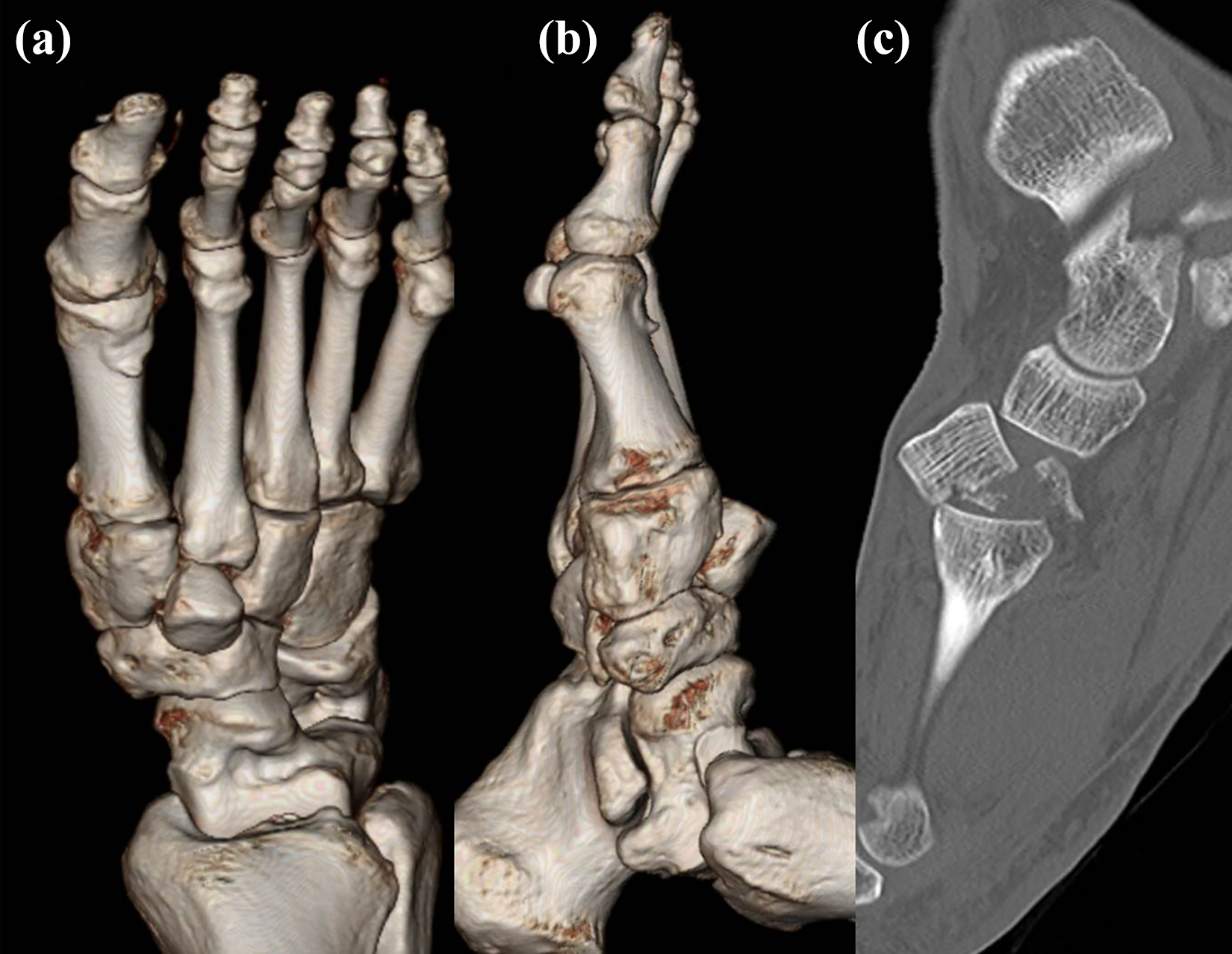
Anteroposterior, lateral, internal, and external oblique radiographs of the foot were obtained and assessed. To determine the exact features of the fracture morphology, computed tomography (CT) was performed for all included patients with a three-dimensional (3-D) reconstruction. Using 3-D CT, all fractures were divided into three types. Type 1 was avulsion fractures, which had two subtypes. Extra-articular avulsion (type 1A) included both chip bone avulsion and shell-like cortical avulsion. Chip bone avulsion was defined as a complete separation of the fragment (Figure 1(a)), whereas shell-like cortical avulsion was defined in cases where there was an attachment between the fragment and the body (Figure 1(b)). Intra-articular avulsion was defined as type 1B (Figure 1(c)). Type 2 included axial compressive fractures (Figure 1(d)) and type 3 included direct blow injury (Figure 1(e)) caused by an impaction on the dorsum of the foot.

Extra-articular avulsion (type 1A) included both chip bone avulsion (a) and shell-like cortical avulsion (b). Intra-articular avulsion was defined as type 1B (c). Type 2 comprised axial compressive fracture (d) and direct blow injury by a cutter is shown (e).
Along with the fracture-type determination, we anticipated the direction of the injury force in type 1 fractures. In type 2 fractures, we anticipated the forefoot position when the axial compressive force was applied to determine the comprehensive fracture pattern. Additionally, we investigated the related foot bone fractures or dislocations on the affected side. In particular, we focused on the existence and type of the Lisfranc injury using Hardcastle and Myerson classification. 8
Ethical considerations
Informed consent was obtained in writing from each patient before enrolling them in the study. This study was approved by our institutional ethical review committee and conformed to the guidelines of the Declaration of Helsinki.
Results
Single medial cuneiform fracture
Among the 21 cases, 10, 3, 6, and 2 cases were of type 1A, 1B, 2, and 3, respectively. In type 1A fractures, the first metatarso-cuneiform (MTC) joint dorsal avulsion fracture resulting from abrupt plantar flexion of the first MTC joint was common. We also found two cases of type 1A fractures accompanied by medial dissociation of the first ray (Lisfranc B1). Besides, first MTC volar avulsion fracture was found with the first MTC dorsal dislocation accompanied by Lisfranc A. With Lisfranc B2, we found two cases of lateral or dorsolateral avulsion on the first MTC joint.
Regarding type 1B fractures, two of three cases showed concomitant medial dissociation of the first ray (Lisfranc B1). In one case, the intra-articular avulsion was caused by naviculo-cuneiform (NC) joint dislocation. We were able to confirm that all three cases were related to a high-energy trauma.
In type 2 fractures, three of the six cases showed volar compression on the MTC articular surface, which could have resulted from axial compressive force with the forefoot in plantar flexed position. Only one case was related to divergent-type Lisfranc injury (Lisfranc C2).
There were no related injuries for all type 3 fractures. Detailed information for the single medial cuneiform fracture is presented in Table 1.
Detailed information for the single medial cuneiform fractures (n = 21).

fx: fracture; D/L: dislocation; SD: slip down; MTC: metatarso-cuneiform joint; TMT: tarsometatarsal; Add: adduction; Pf: plantar flexion; TA: traffic accident; MT: metatarsal; NC: naviculo-cuneiform; Abd: abduction; N/A: not applicable; C-C: calcaneo-cuboidal.
a Gustilo–Anderson classification was used.
Single intermediate cuneiform fracture
We found only one case of a single intermediate cuneiform bone fracture in a 62-year-old man who fell from a 2-m height. He presented a single type 2 volar compressive intermediate cuneiform fracture with dorsal dislocation. The anticipated fracture pattern was axial compression with the forefoot in plantar flexed position. No related foot injuries were noted (Figure 2).
A single type 2 volar compressive intermediate cuneiform fracture with a dorsal dislocation was noted in a 62-year-old man who fell from a 2-m height. 3D reconstruction images (A, B) show dorsal dislocation and a sagittal image shows a small bony fragment containing articular cartilage (C).
Single lateral cuneiform fracture
Among eight cases, seven cases were type 1 fractures (four cases in type 1A and three cases in type 1B). Type 1A fractures were related to adduction with plantar flexion of the lateral tarsometatarsal joint or the NC joint. We found only one case of type 1A single lateral cuneiform fracture related to Lisfranc B2. In type 1B fractures, all three cases were related to Lisfranc injuries (one case of Lisfranc A and two cases of Lisfranc B2).
One case of type 2 fracture showed total collapse of the MTC articular surface due to the axial compressive force with adducted and plantar flexed position of the tarsometatasal joint lateral to the second metatarsal bone. A concomitant nutcracker fracture of the cuboid bone was also noted.
No type 3 fractures were found in this group. Detailed information for single lateral cuneiform fracture is presented in Table 2.
Detailed information for the single lateral cuneiform fractures (n = 8).

fx: fracture; D/L: dislocation; SD: slip down; MTC: metatarso-cuneiform joint; TMT: tarsometatarsal; Add: adduction; Pf: plantar flexion; TA: traffic accident; MT: metatarsal; NC: naviculo-cuneiform; Abd: abduction.
a Gustilo–Anderson classification was used.
Discussion
Our data suggest that cuneiform fracture could be classified into three categories: avulsion, axial compression, and direct blow. Recently, Mehlhorn et al. 9 established the classification for fracture–dislocation of the cuneiform bone. The classification was as follows: isolated fracture [1], isolated dislocation [2], or fracture–dislocations [3] involving 1 [A], 2 [B], or 3 [C] cuneiform bones. Along with the old AO classification system, they added the concept of dislocation to predict the outcome more precisely. However, it is easily predictable that multiple cuneiform fractures with dislocation will show worst outcomes.
The new AO/OTA classification for cuneiform fracture 10 categorized the fractures on the basis of location (medial, intermediate, or lateral) and articular surface involvement (avulsion, partial articular, or complete articular). Practically, it is difficult to distinguish partial and complete articular involvement even with CT scans. Moreover, it is also difficult to judge which articular surface is involved with this classification system. This is the reason why we especially focus on the exact location of the fracture describing (1) articular MTC or NC, (2) dorsum or volar, and (3) medial or lateral. We would like to reveal the specific relationship between the fracture location/type and the related foot injury including Lisfranc injury.
Regarding the isolated medial cuneiform fracture, some case reports have been already presented. Eraslan et al. 11 reported that the isolated medial cuneiform fractures were extremely rare and might be missed and underestimated with conventional radiographs at initial evaluation in the emergency department. Tai 12 also reported a case report of the isolated medial cuneiform open fracture caused by direct blow injury (metallic board). Yamaguchi et al. 13 showed two cases of hidden intra-articular avulsion fractures of the lateral side of the medial cuneiform bone. They defined them as isolated, nondisplaced medial cuneiform bone fractures. However, we believe that the lateral side type 1B avulsion fracture is always associated with Lisfranc B2; therefore, these fractures cannot be defined as “isolated.” In our study, only five cases of true isolated medial cuneiform fractures were detected. Three cases were dorsal or dorsomedial type 1A avulsion fractures on the MTC joint, whereas the other two were caused by direct blow injury (type 3). Therefore, associated foot injury must be excluded, and thus CT or magnetic resonance imaging is highly suggested.
Several reports have been published about the medial cuneiform fracture associated with medial dislocations. 1 –5 Hidalgo-Ovejero et al. 14 insisted that most of the isolated dislocations of medial cuneiform were pure dislocations of the first ray (medial cuneiform and the first metatarsal), whereas only few case reports had described pure dislocation of the medial cuneiform from both navicular and first metatarsal base articulation. In our study, medial cuneiform dislocation was shown as the part of the Lisfranc A or B1 along with the avulsion fracture of medial cuneiform. Brandser et al. 15 also reported the combined Lisfranc and medial cuneiform fracture and dislocation after a heavy metal bar fell onto the foot dorsum. In their case, intercuneiform distance was preserved, whereas the first to second intermetatarsal space was widened. In our study, the single medial cuneiform fracture was associated with various types of foot injuries including Lisfranc injury, NC joint, or calcaneo-cuboidal dislocation. 16
Regarding the single intermediate cuneiform fracture, only a few case reports have been made. Hensley et al. 17 presented an isolated, nondisplaced intermediate cuneiform fracture in an ice hockey player. In their report, the patient was injured from a direct blow slap shot. Doshi et al. 7 reported a dorsal dislocation of the intermediate cuneiform bone with fracture of the Lisfranc joint. Although their case was very similar to our case, the correlated Lisfranc injury was not noted in our case.
Interestingly, there was no previous report about the single lateral cuneiform fractures. However, we found that the single lateral cuneiform fractures were more frequently shown than the single intermediate cuneiform fractures. Most of the fractures were avulsion fractures. Additionally, isolated single lateral cuneiform fractures always occurred at the dorsolateral area of the NC joint. Intra-articular avulsion was highly associated with Lisfranc injury.
The main limitation of this study was that we did not report the treatment outcomes, prognosis, or differential operative techniques according to the fracture type and location. In most of the stable cases, we did not perform the operation; only trans-articular fixation was performed for cases with Lisfranc or adjacent joint dislocations, leaving the fractured cuneiform untouched. Although the open reduction and internal fixation for cuneiform fracture itself was barely done, we believe that fracture type or location-specific operative technique could be considerable. For instance, open reduction and internal screw fixation for cuneiform fracture with a simultaneous bridging plate or external fixator from navicular to metatarsal for the lengthening might be necessary in unstable axial compressive fractures. Also, an additional bone graft could be added in this situation. Retrospective study design was another limitation of our study. A future study is recommended to summarize these differential operative techniques according to the fracture type and location. Another limitation was the small number of cases and the retrospective design. Nevertheless, this study is meaningful because, to the best of our knowledge, it is the first study that reveals the pattern and related foot injuries of the single lateral cuneiform fracture.
In conclusion, we categorized the single cuneiform fracture into three types and investigated the concomitant foot injury including Lisfranc joint. More than two-thirds of the single cuneiform fracture was shown in the medial cuneiform bone. Most intra-articular avulsion fractures were associated with high-energy trauma; therefore, careful investigation about the related injuries is highly necessary.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.