
Abstract
This study aimed to compare clinical efficacy and safety of chloroprocaine and lidocaine in epidural anesthesia for outpatient knee arthroscopy. Eighty patients undergoing knee arthroscopy were randomly allocated to receive 3% 2-chloroprocaine (group C, n = 40) or 2% lidocaine (group L, n = 40) for epidural block. Latency to anesthesia onset, highest block level, time to achieve peak effect, time to complete sensory and motor block regression, vital signs including respiration and hemodynamics, and complications during follow-up were recorded. No significant differences were found in the latency to anesthesia onset and peak effect, duration of anesthesia efficacy, and the time for recovery of sensory function between the two groups. However, the latency to maximal block of pain sensation and the time needed to recover motor function were significantly shorter in group C than in group L (p < 0.05). No adverse effects or neurologic complications were found in both groups. In conclusion, epidural chloroprocaine elicits rapid anesthetic effects, fast sensor and motor block, and faster recovery of motor function compared to lidocaine. These characteristics make chloroprocaine better than lidocaine as the choice of epidural anesthesia in short clinical operations such as knee arthroscopy.
Introduction
Outpatient surgery offers several advantages over traditional inpatient surgery, which include a shorter operation duration, relatively little trauma, faster recovery, fewer adverse reactions or complications, and earlier discharge times. Knee arthroscopy is an outpatient procedure that benefits greatly from epidural anesthesia which provides rapid and reliable anesthetic effects, predictable recovery, and minimal complications. A number of local anesthetics have been developed to meet the growing need for day case surgeries including knee arthroscopy. 1 –4
Lidocaine has been the choice of epidural anesthetic in many outpatient procedures with a rapid onset of action and long duration of efficacy. However, neurological complications associated with the use of lidocaine, collectively named the transient neurologic symptoms, have limited its use. 2,5,6 Chloroprocaine is an amino-ester type of local anesthetic and has similar recovery profile as epidural lidocaine when used as epidural anesthetic. Compared to lidocaine and other local anesthetics, chloroprocaine induces an anesthesia that is characterized by rapid onset, a very short duration of action and a favorable evolution of spinal block for short outpatient procedures. 5,7 Therefore, chloroprocaine has been proposed as an excellent candidate anesthetic and alternative of lidocaine for short procedures.
In spite of the significant advantages of chloroprocaine, the use of chloroprocaine for epidural anesthesia has proven controversial and, therefore, more studies are needed to determine clinical efficacy and safety of chloroprocaine in outpatient procedures. In this study, chloroprocaine and lidocaine were compared for epidural anesthesia in patients undergoing knee arthroscopy.
Materials and methods
Patients
This study has been approved by the Ethics Committee of Jingzhou Central Hospital. All patients provided signed consent to participate in the study. Eighty patients who underwent knee arthroscopy were enrolled. They had no endocrine or metabolic diseases or any nervous system disorders, no abnormalities in liver and kidney function, and no epidural puncture contraindications. Using a randomized, double-blind method, 80 patients were randomly divided into two groups: chloroprocaine group (group C, n = 40) injected with 3% 2-chloroprocaine (30 mg/mL, Jincheng Hayes Pharmaceutical, Shanxi, China) and lidocaine group (group L, n = 40) injected with 2% lidocaine (20 mg/mL, Xudong Haipu Pharmaceutical, Shanghai, China).
Procedures
The patients were monitored with a GE multifunction monitor to measure heart rate (HR), blood pressure, and respiratory rate. The L2–3 vertebral body gap was selected for epidural anesthesia in a lateral position and a 3.5 cm catheter was placed upward. Then, 3% 2-chloroprocaine or 2% lidocaine was injected in a 5 mL test dose with the patient in supine position. It was confirmed that the conduit was in the epidural space and there were no unwanted spinal anesthesia symptoms. Five minutes later, a 10 mL dose of 3% 2-chloroprocaine or 2% lidocaine was added. The injection speed of both groups was the same, and no other local anesthetics were added during the entire operation. After the successful epidural anesthesia puncture, oxygen was taken up through a nasal catheter at 2–4 L/min. If the blood pressure dropped to lower than 30% of the base value, 10 mg ephedrine was injected intravenously. If the HR dropped to lower than 50 beats/min, 0.5 mg atropine was injected intravenously. The two groups of patients were not given any sedation, analgesia, or other intravenous anesthetics for assistance. Patients with unsmooth anesthesia operation or uncertain effects were excluded.
Measurements
Latency to anesthesia onset (the time period from giving the test dose to the disappearance of cold sensation); latency to nerve block onset (the time period from giving the test dose to elimination of pain sensation, tested by pinprick); highest block level (determined by the disappearance of cold sensation); latency to peak effect (the time period from giving the test dose to appearance of highest block level); sensory recovery time (time period from giving the test dose to feeling pain in the surgical wound, scored ≥4 in visual analog scale (VAS)); and motor recovery time (time period from giving the test dose to recovering motor function in the lower limb joints, scored 0 by Bromage scoring method) were measured.
VAS scoring method: 0 indicates no pain, ≥4 indicates moderate pain, and the highest score of 10 represents unbearable intense pain. Bromage scoring method: 0 represents no motor nerve block (hip, knee, and ankle joints are inflective); 1 represents the inability to lift legs (but knee and ankle joints are still mobile); 2 represents the inability to bend the knee (but retention of movement in ankle joints); 3 represents the inability to move the ankle joints (all three major joints—hip, knee, and ankle—are immobile). Vital signs including blood pressure, HR, and respiratory rate were measured and monitored before anesthesia and after drug delivery at 5, 10, 15, 20, and 30 min. Patients were also monitored for adverse reactions including dizziness, nausea, vomiting, drowsiness, restlessness, unconsciousness, peripheral numbness of mouth, and nervous system complications such as hypotonia in the lower extremities or muscle, abnormal sensation, and bladder dysfunction.
Statistical analysis
Statistical analysis was performed using statistical software SPSS13. Results were presented as mean ± standard deviation. The comparison of anesthetic effects and vital signs at different time points between the two groups was determined using t-test. Changes in vital signs of both groups and the comparison of vital signs between groups before and after anesthesia were assessed using repeated measures analysis of variance. Differences in categorical variables between the groups were analyzed with χ 2 test. The value of p < 0.05 was considered statistically significant.
Results
Eighty patients were randomized into two groups. There were no dropouts or case failures in our study. Demographics including the age, gender, weight, and height were similar between the two groups and there were no significant differences in duration of operation and epidural infusion volume between the two groups (Table 1, p > 0.05). The latency to anesthesia onset and the latency to elimination of pain sensation were both shorter in group C than in group L, but the differences between the two groups were not statistically significant (Table 2, p > 0.05). Notably, the average time required to reach the highest level of sensory block was significantly shorter in group C than in group L (14.7 ± 3.4 min vs. 18.5 ± 4.8 min) (Table 2, p < 0.05). Furthermore, the average motor recovery time in group C was much faster than that in group L (76.1 ± 16.3 min vs. 85.9 ± 18.8 min) (Table 2, p < 0.05).
Summary of demographic data, duration of operation, and infusion volume (mean ± SD).a
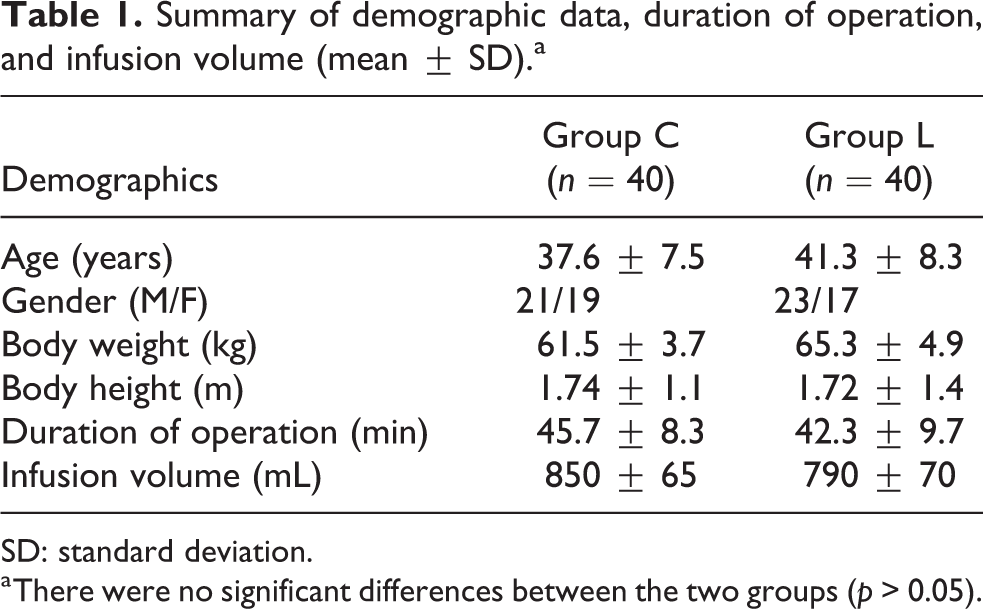
SD: standard deviation.
a There were no significant differences between the two groups (p > 0.05).
Summary of anesthetic effects and recovery (mean ± SD).

SD: standard deviation.
a p < 0.05 between the two groups.
Vital signs of patients were monitored carefully throughout the procedure. The arterial pressure (AP) of group C decreased significantly 10 min after delivery of anesthesia. In contrast, AP of group L decreased significantly 10–15 min after delivery of anesthesia, indicating a trend toward longer latency to AP reduction. Meanwhile, HR for both groups showed an upward trend and there was no significant difference between the two groups (p > 0.05). The percentages of patients experiencing side effects such as hypotension, bradycardia, sicchasia, dizziness, or backache in each group during the operation are shown in Table 3. There were no significant differences in the incidence of such side effects between the two groups (p > 0.05). In addition, no neurological complications such as paraesthesia of lower limbs and dysfunction of vesica urinaria were reported for patients in either group during the follow-up.
Incidences of hypotension, bradycardia, sicchasia, dizziness, and backache after operation.a

a There were no significant differences between the two groups (p > 0.05).
Discussion
The number of outpatient small surgeries has greatly increased in recent years due to the advance in technologies. The growing popularity of outpatient surgeries calls for effective and safe local anesthetics. The ideal anesthetics should exhibit features such as rapid and reliable anesthetic effects with minimal to no toxicity. Chloroprocaine has been widely used in infiltration anesthesia and nerve block worldwide, 8,9 and is especially applicable to outpatient procedures and daytime surgeries. 1,4,10 In particular, chloroprocaine was used for epidural block and subarachnoid space block. 5,11,12 Neal et al. applied chloroprocaine or lidocaine epidural anesthesia to short-duration minor orthopedic operations of the lower limbs. 13 Casati et al. compared the efficacy of chloroprocaine and lidocaine for spinal block in knee arthroscopy. 5 In both studies, the group receiving chloroprocaine required less time in the observation room following the operation. Yoos and others compared the spinal anesthesias using 40 mg of chloroprocaine and 7.5 mg of lidocaine and found that the surgeries for patients receiving chloroprocaine were more likely to fit in the expected time frame, allowing patients to be discharged from hospitals earlier. 14
With accumulating evidences supporting the application of epidural chloroprocaine in outpatient surgeries, this study aimed to test the hypothesis that chloroprocaine provides similar effective sensory block but a faster recovery of motor function compared to an equivalent dose of lidocaine in Chinese patients. The results of our study indicate that 3% chloroprocaine had a slightly faster onset of anesthetic effect compared to 2% lidocaine in patients undergoing outpatient knee arthroscopy. Chloroprocaine required significantly shorter time to reach the maximal sensory blocking effect than lidocaine. The time for sensory recovery is comparable between the groups receiving chloroprocaine and lidocaine, making them both ideal for knee arthroscopy and other short surgical procedures of ≤1 h. However, the motor function of the group receiving chloroprocaine recovered significantly faster than the group receiving lidocaine following the emergence of pain sensation. The faster motor recovery may be explained by the fact that chloroprocaine can be locally hydrolyzed by cholinesterase. 15 The rapid metabolism of chloroprocaine also contributes to less toxicity.
In our study, anesthesia caused a decrease in AP and an increase in HR for both groups of patients. Thus chloroprocaine elicits the same effect on the circulatory system as lidocaine and other local anesthetics, which block the intraspinal sympathetic system to reduce blood pressure and increase HR. During the operation, the incidences of hypotension, bradycardia, sicchasia, dizziness, and backache were very low and unwanted side effects were similarly infrequent in both groups. Early reports indicated that a large dose of chloroprocaine applied outside the dura mater would lead to severe spastic backache. 16 This adverse effect may be related to the permeation of local anesthetics into human tissues by needle passages after a large dose of medicine being injected. More recent reports showed that when appropriate dose of preservative-free chloroprocaine was used for spinal block, no serious backache and very rare complications were observed. 4,5,8 In our study, the incidence of backache in both groups was very low (1 in 40 patients), consistent with other reports. According to follow-up visits within 24 h and 1 week after the operation, patients from either group experienced no obvious complications related to neurotoxicity, consistent with other reports. 3,4,17
In conclusion, our study provides additional evidence to support the hypothesis that chloroprocaine is a better alternative to lidocaine in epidural anesthesia. Chloroprocaine exhibits characteristics of rapid onset, defined efficacy, rapid motor recovery, minimal toxicity, and lack of adverse reactions. Therefore, chloroprocaine is a good anesthetic option for patients undergoing small outpatient procedures such as knee arthroscopy. With shorter surgical procedures, faster recovery time, and decreased risk of complications, the patients do not need to stay in the hospital for prolonged observation. Our findings support the use of the epidural chloroprocaine in ambulatory knee arthroscopy.
Footnotes
Author contributions
ZY and DL equally contributed to this work.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.