
Abstract
Purpose:
Tibial tubercle osteotomy (TTO) is a surgical technique used in the management of severe fractures of the knee joint and revision total knee arthroplasty. Limited research discusses the performance of the osteotomy and fixation of the TTO with screws. Therefore, this study investigated the effects of fragment shape and screw configuration on the mechanical behavior in the fixation of the TTO using the finite element (FE) method.
Methods:
FE TTO models with three fragment shapes and three screw configurations were developed. The three fragment shapes were a step cut, bevel cut, and straight cut. The screw configurations were two parallel horizontal and downward screws and two trapezoidal screws. A 1654-N upward tension force was applied on the tibia tubercle, and the distal end of the tibia was completely fixed.
Results:
The results indicated that the step cut resulted in higher stability than the bevel and straight cut, but the stress was higher as well. Among the screw configurations, two parallel downward screws resulted in the highest stability, given the same fragment shape. In the horizontal configuration, the step cut tibia developed the largest contact force to achieve stability of the bone fragment under loading.
Conclusion:
The fragment shape with a step cut and fixation with two parallel horizontal or downward screws are suggested for TTO, while the trapezoidal screw configuration is not suggested. Furthermore, the downward screw configuration is a suitable strategy to reduce bone stress.
Introduction
Tibial tubercle osteotomy (TTO) is a surgical technique used in many surgeries around the knee joint, including reduction and fixation of severe fractures of the distal femur and proximal tibia, revision total knee arthroplasty, and management of malaligned patellar tracking and patellofemoral incongruence. 1 –5 TTO is gaining popularity because of its advantages, including greater exposure and a larger field, negligible soft tissue violation, and predictable recovery through bone healing. 6 –10 However, complications, including the fracture and proximal migration of the osteotomized bone fragment and postoperative extensor lag, are associated with the fixation of the TTO. 11 –14 Most complications involve the bone fragment, but little is known about the relationship between the shape of the osteotomized tubercle fragment and the TTO stability or bone stress. In addition to the fragment shape, the screw configuration is critical to stability, but rarely investigated.
Koëter et al. suggests a straight cut for the tubercle fragment to avoid a stress riser in the tibia. 15 However, the bone stress and screw configuration were not considered in the study. Davis et al. demonstrated that applying a step cut to the fragment resulted in higher stability than applying a bevel cut with wire fixation of the TTO. 16 However, the screw configuration and the bone stress were again ignored. In clinical practice, the surgeon cuts the fragment with an insertion angle between 30° and 45° to the tibial axis and an insertion site above the insertion of the patellar tendon. 17 Fragment shape in TTO remains controversial and few evidence-based studies reveal the effect of fragment shape on the bone stress and stability of the TTO. The parallel horizontal screw configuration is currently used in TTO fixation and demonstrates an acceptable union rate 16,18 ; however, in many clinical cases, surgeons must change the trajectory of the screw based on the bone quality or implant geometry, such as long tibial stems in revision total knee arthroplasty, to achieve a favorable outcome. 17,19,20 Two parallel horizontal screws are typically considered in cadaveric studies, and other screw configurations, such as downward and trapezoidal, are rarely studied.
It is difficult to detect the internal stress of the tibia. Furthermore, contact forces between the bone fragment and the screws or tibia are difficult to obtain, because no sensor is sufficiently small to place in the bone without destroying it. The finite element (FE) method is a numerical method that can calculate internal stress without a sensor. The FE method is robust and used in many orthopedic studies concerning complex geometry, nonlinear material properties, and complex contact behaviors. 21 –23 Therefore, this study investigated the effects of fragment shape and screw configuration on the mechanical behaviors of the TTO, including fragment stability, fracture-gap opening, contact force between the fragment and tibia, and internal stress of the bone, using the FE method. Clarifying the effects of fragment shape and screw configuration in TTO can help surgeons provide favorable fixation strength for the patient for early rehabilitation.
Methods
Solid model
An intact tibia model was developed based on open-source computed tomography images from the Visible Human Project (from the United States National Institutes of Health), and all methods were in accordance with relevant guidelines and regulations. The images were captured at an interval of 1 mm, and the contours of the bone, retrieved according to their gray values with Avizo Version 6 software (VSG SAS, Bordeaux, France), were used to render the solid tibia model. Then, the solid tibia model was edited to smooth the complex bony surfaces for the mesh in FE modeling. The model was imported into Solidworks 2014 (Dassault Systemes SolidWorks Corp., Waltham, Massachusetts, USA) to create the TTO and screw implantation. Three previously described fragment shapes, step, bevel, and straight cut, were used in the present simulation (Figure 1). 15,16 The angles between the superior cutting plane of the fragment and vertical cutting plane of the tibia were 0°, 45°, and 90° for the straight, bevel, and step cut, respectively. The osteotomized fragment was sectioned through Boolean operation with lengths from 62 mm to 78 mm and a thickness of 10 mm 13,16 ; no gap existed between the fragment and the tibia. Two full-thread cortical screws (outer diameter 4.5 mm, Synethes, Pennsylvania, USA) were used to stabilize the fragment, and three screw configurations were simulated: two parallel horizontal screws with an interval of 20 mm, two trapezoidal screws with an angle of 45°, and two parallel downward screws with an interval of 15 mm (Figure 2(a)). The screw lengths were 45 mm (VA401.054) and 74 mm (VA401.074) for the horizontal and diagonal screws, respectively. The screws were bi-cortical fixation in each screw configuration.
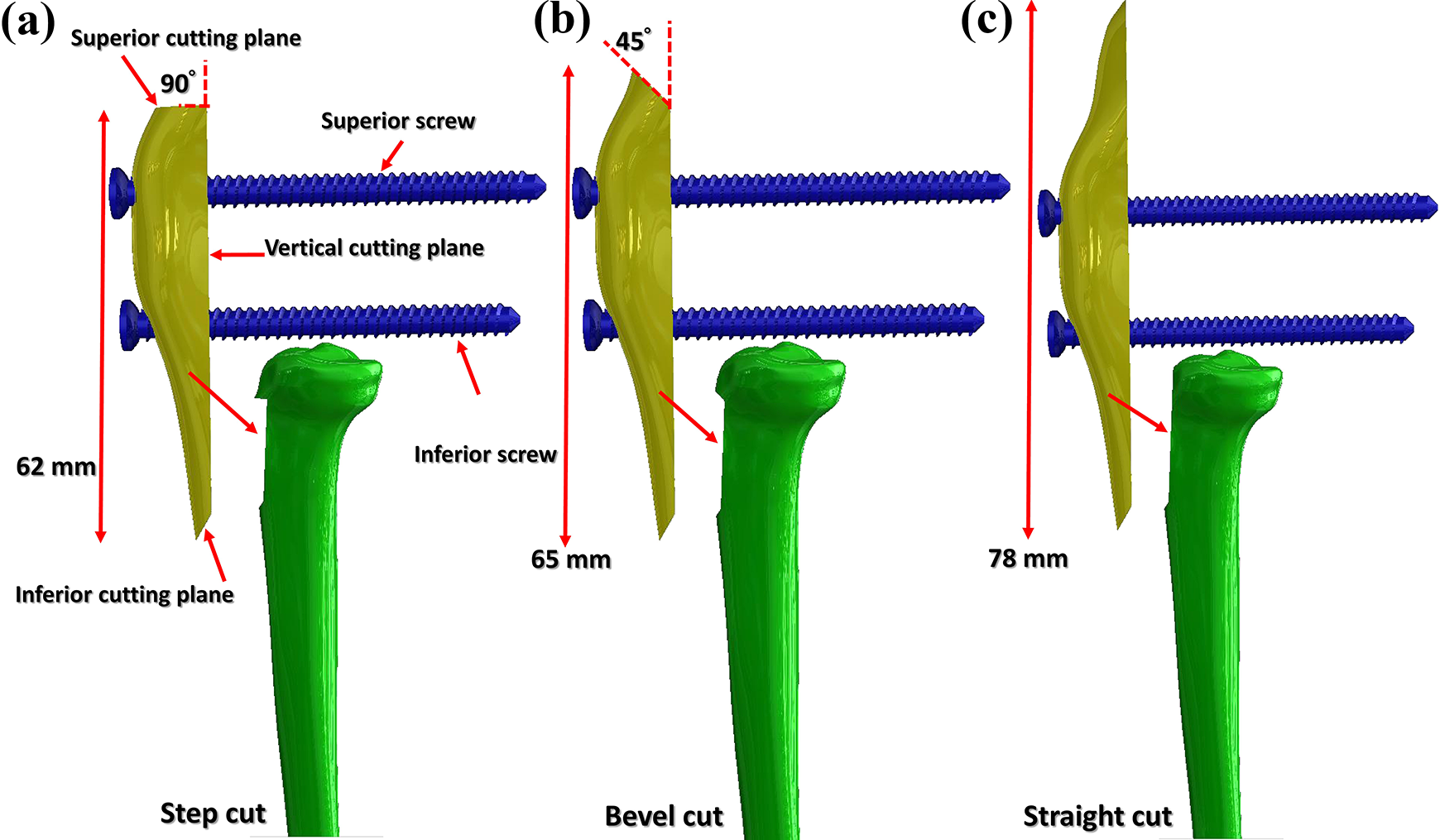
Fragment shapes used in this study: step cut (a), bevel cut (b), and straight cut (c).

Screw configurations (a), boundary conditions (b), and free-body diagram (c).
Finite element model
The models were imported into ANSYS Workbench 17 (Swanson Analysis Systems, Inc., Houston, Pennsylvania, USA) for meshing and simulation. All the parts, including the bones and screws, were meshed with quadratic tetrahedral elements (solid 187) to achieve a balance between accurate calculation and computing time. The mesh densities in the bone fragment, the areas of the tibia in contact with the bone fragment, and the screws were locally refined by setting the element length to 0.75 mm with the “sizing” command in Workbench. The global element size was set to 2 mm. In total, 386,261 nodes and 253,330 elements were used in the model with the straight cut and horizontal screw configuration; this mesh setting was applied to the other models. Contact behaviors between the screws and the surrounding bones (metal-to-bone) and between the fragment and the tibia (bone-to-bone) were defined as frictional surface-to-surface contact behavior (contact174 and target170, ANSYS). The coefficients of bone-to-bone and metal-to-bone contact were set to 0.46 and 0.3, respectively. 24
Material properties and boundary conditions
Young’s modulus of the cortical bone and cancellous bone were set to 12.6 GPa and 457 MPa, respectively, and their Poisson’s ratio was set to 0.3. 25 –27 The screws were titanium; therefore, Young’s modulus was set to 110 GPa and the Poisson ratio was set to 0.3. 28 All materials were assumed to be linear elastic, isotropic, and homogeneous in this study. A 1654-N upward force, divided into eight vectors on eight small areas, was directly applied on the tibial tuberosity to simulate patellar tension force. 16 The entire superior surface of the tibia was set to compression-only support, and the distal end of the tibia was completely fixed (Figure 2(b)). Compression-only support means the surface could bear only normal force, instead of tension force, to simulate resistance from the distal femoral condyle. The purpose of this application was to mimic a worst-case condition in which the tibia is under great tension when the quadriceps muscle contracts (such as when standing or stepping up), and the bilateral end of the tibia is constrained by the distal femur and the ankle joint. The magnitude of the force was based on failure loads in the literature. 16
Comparison incidence
The maximum displacement of the fragment and gap opening (between the fragment and the tibia) were used to evaluate the stability of the TTO with various fragment shapes and screw configurations. The magnitude of the contact forces, developed by the tibia and screws for static balance, on the tubercle bone fragment (Figure 2(c)) is critical to fragment stability. The stress of the bone is an index of the stress fracture of the TTO with various screw configurations and fragment shapes.
Validation
To validate the present model, the result regarding osteotomy displacement from the TTO model with two horizontal screws was compared with Davis’s experimental result. 16 Cadaveric knees were used in Davis’s test to compare the difference of osteotomy displacement between screw and wire fixations. The fixation of bevel cut in Davis’s test was similar to the present study; therefore, the result of bevel cut osteotomy was used for validation. Because the experimental setting of Davis’s study, lacking constraint from the distal femur, was different from that of the present simulation, the constraint of compression-only support was excluded in the TTO model validation. The osteotomy displacements were 5.7 and 6.9 mm (standard deviation, 3.1 mm) in the present study and Davis’s study, respectively.
Results
Fragment displacement and gap opening
The results indicated that the step cut resulted in the highest stability, exhibiting a smaller fragment displacement and fracture gap opening than the bevel and straight cuts in identical screw configurations (Figure 3; Table 1). Furthermore, the displacement of the bone fragment and the fracture gap opening with the bevel cut were smaller than those with the straight cut. Among the screw configurations, the downward screw configuration resulted in the smallest fragment displacement and gap opening, given identical fragment shapes. The maximum differences of fragment displacement among the screw configurations were 0.65 (0.33–0.98) mm, 0.27 (0.26–0.53) mm, and 0.22 (0.24–0.46) mm for the straight, bevel, and step cuts, respectively.

Total displacement of the fragment with the straight (a), bevel (b), and step cuts (c).
Maximum gap opening (mm) for each fragment shape under various screw configurations.

Contact force on the bone fragment
The superior cutting plane of the tibia with the step and bevel cuts generated a great contact force on the fragment for stability under the applied force, while the screws provided the largest force for the fragment in the straight cut (Table 2). The contact force on the superior cutting plane of the fragment from the tibia was lower with the bevel cut than with the step cut. This force in the trapezoidal and downward configurations was lower than that in the horizontal screw configuration, given identical fragment shapes. The maximum difference of the contact force between the screws and the superior cutting plane was lower in the two parallel screw configurations than in the trapezoidal configuration, given identical fragment shapes (Table 2). With the step cut, the contact forces on the superior cutting plane of the bone fragment were 1431 N, 1134 N, and 997 N, respectively, while the screw contact forces (superior screw plus inferior screw) were only 169 N, 464 N, and 572 N, respectively.
Force (N) on the bone fragment after static balance of the TTO.

TTO: tibial tubercle osteotomy.
Maximum principle stress
The step cut resulted in the highest tibial stress near the superior corner (Figures 4 –6), while the straight cut yielded the lowest stress of the tibia. The parallel horizontal screw configuration led to higher stress of the tibia than the trapezoidal and downward configurations, given an identical fragment shape. The maximum principle tibial stress was 238, 88.2, and 48.8 MPa with the step, bevel, and straight cut, respectively, in the horizontal configuration.

Maximum principle stress of the cutting plane of the tibia with the straight cut under various screw configurations.

Maximum principle stress of the cutting plane of the tibia with the bevel cut under various screw configurations.

Maximum principle stress of the cutting plane of the tibia with the step cut under various screw configurations.
Discussion
This study used FE methods to demonstrate the effects of the tubercle fragment shape and screw configuration on the mechanical behaviors of the TTO: stability (fragment displacement and gap opening), contact forces on the fragment, and bone stress. Understanding the contact forces on the fragment with various fragment shapes is helpful to ensure fragment stability. Furthermore, screw configuration in TTO was demonstrated to affect the fragment stability, contact forces on the fragment, and bone stress. The surgeon can adjust the force ratio of the screws and bone using different fragment shapes and screw configurations to achieve a favorable outcome.
The superior cutting plane of the tibia is critical to the fragment stability, because this plane, especially with the step cut, provides a physical barrier preventing fragment migration under sustained pulling force from the patellar tendon. Even when this plane is not perpendicular (bevel cut) to the applied load, it increases the fragment stability by reducing the fragment displacement and gap opening. By contrast, with a straight cut without the superior cutting plane, no solid barrier exists on the tibia to prevent the bone fragment from migrating under load; only the screws inhibit the movement of the fragment. Therefore, the fragment displacement and gap opening increase. Screw direction is another factor affecting fragment stability. The reduced fragment displacement with oblique screws (downward and trapezoidal) was attributed to the applied load generating both axial load and a bending effect on the screws. Only a bending effect, without axial load, was generated on the horizontal screw. From a mechanical viewpoint, screws resists axial load more than bending and therefore the oblique screw provides greater stability than the horizontal screw. Furthermore, the fixing point of the oblique screw is at a more distal position on the fragment than the horizontal one is. The distal end of the fragment migrates most. Therefore, when the screw is closer to the distal end of the fragment, the fragment migration is smaller.
The superior cutting plane and the screws are vital to the equilibrium of the fragment. With the step cut, the superior cutting plane shares a substantial amount of the load (1431 N) with the screws. Again, that evidences the importance of this plane to the fragment stability, because this plane receives 86.5% of the applied load. Even for the fragment with the superior cutting plane at 45° relative to the tibia, the contact force (1059 N) is still high. By contrast, with the straight cut fragment (without the cutting plane), the screws receive almost all the load on the fragment; therefore, the load on the screw is greater than that for the cuts with the superior cutting plane. From a mechanical viewpoint, force distributed across a large area instead of the screw is a more favorable outcome.
Among the screw configurations, the trapezoidal screw configuration resulted in force concentrating more on one screw than the two parallel (horizontal and downward) screw configurations. This force was particularly high (1145 N) with the straight cut fragment. Force concentration on one screw, from a mechanical viewpoint, raises the risk of screw rupture or bone failure near the screw. Therefore, the trapezoidal screw configuration is not suggested for clinical practice. If the surgeon must use the trapezoidal screw configuration for unavoidable reasons, such as osteoporosis, then the protection period must be sufficiently long to enhance the bone healing to bear load. Although the load on the superior cutting plane of the tibia is relatively high in horizontal and trapezoidal screw configurations with the step cut fragment, force on the bone is much safer than that on the metallic screw. This appropriate allocation of force promotes the healing of the fractured bone. 29,30
Screw configuration is a vital consideration for surgeons, because it affects the stability and stress of the TTO. The configuration of two horizontal screws is currently used in clinical practice to attain favorable results. Although the maximum principle stress of the tibia, fragment displacement, and gap opening with the horizontal configuration are higher than those with the trapezoidal and downward screw configurations, horizontal screw insertion is easier to conduct with sufficient strength than oblique screw insertion. In the case that two horizontal screws are inadequate, diagonal downward screws are suitable for the fixation of the TTO.
The step cut indeed leads to a stress riser at the superior corner of the tibia, in accordance with Koëter et al., 15 while the straight cut leads to another high-stress area at the inferior region in the fragment slot of the tibia. The cause of this high stress is that the superior cutting plane sustains a large load. The geometrical change near the corner also causes high stress. Despite the high tibial stress with the step cut, this cut provides high stability of the fragment. Davis’s cadaveric study demonstrated the same stability tendencies as this study; the step cut resulted in higher stability than the bevel cut. 16 Each fragment shape has distinct advantages in stability and stress. Therefore, in clinical practice, the surgeon must decide the fragment shape and screw configuration to achieve a balance between stability and potential for stress risers.
This study has some limitations. First, the morphology of the trabecular structure was simplified. The real contact between the screw and bone is much more complex. Second, the cutting plane was completely smooth, but in clinical practice, small irregularities are unavoidable during osteotomy. Third, only patellar tendon force was considered. Other constraint forces from the surrounding soft tissue, such as the ligament and joint capsule, were not considered. Fourth, relatively simple fragment shapes as well as screws configurations were applied in this study. Certain clinical scenarios like the tibial prostheses during revision procedures and the common tubercle translation in the correction of patellofemoral disorders were not considered due to these more complex, specified conditions might affect the strength of TTO fixation with screws though they are worthy of our future work. Finally, all material properties were assumed to be homogeneous and linear elastic; nonlinear effects, such as viscoelastic and anisotropic, were not considered.
Conclusion
This is the first study to investigate numerically the mechanical behaviors of the TTO with various fragment shapes and different screw configurations. Results suggest that the fragment shape with a step cut and fixation with two parallel horizontal or downward screws are suitable for the TTO. The trapezoidal screw configuration is not recommended. Furthermore, the downward screw configuration is a suitable strategy to reduce the stress of the bone.
Footnotes
Authors’ note
This article does not contain any studies with human participants or animals. This manuscript was edited by Wallace Academic Editing.
Acknowledgements
The authors acknowledge Chi-Mei Medical Center (Taiwan) for the support (CMNCKU10613) to this study. The authors also acknowledge the United States National Library of Medicine (NLM) and the Visible Human Project for the image data used to create the numerical model in this study.
Author contributions
Y-NC and C-WC contributed equally to this study.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.