
Abstract
Purpose:
The purpose of this study was to assess the impact of developed minimally invasive operation such as the partial lateral facetectomy (PLFE) with patella thickness resection in patients with lateral patellofemoral (PF) osteoarthritis on short-term clinical and radiographic outcomes.
Methods:
This is a prospective study of 27 knees in 27 patients (18 females and 9 males, mean aged at surgery 59.1-year old) whom a PLFE with patella thickness resection using developed minimally invasive method was performed. Data of preoperative and postoperative questionnaires, physical examinations, and radiographs were analyzed. The minimum follow-up was 12 months (mean, 24.1 months; range, 12–36 months).
Results:
The subjective outcomes included the anterior pain relief assessed by scores using the Western Ontario and McMaster Universities Arthritis Index score (scores improved considerably by 2.34 points with respect to pain and by 1.63 points with respect to function), visual analog scale, and Knee Society Score (that improved in 78% of the knees). The majority of these patients experienced improvement in their PF symptoms. The PF index decreased considerably after surgery. The mean patellar width and thickness were decreased after surgery, maintaining a width/thickness ratio of 1.8:1.0 after surgery.
Conclusion:
PLFE with patella thickness resection aiming to decrease the high pressure in the lateral facet and improving congruence of the patella confirmed frequent pain relief. This surgical procedure is minimally invasive, relatively simple, and effective in selected patients and can be a valid early alternative to more complex operations. Level of Evidence: Level IV Therapeutic study.
Keywords
Introduction
Patellofemoral osteoarthritis (PFO) is a relatively common condition in men and women older than 55 years, with an estimated prevalence of 11% and 24%, respectively. 1 Isolated PFO occurs in 9% of patients over 40 years of age, 1 –3 most frequently involving the lateral facet of the patella up to 89% of all of PFO. 2,4 Excessive lateral pressure syndrome (ELPS) and permanent lateral subluxation lead to lateral PFO. 4 Valgus alignment increases the risk for progression of osteoarthritis (OA) in the lateral patellofemoral (PF) compartment as well as other factors, such as patella dysplasia, tibial malrotation, or direction and magnitude of quadriceps loading, trochlear dysplasia, or disorders of the patellar tilt and shift. 2,4 –7
There are various options of treatment offered for PFO not sufficiently justified by the literature (conservative therapy, nonarthroplasty procedures, and arthroplasty (PF arthroplasty, and total knee arthroplasty (TKA)) treatment). 3,8 –10 There is a wide range of surgical procedures that may be offered to patients with PFO, once conservative treatment fails. 3,8 The success of surgery highly depends on the technique and patient selection. The purpose of surgical treatment of the patellar articular surface is to relieve pain and preserve the mechanical advantage of the patella for normal knee function. Patellectomy was one of the first surgical procedures performed for PFO. However, awareness of the importance of the biomechanical role of patella led to the development of alternative surgical procedures. Partial lateral facetectomy (PLFE) was initially proposed to treat PFO by Martens and De Rycke 11 and has been previously shown as a relatively simple and effective treatment modality for PFO and patellar chondrosis. 8,9,12,13 Some authors have employed this technique alone 12,14 or in combination with medialization of the tibial tubercle, 9 with Insall’s realignment procedure. 15
The emergence of diagnostic and surgical technologies using arthroscopic instrumentation has opened up new opportunities for improving the diagnosis and treatment of knee joint lesions. 16
In the present study, we developed a new minimally aggressive method of treatment for PFO (resection of lateral facet and thickness of the patella with the formation of new PF contour using arthroscopic technique) and investigated whether a satisfactory outcome can be achieved with this method, thus delaying TKA. This is of particular interest in middle-aged active patients with isolated PF arthritis.
Material and methods
Patients
This is a descriptive, observational prospective case series study that was conducted to estimate clinical and radiological aspects in 27 patients (27 knees) who received minimally aggressive surgical treatment according to the method developed by us (Kazakhstan patent application No. 2017/0102.1) on the basis of the Traumatology and Polytrauma Department, City Hospital #1, Pavlodar, Kazakhstan, between 2015 and 2018 (Table 1).
Preoperative clinical and radiographic characteristics of patients.
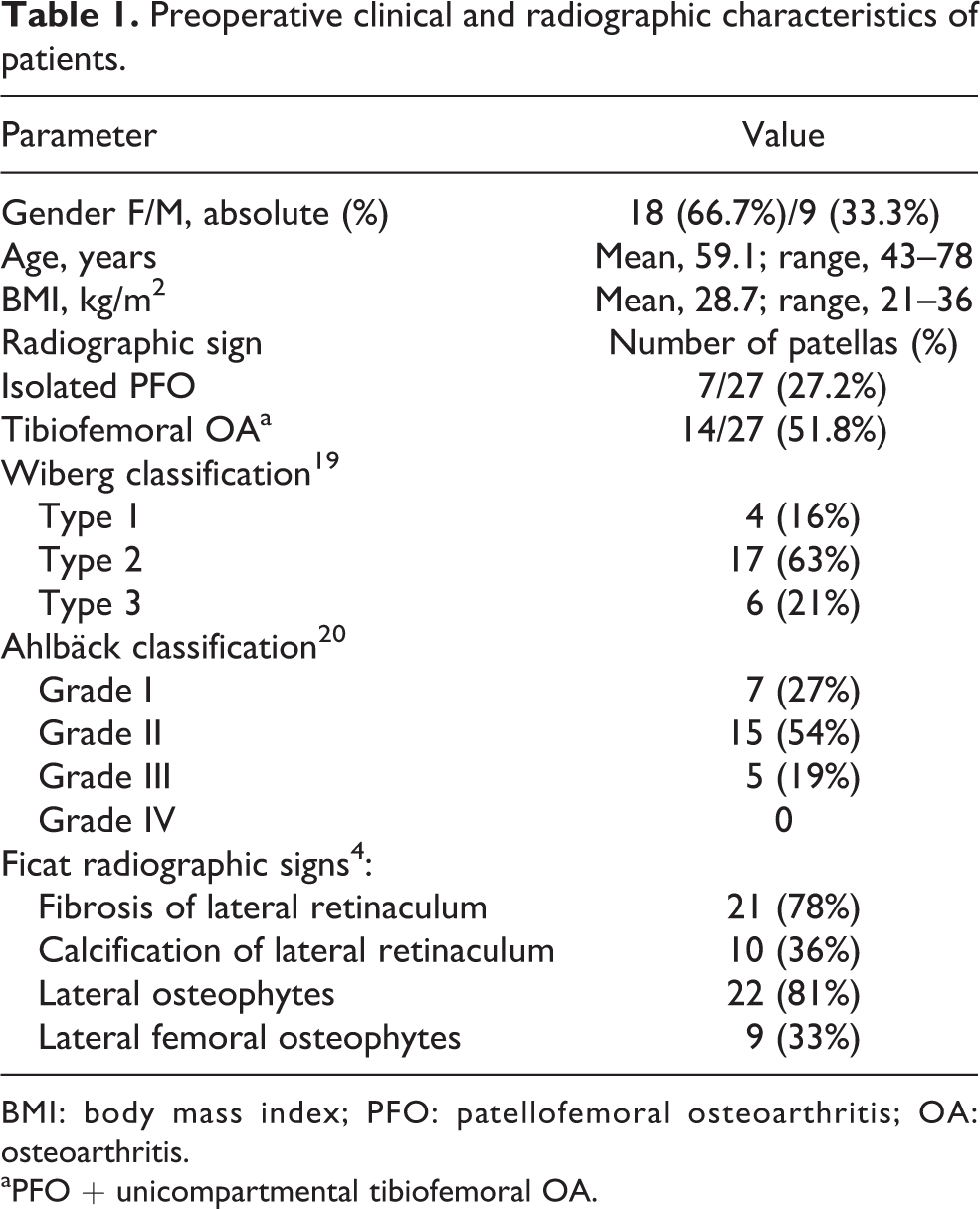
BMI: body mass index; PFO: patellofemoral osteoarthritis; OA: osteoarthritis.
aPFO + unicompartmental tibiofemoral OA.
The study was performed in accordance with institutional guidelines for human research and the principles of the Declaration of Helsinki. Study protocols were approved by the Ethics Committees of Semey Medical University and City Hospital #1, Pavlodar, Kazakhstan. All patients gave written informed consent and permission to publish deidentified data.
All patients reported sit to stand with PF pain and stairs with pain ranging from moderate to severe before the surgery causing a significant limitation of activity. This was a clinical symptom that was required as an indication for surgery. Conservative treatment in all patients for at least 6 months was attempted without satisfactory results. Subjects were excluded if they had a previous patellar dislocation, patellar fracture, tibiofemoral OA, inflammatory or rheumatoid disease of the knee, and infectious arthritis.
A thorough anamnesis and physical and radiological exams were performed in each patient prior to and after surgery. Clinical signs of the postoperative period were monitored. The minimum follow-up period was 12 months (mean, 24.1 months; range, 12–36 months). Surgery was performed by two senior orthopedic surgeons (KRA and KTA) at the department.
The patients were assessed preoperatively and postoperatively with the Western Ontario and McMaster Universities Arthritis Index (WOMAC) score, 17 and a visual analog scale (VAS) of pain 18 and knee function was assessed through the Knee Society Score (KSS). 14 The clinical assessment was performed by an independent examiner (SS) who had not seen the patients previously.
The radiographic studies included posteroanterior flexion weight-bearing views, lateral views, and axial views in 45° and 90° of knee flexion. Analysis of the radiographs on the axial views can estimate indirect signs of ELPS or excessive lateral ligamentous tension according to the criteria described by Ficat, 4 the morphological Wiberg’s patella types, 19 and the extension and grade of PFO. We assessed the medial and lateral compartments by measuring the shortest distance between the femur and tibia and classified the joint space according to Ahlbäck, 20 using the posteroanterior 45° weight-bearing view. To measure the depth of the trochlea, the sulcus angle was used which is considered normal if approximately equal to 138° ± 6° by Merchant. 21 The congruence angle measures the position of the patella in relation to the center of the trochlear groove. The PF index provides information regarding the thickness of the medial and lateral PF space. The smallest distance was measured between the medial and lateral facet of the patella to the medial and lateral aspect of the trochlea, respectively. The patellar thickness was measured from the anterior surface of the patella to the median ridge at the proximodistal center of the median ridge. We also made measurements of the patellar width, width:thickness ratio (Figure 1).

Preoperative MRI image of the left knee: a line drawn across the widest points of the patella (the patellar horizon, patella width) and patella thickness line; a lateral facet of the patella including lateral osteophyte and PF space narrowing are marked with arrows. MRI: magnetic resonance imaging; PF: patellofemoral.
Statistical analysis
Quantitative variables were described with mean and standard deviation (SD) and range; and qualitative variables described with absolute percentages. The Wilcoxon test was used to determine differences between the preoperative and postoperative clinical and radiographic outcomes. The bivariate analysis included χ 2 test for qualitative variables, Student’s t-test for mean comparison, and Pearson’s correlation coefficient for quantitative variables. Differences were considered significant with a two-tailed p < 0.05. All statistical tests were performed using SPSS software version 23.0 (SPSS Inc., Chicago, Illinois, USA).
Surgical technique
We performed the surgical procedure with the patient supine. After induction of anesthesia and administration of prophylactic antibiotics, a tourniquet was placed as high on the thigh as possible and inflated to 300 mmHg on the affected leg.
First step. Under the control of the electro-optical transducer (Siemens Arcadis Varic C-Arm; Soma Technology, Inc., Bloomfield, Connecticut, USA) in pulsed fluoroscopy regimen with average exposure time 5–10 s through the patella in the longitudinal direction in the sagittal plane, a series of Kirschner’s wires (K-wires) were conducted (Figures 2(a) and (b) and 3(a) and (b)). With the help of cannulated drills of different diameters (No. 6–8), the subchondral layer of the patella width was resected along the knitting wires (Figures 2(c) and 3(c) and (d)) to remove the bone substance, the damaged joint surface, and thickness of patella. Wires were removed. Conducting a wire through the lateral facet of the patella and using a larger diameter drill (up to 1 –1.2 cm) (No. 8–12) provides a resection of the lateral facet of the patella and an extension and release of the lateral retinaculum, resulting in medialization of the patella. There was no significant soft tissue damage during the introduction of K-wires. A skin incision (10 mm) was made above the insertion point of the K-wires. The fibers of the quadriceps tendon are bluntly apart in the longitudinal direction along the fibers. The defender of soft tissues from the drill is installed on the wire next to the bone of the patella, therefore drilling prevents tearing and winding of soft tissues on the drill. Electro-optical transducer (EOT) turned on only during K-wires insertion points localizing resulting in short irradiation time, since the EOT is switched on in a pulsed mode only to determine the points of introduction of the K-wires. The main difficulties arise when conducting the first K-wire, which must be carried out through the lateral edge of the patella in the longitudinal direction, further is only necessary to determine the point of pricking of the subsequent K-wires that run in parallel to the first K-wire in the longitudinal direction at different levels according to the subchondral layer of the patella. Totally, the mean time of radiation exposure during the operation of patient was approximately 10–15 min.
Second step. The arthroscopy of the knee joint through standard points was performed (Arthroscope, Richard Wolf GmbH, Knittlingen, Germany). The final processing of the patella contour is made with the formation of conformity in the PF joint (the shaving bone removes bone cartilage and remains on the patellar articular surface, in the region of the upper and lower poles of the patella and femur; Figures 2(c) and (d) and 3(e) and (f)). The condylar osteophytes were then excised and the edge of the patella smoothed. A shaver can be used to remove the debris while trimming the lateral patellar facet. It is of utmost importance to cautiously resect any remnant bony sharp edges that can impinge on the trochlear surface during knee motion. In addition, the lateral patellar retinaculum is carefully preserved so that iatrogenic medial patellar instability does not occur. The knee is dynamically reevaluated (through flexion and extension and with medial excursion) for residual impingement and to assess for improvements in patellar mobility (Figure 3(g) and (h)). Patellar tracking is assessed to verify that there is no catching in flexion and that patellar mobility is improved. If any impingement does remain, it can be addressed at this point. Hemostasis is performed with a radiofrequency probe to minimize postoperative bleeding. After profuse irrigation, lastly, the portals are closed and the skin wounds were sutured. A sterile compressive draping is prepared, because the bone resection may produce a bloody effusion and then the tourniquet was deflated. Low-molecular-weight heparin was used for venous thromboembolism prophylaxis in all patients. Postoperative rehabilitation consisting of range of motion and isometric quadriceps exercises was initiated in all patients as soon as possible after the surgery and partial weight-bearing was allowed the first week postoperatively for 6 weeks (Figure 3(i)). At 6 weeks postoperatively, radiographs were obtained and full weight-bearing was allowed.
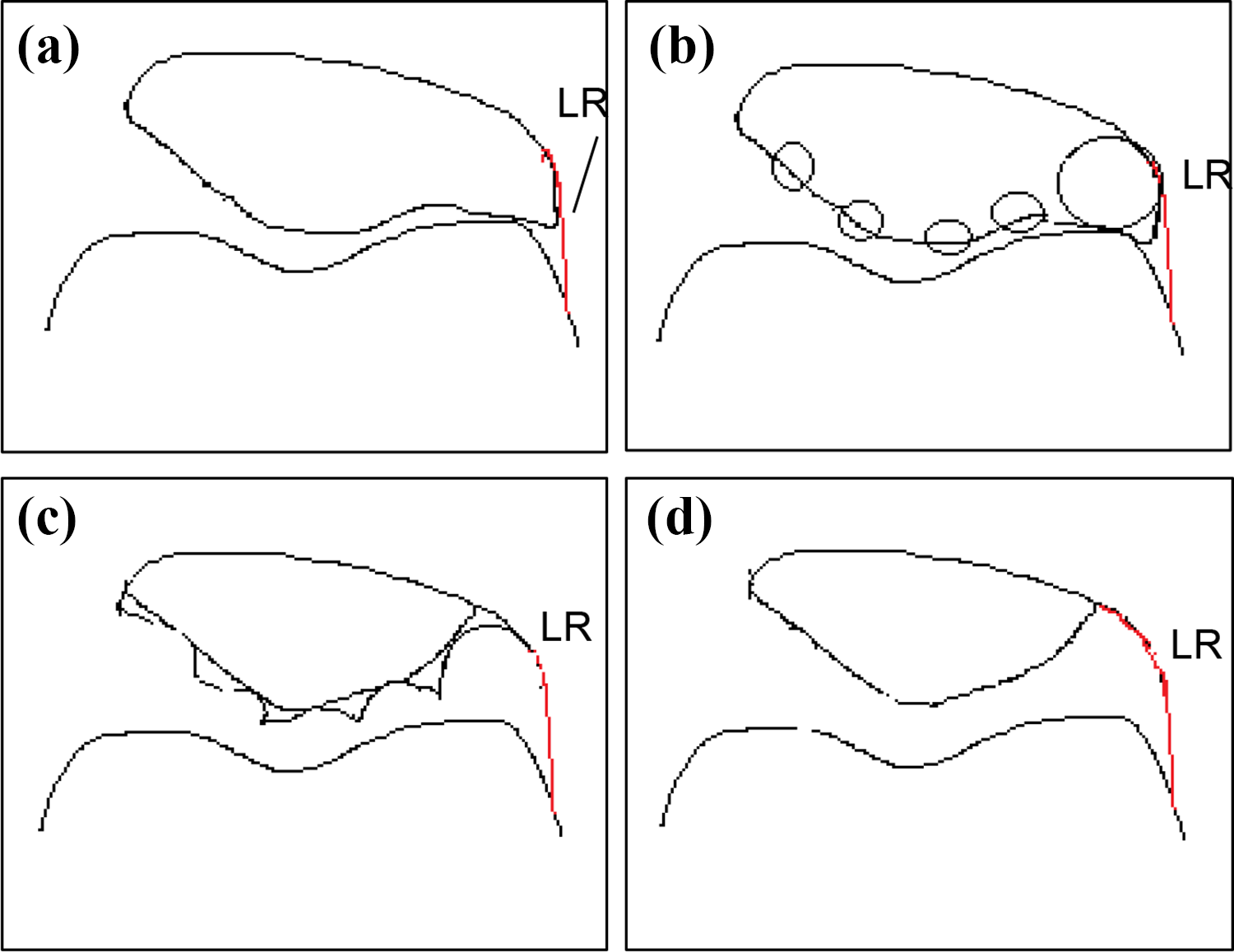
Scheme of the patella resection. (a) The patella is schematically presented. Preoperative image. (b) K-wires insertion places in the sagittal/coronal plane in the longitudinal direction are shown. (c) Wavy edge of the patella after resection with drills, the prospective line of a new contour of the articular surface of the patella is shown. (d) Postsurgery image. LR: lateral retinaculum; K-wires: Kirschner’s wires.

Description of the surgical technique. (a) and (b) K-wires were conducted. (c) and (d) With the help of a cannulated drill, the subchondral layer of the patella width was resected along the knitting wires. (e) The arthroscopy of the knee joint. (f) X-ray image post-surgery. (g) and (h) Movement control in PF joint. (i) At discharge. K-wires: Kirschner’s wires; PF: patellofemoral.
Ethical approval
All procedures performed in the study were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed consent
Written informed consent was obtained from all individual participants included in the study. Additional informed consent was obtained from all individual participants for whom identifying information is included in this article.
Results
The most relevant clinical and radiographic data before surgery are summarized in Table 1. No major complications were detected after the noninvasive surgical treatment in our series. WOMAC score assessment shows considerable improvement of pain and function—the indicators improved significantly by 2.3 points in relation to pain and by 2.1 points in relation to the function (Table 2). Twenty-one patients assessed their knee as improved, five as unchanged, and one as worse with respect to pain. These latter six patients with no effect on pain reduction also had tibiofemoral OA radiographic signs. Stiffness was not affected by the surgical procedure (p = 0.659). No correlation was found among the follow-up time, the age, body mass index (BMI), and the WOMAC score (data not shown). Patients on admission had moderate to severe pain (VAS, 7.4 ± 1.9). After applying the treatment developed by us, there was a significant reduction in the pain syndrome in the knee joint at discharge (VAS 3.6 ± 1.9, p < 0.001) and at follow-up (VAS, 2.2 ± 1.3, p < 0.01; Table 2). Twenty-one of the 27 operated knees (78%) reported pain relief after surgical treatment. The average knee clinical score using the KSS improved from 54.5 points (SD, 8.2; range, 36–72) before surgery to 76.3 points (SD, 12.8; range, 49–100) after the surgery; whereas the average functional score increased from 71.4 points (SD, 11.6; range, 40–80) preoperatively to 83.6 points (SD 14.3; range 40–100) after surgery (Table 2).
Subjective assessment of patients before and after surgery using WOMAC score, VAS scale, and KSS score.

WOMAC: Western Ontario and McMaster Universities Arthritis Index; VAS: visual analog scale; KSS: Knee Society Score.
The sulcus angle was not affected by the procedure (p = 0.634; Table 3). The mean Merchant’s congruence angle before surgery was 22.7° (SD, 17.8°; range, 0° to 60°) and the mean angle after the surgery was 15.4° (SD, 22.2°; range, −8° to 50°). The mean difference between pre- and postsurgery Merchant’s congruence angle was 7.3°. The postoperative congruence angle did not correlate with the pain (r = 0.23, p = 0.1). However, the postoperative congruence angle showed good correlation with function (r = 0.319, p = 0.027). The PF index decreased considerably after surgery (Table 3). The mean patellar width and thickness were decreased after surgery (
Values of angles measured in the axial view.

PF: patellofemoral.
aMeasured in the posteroanterior weight-bearing view.
Discussion
In the present study, we developed a new method of minimally aggressive method of surgical treatment of PFO and investigate if the satisfactory outcome can be achieved with this method in active middle-aged patients in hopes of delaying partial or total joint arthroplasty. PFO can cause severe disability and, sometimes, it is more disabling than OA in the medial tibiofemoral compartment. 1 This ultimately leads to pain during activities that require a deep flexion of the knee, which results in a challenging and limiting issue especially in middle-aged and active patients. 2,8,9
Several surgical techniques have been reported for the treatment of PFO following failed conservative treatment. 3,8 PLFE is described in the literature as a safe procedure to treat isolated PFO, and it does not affect a potential patellar replacement, if needed, 9 but does not realign the patella in the trochlear groove. 14 Thus, PLFE and bony resection of thickness of the patella with the formation of new PF contour were performed as a combined procedure. Main difference of technique was that we did not perform open surgery, but only small (10 mm) skin incision was made above the insertion point of the K-wires. The fibers of the quadriceps tendon are bluntly apart in the longitudinal direction along the fibers. The defender of soft tissues from the drill is installed on the wire next to the bone of the patella, therefore drilling prevents tearing and winding of soft tissues on the drill. So there was no significant soft tissue damage during the introduction of K-wires. Using of the electro-optical transducer (Siemens Arcadis Varic C-Arm; Soma Technology, Inc.) in pulsed fluoroscopy regimen with average exposure time 5–10 s turned on only during K-wires insertion points localizing prevent excessive irradiation time during operation. Using K-wires and then drills of different diameters allow partly removal of facet and tissue of the patella. The potential risk of fracture of the patella and rupture of the extensor reduced by ensuring the protection of the extensor and the correct selection of the diameter number of the cannulated drill for reaming. Arthroscopic patellar shaving and debridement is an easy procedure and allowed us to remove remnant parts and smoothen patellar edge from new contour and better align to the trochlear groove.
The purpose of surgical treatment of the patellar articular surface is to relieve pain and preserve the mechanical advantage of the patella for normal knee function. Albanese et al. 22 showed that near-normal PF biomechanics were maintained with the removal of 25% of either the medial or the lateral facets. Therefore, 1 cm or 1.5 cm resection of the patellar lateral facet does not have a detrimental effect on the quadriceps function. The mean lateral patella that we removed was 26%. We measured the mean patella width:thickness ratio, which was 1.8:1.0 in our series after surgery. Same as Porteous et al. proposed as the normal “index of patella width:thickness” = 1.8:1, which can be used as a guide for restoring patella thickness during total knee replacement (TKR) or patellafemoral replacement to that of a knee free from age-related wear and OA. 23
The mechanism, by which PLFE improves functional scores, remains unproven. Paulos et al. 12 showed that denervation of the lateral retinaculum caused by the associated lateral retinaculum release may play a role in decreasing pain and improving function. Also, resecting the “kissing” osteophytes from the lateral patella and femur reduces “catching.” The bony resection of lateral facet and thickness of the patella with the formation of new PF contour may contribute to decreasing contact pressures on the lateral femoral condyle and decreased mechanical crepitus and eliminate an added source of pain. In our series, the mean patellar thickness decreased after surgery on 5.6 mm. Vaquero and Arriaza performed patella thinning osteotomy and found that thinning the patella by 7 mm significantly reduced PF joint reacting forces. 24 Postpatella thinning osteotomy improvement may be attributable to various factors, including decreased PF pressure and decreased intraosseous pressure.
In our study group, 78–82% of the surgeries achieved pain decrease and knee function improvement. Functional improvement has been reported to be maintained for a long-term period. 13 Our patients were followed for a short-term period; mean 24.1 month, which of course not enough to make a final estimation. However, the patients in our study showed considerable improvement in pain and function according to the WOMAC score. Six patients had no improvement of pain syndrome; they had tibiofemoral OA radiographic signs, potentially showing that they can be candidates for TKR. Studies after isolated PLFE solely also reported considerable improvement based on the KSS 14 and good and moderate results in 90% 12,14 of the patients. BMI did not show any effect on clinical outcome in our series similarly as already shown in other studies. 9 Most of the radiographic parameters did not correlate with the clinical outcome based on the WOMAC score. Other investigators also have reported that the radiographic appearance does not always correlate with the clinical symptoms. 13,25 This may be one of the reasons that so many surgical techniques are recommended. Neurosensory mapping of the internal knee structures showed no sensation on the patella cartilage surface. 26 Our method had no effect on the trochlear dysplasia, which limits the usage of this method in patients with trochlear dysplasia. In our case, a series exclusion criterion was “previous patellar dislocation,” main reason of which is trochlear dysplasia. The main goal of our technique was to remove the pain syndrome: due to the medialization of the patella, reducing intraosseous pressure (reducing the thickness of the patella), and restoring biomechanics in the PF joint. Resection of the patella thickness involving cartilage did not cause further pain in our patients. In the PF joint, PF congruence and smooth kinematics appear to be much more important than normal articular cartilage. 8,10 In contrast, the anterior synovial tissue, the fat pad, and the capsule were the most sensitive sites in the knee. This feature might partially explain why there is a poor correlation between the degree of patellar chondromalacia and malpositioning and clinical outcome based on the subjective assessment. Soft tissue balancing and the degree of synovitis might play an important role in clinical symptoms.
Conclusion
PLFE with resection of the patella thickness and forming new contour by our developed method is a minimally invasive procedure, less aggressive, simple, effective enough, and safe with potentially less complications in selected patients, and it requires a relatively short period of time for postoperative rehabilitation and allows quick recovery of function. In accordance with positive clinical outcomes seen in the literature and our clinical experience, we recommend our approach for the treatment of isolated PFO in middle-aged active patients with high physical demands. Nevertheless, future long-term studies with large sample sizes are needed to further assess the efficacy of this procedure in comparison with more aggressive approaches.
Footnotes
Authors’ note
Any research materials related to this article (e.g. data, samples, or models) can be accessed from authors upon request.
Acknowledgements
The authors are grateful to the staff of the traumatology and polytrauma departments of the City Hospital #1 of Pavlodar city as well as to the patients participating in the study.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.