
Abstract
Bilateral acetabular fractures have been documented in the setting of high-energy trauma, but few reports regarding atraumatic bilateral acetabular fractures exist. The following is a case report of bilateral insufficiency acetabular fractures which occurred acutely in the absence of trauma in a 49-year-old female. The case highlights the importance of perioperative awareness of those patients at significant risk of insufficiency fractures and offers a relatively elegant, less invasive solution for early mobilization in the context of acetabula insufficiency fractures.
Introduction
Acetabular fractures are most commonly associated with high-energy trauma in young patients. In the elderly however, insufficiency fractures due to osteoporosis are the leading cause of acetabular fractures. 1 Bilateral acetabular fractures have been documented in setting of high-energy trauma, but few reports regarding atraumatic bilateral acetabular fractures exist, these most exclusively being associated with seizure activity due to epilepsy or electroconvulsive therapy. 2 The following is a case report of bilateral isolated insufficiency acetabular fractures which occurred acutely in the absence of trauma in a 49-year-old female. The subject patient provided informed written consent to have her case published.
Case
A 49-year-old female presented to the emergency department with severe abdominal pain associated with vomiting and constipation for 4 days. Her past medical history included liver transplantation for hepatitis C virus cirrhosis (requiring regular oral Sirolimus), chronic renal impairment (stage 4), osteoporosis (T score −3.1, managed with regular Zoledronic acid) and asthma, previously requiring long-term oral corticosteroid therapy.
The underlying cause of her presentation was investigated via serial examinations, upper abdominal and renal tract ultrasound and contrast computer tomography (CT) imaging of the abdomen and pelvis. Ultrasounds showed bilateral renal atrophy in keeping with chronic renal impairment without additional pathology and normal hepatic echotexture/vasculature. CT imaging was inconclusive demonstrating long segment low attenuation proximal bowel wall thickening and mildly dilated loops of proximal small bowel – suspicious for obstruction and ischaemia/enteritis without evidence of perforation or a transition point. Both acetabula were normal without evidence of fracture. In the context of persistent severe pain, acute on chronic renal impairment and a rising lactate the patient was taken to theatre for exploratory laparotomy. No pathology was identified and the abdomen was closed.
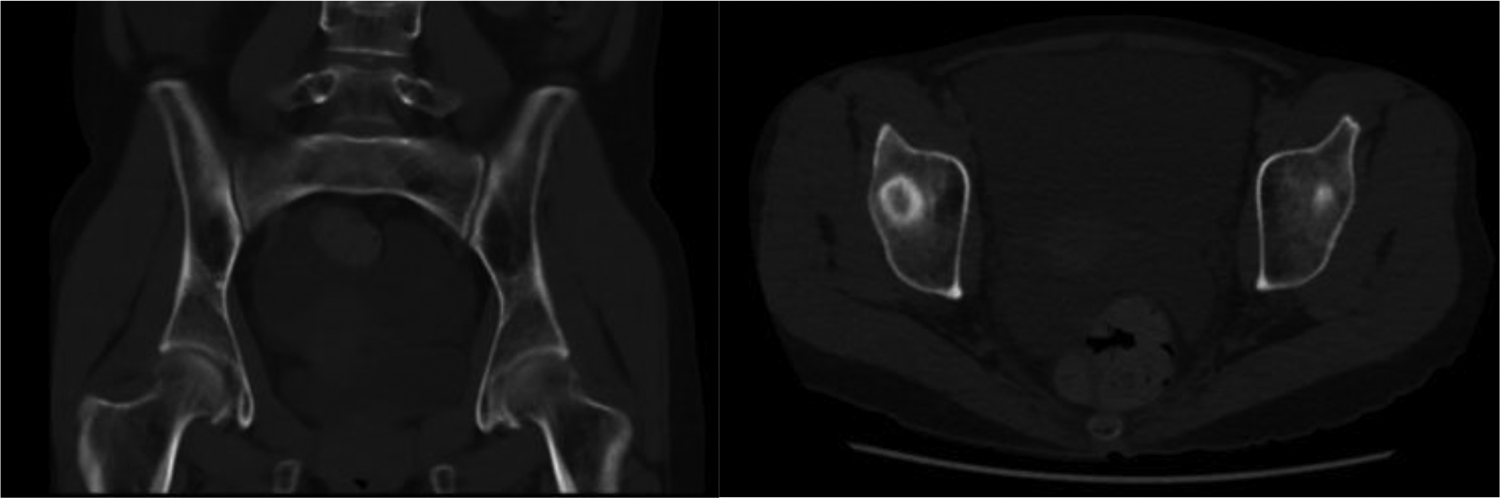
Post-operatively in recovery, the patient complained of bilateral groin pain and a subsequent CT scan identified bilateral anterior column posterior hemitransverse fractures of both acetabula (Figure 1). These fractures were not present on pre-operative imaging (Figure 2) undertaken less than 24 h prior. Fortunately, the patients presenting abdominal pain resolved without further active treatment. She initially underwent a period of non-operative management but with continued pain and immobility elected to proceed to surgery for reduction and internal fixation of both acetabula after two inter-hospital transfers. The surgery was performed 24 days following detection of the fractures applying less invasive principles to prevent further medial and superior migration of the femoral heads. Detailed anatomical reduction was not attempted in this very high-risk patient with coagulation problems and limited physiological reserve (Figure 3). Three 10 cm incisions were utilized (midline Pfannenstiel and two symmetrical incisions over the iliac crests). At 1 year post-surgery the patient was mobilizing without aid, did not require regular analgesia and radiographs demonstrated good bony healing without secondary displacement of the fractures or hardware.

Bilateral anterior column posterior hemitransverse acetabular fractures and left sacral ala fracture evident on a focused pelvic CT within 24 h of laparotomy. CT: computer tomography.
Intact acetabula evident on pre-laparotomy CT. CT: computer tomography.

(a) Post acetbula fixation imaging demonstrating bilateral suprapectineal plates. (b) Radiographs 1 year following fixation demonstrating bony union.
Discussion
Described by Pentecost et al. in 1964, ‘insufficiency fractures’ represent fractures that occur when normal or physiological stress acts on abnormal bone. Insufficiency fractures contrast ‘fatigue fractures’ in which abnormal forces fracture normal bone and the term ‘pathological fracture’, which itself should be limited to the description of fractures occurring through a focus of abnormally weakened bone – typically by tumour. 3 Insufficiency fractures themselves primarily occur in the weight-bearing lower extremities and pelvis. 4 Acetabular insufficiency fractures themselves most commonly occur concurrently with other pelvic fractures, however several cases of isolated acetabular insufficiency fractures have been previously documented. 5,6
It is unclear at what perioperative point this patient sustained her injuries, however at some stage she sustained enough force to both her acetabula to result in fracture. This specific acetabular injury pattern is encountered almost exclusively in osteoporotic geriatric patients 7 whereby falls from standing result in a force directed through the femoral greater trochanter which is subsequently transmitted anteromedially to displace the anterior column and quadrilateral plate with eventual anterocentral displacement/dislocation of the femoral head. 8,9 Controversy exists whether these injuries are best managed surgically via percutaneous fixation, open reduction internal fixation or acute/delayed arthroplasty. This decision should be individualized, based on the patients’ health status, functional requirements, fracture personality and available surgical expertise. 10 However, the achievement of anatomical reduction and internal fixation in this fracture pattern in delayed presentations and in patients with poor physiological reserve is technically challenging, if not impossible. In cases of articular cartilage disintegration and post-traumatic hip arthritis, successful arthroplasty is dependent on the stabilization of the displaced acetabular fragments to allow solid fixation of the acetabular component. Several reports have described the technical difficulties in achieving this when the anterior acetabular structures are fractured. 7,9 The symmetry of this patients’ fractures is suspicious for flexion of the hips with the femoral necks driving against the anterior column, however the exact mechanism remains unknown. She was catheterized without complication prior to any anaesthesia and positioned supine during the laparotomy. Neither stirrups nor lithotomy positioning were utilized at any stage and the patient was transferred on and off the operating table without incident. This patient did not have a history of epilepsy and did not experience witnessed seizure activity during her perioperative course.
This case highlights the importance of perioperative awareness of those patients at significantly high risk of insufficiency fractures and offers a relatively elegant, less invasive solution for early mobilization in the context of acetabula insufficiency fractures.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.