
Abstract
Background:
Based on established posterior atlantoaxial fixation techniques, we present a novel technique that uses a polyaxial screw rod system and utilizes a combination of C1 lateral mass and C1–C2 transarticular screws.
Methods:
We conducted a retrospective review of six men and four women (mean age: 57, range: 20–86). Indication for atlantoaxial fixation was type II odontoid fractures or pseudarthrosis after odontoid fracture (n = 7), rheumatoid arthritis (n = 2) and os odontoideum (n = 1).
Results:
The mean follow-up time was 48 months (range: 24–72). There were no intraoperative complications such as vertebral artery, nerve root or spinal cord injury. Post-operative imaging showed no screw malposition. During follow-up, no patient had screw loosening, screw fracture or bone absorption around the screws. Clinically, patient neck pain improved in all cases.
Conclusions:
C1 lateral mass and C1–C2 transarticular polyaxial screw rod fixation is a novel and potentially effective surgical technique for achieving immediate rigid immobilization of the C1–C2 motion segment. However, further biomechanical studies should be performed to prove our clinical results.
Keywords
Introduction
Several techniques have been described to treat atlantoaxial instability, ranging from external immobilization to surgical procedures. Nowadays, the most accepted treatment modalities are the Magerl transarticular screw fixation 1 and the Harms/Goel C1–C2 rod technique. 1 –3 C1–C2 transarticular screws can be combined with posterior wiring, claws or laminar hooks to achieve 360° three-point fixation. In recent biomechanical cadaver studies, three-point fixation techniques result in better biomechanical fixation constructs compared with the established C1–C2 fixation techniques. 4 Therefore, we present a novel technique for posterior atlantoaxial fixation that uses a polyaxial screw rod system and utilizes both C1 lateral mass screws and C1–C2 transarticular screws (Figures 1 and 2).
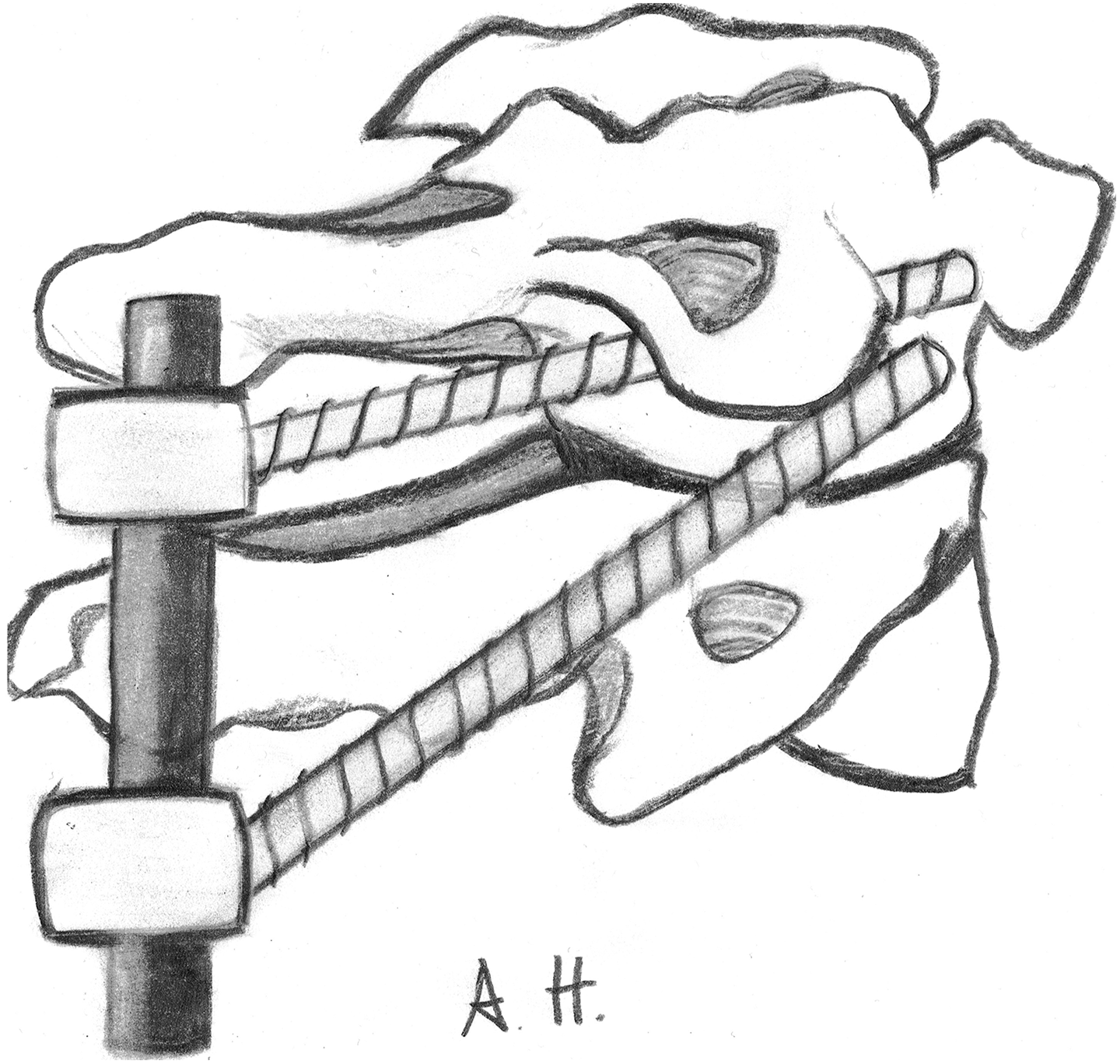
Schematic drawing showing posterior atlantoaxial fixation with combination of C1 lateral mass and C1–C2 transarticular screws using a polyaxial screw rod system.

Post-operative sagittal computed tomographic-reconstructed view after atlantoaxial fixation with combination of C1 lateral mass and C1–C2 transarticular screws.
Methods
Patients
We reviewed the records of 10 patients who underwent atlantoaxial fixation using both C1 lateral mass screws and C1–C2 transarticular screws in our institution between March 2012 and October 2017. The patients (six men and four women) were between 20 and 86 years of age (mean age 57 years). Indication for C1–C2 fixation includes odontoid fracture including pseudarthrosis after anterior odontoid screw placement in seven patients, craniovertebral rheumatoid arthritis in two patients and os odontoideum in one patient. All patients had pre-operative thin sliced computerized tomography (CT) scan and/or CT angiography of the craniovertebral junction to assess the course of the vertebral artery and any aberrant paths. Patient data are summarized in Table 1.
Patient characteristics.
Surgical technique
The patients were placed in the prone position with their heads fixed in a three-pin head holder. The atlantoaxial joint had to be aligned, otherwise the transarticular screws could not be inserted. A midline incision was performed. The suboccipital space, the posterior elements of the atlas and the axis were exposed. The placement of the transarticular screws required separate stab incision to achieve the extremely steep angle to cannulate the C1 lateral mass. Therefore, a small paramedian incision was made at the level of C7 or Th1 spinous process. The inferior facet of C2 was docked, with or without trocar. Starting at the medial half of the inferior facet of C2, drilling was started under fluoroscopy. The ideal trajectory was when the drill was aimed at the superior portion of the C1 anterior arch. Drilling was performed through the C1–C2 facet joint to the level of the anterior arch of C1, within the lateral mass of C1. A polyaxial screw, typically 40 mm in length, was placed. Next, the dorsal arch of C1 was exposed laterally. The vertebral artery was typically located at the sulcus arteriosus of C1 on the superior aspect of the C1 arch. The C2 nerve root was identified and mobilized inferiorly. Haemostatic agents should be used to control bleeding from the vertebral venous plexus surrounding the C2 nerve root. The lateral part of the C1 arch, which overlies the lateral mass below the sulcus arteriosus, was drilled until the lateral mass was exposed. The entry point was identified at the centre of the C1 lateral mass. A drill was placed at the decorticated C1 lateral mass and under fluoroscopy a pilot hole was performed. A polyaxial C1 lateral mass screw was inserted; contrary to expectations, the C1 lateral mass screw did not collide with the transarticular screws in our series. Otherwise a shorter screw can be inserted. The polyaxial screw head should sit superficial to the C2 nerve root without causing foraminal stenosis after fixing the rods. The process was then repeated on the other side. We usually placed a bone graft in the interlaminar space or laterally in the facet joint. Two subfascial drains were placed, using the stab wounds.
Results
The C1 lateral mass screw and C1–C2 transarticular screw rod construct was applied in 10 patients for C1–C2 fixation.
In one patient, the C1–C2 transarticular screw was inserted on the left side and C2 pars screws on the right side, due to the aberrant course of the vertebral artery on the right side. In another patient, the C1 lateral mass screws and C2 pars screws were primarily inserted for a dislocated odontoid fracture, and after repositioning the C2 pars screws they were replaced by longer C1–C2 transarticular screws. There were no major complications (e.g. vertebral artery or spinal cord injury). X-Ray and/or CT were performed post-operatively and during follow-up in all patients. No instance of incorrect screw position was found. The mean follow-up time was 48 months (range: 24–72). During follow-up, no patient had screw loosening, screw fracture or bone absorption around the screws. Clinically, neck pain improved in all cases.
Discussion
We were able to demonstrate that the combination of C1 lateral mass screws with C1–C2 transarticular screws is a safe and solid technique for posterior three-point atlantoaxial fixation based on well-established posterior atlantoaxial fixation techniques. The particular anatomy of the C1 lateral mass allows placement of two independent screws on the same lateral mass, as we have done in our series. The transarticular screw purchases the lateral mass at its anterior–inferior portion while the C1 lateral mass screw is placed the middle or upper portion of the lateral mass. The rods connecting the two screws result in a posterior tension band and the addition of a cross-link adds significant rotational and axial stability. Treatment indication includes all kinds of atlantoaxial instabilities.
The C1–C2 motion segment has the widest range of movement of any spinal motion segment. Flexion–extension ranges are between 10° and 22°, 4,5 axial rotation ranges are between 23° and 38° per side 4,5 and lateral bending is 6.7°. 6 Sagittal translation, lateral translation, distraction and compression are also present in the non-pathologic state, to some degree. 4,6 This range of motion increases if components of the C1–C2 motion segment are damaged by trauma, inflammation, neoplasm or congenital defects. Therefore, atlantoaxial immobilization by instrumentation is challenging. The first description of surgical treatment for atlantoaxial instability appeared in the literature in 1910 and was reported by Mixter and Osgood. They passed the posterior arch of the atlas to the spinous process of the axis with a heavy silk thread. 7 Since then, other techniques have been developed, like the Gallie fusion, the Brooks fusion and the interlaminar clamp fusion. These techniques of dorsal atlantoaxial fusion include variations on wiring together the posterior elements of the axis and atlas. 7 Although these techniques restrict flexion–extension, they offer minimal stabilization during axial rotation and lateral bending. This contributes to high nonunion rates (as high as 25%), and patients require longer periods of external immobilization post-operatively. 8 Additionally, they cannot be applied in case of congenital absence or fracture of the C1 or C2 arch.
Posterior wiring techniques and interlaminar clamps were nowadays completely replaced by rigid screw fixations of the atlas and axis. 7 The transarticular screw fixation through the C1–C2 articular surfaces was first described by Jeanneret and Magerl. 1 The C1 lateral mass screw with C2 pedicle screw construct was initially created with plates and screws by Goel and subsequently popularized with a screw rod construct by Harms. 2,3 Other techniques for atlantoaxial fixation include the Wright C1 lateral mass–C2 translaminar screw construct, and the C1 lateral mass–C2 pars screw construct. The main limitation of the C1–C2 transarticular fixation technique relates to anatomic variations that occur in up to 20% of patients. 1 Anatomic variations in the location of the foramen transversarium place the vertebral artery at risk during screw placement. 9 Additionally, the technique cannot be performed in patients with a fixed thoracic kyphosis or who are obese, as these conditions preclude the steep angle of approach required for the screw insertion. The technique of C1 lateral mass screws combined with C2 pedicle screws results in high fusion rates and good outcomes. The main advantages are that it can be used in patients who have an anomalous course of the vertebral artery. Furthermore, the C1 and C2 screws can be placed before reduction is performed.
Based on several biomechanical reports, the C1–C2 transarticular screw fixation provides better stabilization than other techniques. 10 –12 However, a recent meta-analysis of the existing literature showed that the technique of C1 lateral mass combined with C2 pedicle or pars screws provides at least the same rigidity as the C1–C2 transarticular screws. 13 To achieve more stability, several three-point fixation techniques of the C1–C2 complex have been published. They include the C1–C2 transarticular screws combined with posterior wiring, claws or laminar hooks. 12,14 Guo et al. combined C1–C2 transarticular screws with C1 laminar hooks and connected them with a rod. 11 In their cadaver-based study, this construction resulted in better biomechanical fixation construct compared with established C1–C2 fixation techniques. 12
The C1 lateral mass screw with C1–C2 transarticular screw is a novel posterior atlantoaxial fixation technique for atlantoaxial instability. This technique was described by Vilela et al. in three patients with favourable outcome. 14 It is based on established posterior atlantoaxial fixation techniques. Therefore, it has the advantages and strengths of both techniques. The anatomy of the C1 lateral mass allows two independent screws to be placed on each side. This has been proven by our results. The connecting rods establish a posterior tension band and provide additional stability. Although we have not performed any biomechanical studies, it has been shown that increasing the number of fixation points further limits C1–C2 motion. 15 This technique can be useful in cases when the C1 posterior arch is fractured or a C1 laminectomy is required. Additionally, it can be applied in a multilevel construct. In cases where anatomic variations of the vertebral artery occur on one side, C1 lateral mass screws can be combined with either a pedicle or pars screw on the ipsilateral side and a transarticular screw on the contralateral side (patient 4).
Conclusion
In spite of the small population, we conclude that C1 lateral mass and C1–C2 transarticular polyaxial screw rod fixation is a novel and effective surgical technique to achieve immediate rigid immobilization of the C1–C2 motion segment. Congenital absence or fracture of the C1 arch is not a contraindication. In cases where anatomic variations of the vertebral artery preclude safe placement of the transarticular screws, it is always feasible to switch to other fixation techniques of the axis at the ipsilateral side. However, further biomechanical studies should be performed to prove our clinical results.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.