
Abstract
Purpose:
To assess the accuracy of cup orientation and learning curve of the disposable accelerometer-based portable navigation system for total hip arthroplasty (THA) in the supine position.
Methods:
A total of 75 patients who underwent THA through the anterolateral supine approach (ALS) with an accelerometer-based portable navigation system for the supine position (HipAlign®) between July 2017 and October 2018 were analyzed in this study. We compared the intraoperative cup angles using navigation records with the postoperative angles using postoperative computed tomography (CT) data. All patients were categorized into the following groups according to the course of three discrete, sequential operative time periods: 1–25 (initial group), 26–50 (intermediate group), and 51–75 (recent group). We compared the accuracy of cup inclination and anteversion among the three groups. The time required for navigation and the operative time of all patients were measured.
Results:
The average absolute error in measurement (postoperative CT-navigation record) was 2.6° ± 2.7° (inclination) and 2.8° ± 2.7° (anteversion). There were no significant differences among the three groups. The average time required for navigation and the operative time were 365.1 ± 90.3 s and 76.1 ± 1.6 min, respectively. The required time for HipAlign® navigation and operative time were constant in most patients, except for those of the initial five cases.
Conclusion:
The accelerometer-based portable navigation system provides good accuracy of cup orientation, has a short learning curve, and requires a minimal surgical time for THA in supine position.
Brief introduction
Accurate acetabular cup position is a critical factor for a successful total hip arthroplasty (THA) because cup malposition causes many complications, such as impingement, dislocation, polyethylene wear, and ceramic fractures. 1 –4 Lewinnek has established the “safe zones” for cup placement as 30°–50° of abduction and 5°–25° of anteversion to minimize dislocation risk. 5 A freehand technique for cup implantation with the patient placed in the lateral decubitus position has a broad range of cup orientations with a higher proportion of outliers even for experienced surgeons. 5,6
The relative muscle-sparing approach, such as the direct anterior approach and mini-anterolateral supine approach (ALS) in the supine position, has gained popularity recently because of its potential for decreasing rates of dislocation, a shorter length of hospital stay, and faster return to function, compared with other surgical approaches. 7 –10 Several authors have reported the good accuracy of cup positioning using the anterior approach. 11,12 However, the freehand technique has a broad range of cup orientations with a higher proportion of outliers even if using the anterior approach. 13 Therefore, a computer-assisted navigation system is the useful method to obtain precise information on cup angles. 14 Several authors have shown that an acetabular cup may be accurately positioned using a computer-assisted navigation system than with the freehand positioning technique. 15,16 However, this technique has not been established in practice for various reasons, such as increased costs, additional surgical trauma, and prolonged surgical time. 17
OrthAlign (Orthalign Inc, Aliso Viejo, California, USA) is an accelerometer-based device consisting of a disposable computer display unit and a reference sensor. This system aims to combine the accuracy of large-console computer navigation systems with the convenience of conventional alignment techniques. 18 Several papers demonstrated the good accuracy of accelerometer-based portable navigation system for total knee arthroplasty. 19 –21 Nam et al. reported that the accuracy was similar to those of other conventional navigation systems. 20 HipAlign® allows cup navigation for supine position approach of THA and is less costly compared to the conventional navigation systems. Moreover, this system is expected to be widely used not only in hospitals with high volume of THA cases but also in many clinics with low volume because of its advantages, such as low cost, minimal required time for use, and ease of use. However, the accuracy and learning curve of the accelerometer-based portable navigation system for THA at supine position have not been reported.
The aim of this study was to assess a surgeon’s learning curve and the accuracy of cup orientation using the accelerometer-based portable navigation system for THA in the supine position.
Materials and methods
Patients
The study’s protocol was approved by the ethics committee of our hospital. The patients provided informed consent for participation in this study. This prospective cohort study enrolled 78 consecutive patients with osteoarthritis of the hip who underwent primary unilateral THA in the supine position using the HipAlign® system (OrthAlign Inc.) at our institutions between July 2017 and October 2018. All patients underwent THA with a Fitmore or Taperlock Microplasty (Zimmer-Biomet, Warsaw, Indiana, USA) performed by a single senior surgeon (TF). Patients with bilateral THA, distorted proximal femoral anatomy, and a history of osteotomy and trauma were excluded. In the surgical procedure, three patients were excluded because the navigation could not be performed due to poor fixation of the pin or problems of the navigation procedure itself. The remaining 75 patients were included in this study (64 women and 11 men; age: 70.0 ± 9.5 years, body mass index (BMI): 23.5 ± 3.6 kg/m2). There were 40 right joints and 35 left joints.
Surgical procedures
All surgeries were performed using the HipAlign® (OrthAlign) portable navigation system. First, the navigation unit was calibrated on a flat table prior to surgery. Two fixation pins were placed in parallel on the iliac crest, and the pelvic unit’s base was secured over both pins (Figure 1(a) and (b)). Three anatomical landmarks, the bilateral anterior superior iliac spines and pubic symphysis, were registered.

(a) Two fixation pins placed in parallel on the iliac crest. (b) A navigation sensor with a base unit. (c) A monitor showing cup inclination and anteversion angles with pelvic tilt and rotation angle.
All surgeries were performed using the mini-anterolateral supine approach. After the neck osteotomy and acetabular shell preparation, a navigation sensor was attached to a cup impactor. We used a G7 acetabular cup (Zimmer-Biomet) for all patients. The cup inclination and anteversion angles, based on the functional pelvic plane, were displayed on the monitor dynamically, and we rechecked the inclination and anteversion angles after the cup was inserted (Figure 1(c)). Next, we prepared the femur with the leg in external rotation, hyperextension, and adduction. After capsular release near the greater trochanter, stem implantation was performed (Fitmore stem or Taperlock Microplasty, Zimmer-Biomet). Finally, we closed the wound.
Postoperative measurement of cup inclination and anteversion
For postoperative evaluation, a computed tomography (CT) was taken from the pelvis to the knee joint and was transferred to 3-D template software (Zed hip, Lexi, Tokyo, Japan). Computer-aided design models of the implants were manually adjusted for postoperative multi-planner reconstruction in CT images. Cup inclination and anteversion angles were measured with respect to the functional pelvic plane. To analyze the accuracy of intraoperative navigation records for cup inclination and anteversion, we compared the intraoperative cup angles using navigation records with the postoperative angles using postoperative CT data. We measured the absolute error (postoperative CT measurement—navigation record) of inclination and anteversion.
Assessment of the learning curve
To determine the difficulties in using the navigation device, all patients were divided into the following groups according to the course of three discrete, sequential operative time periods: 1–25 (initial group), 26–50 (intermediate group), and 51–75 (recent group). We compared the accuracy of cup inclination and anteversion among the three groups. We also measured the time required for using the navigation system and the operative time of all patients. Then, the data between the initial 5 patients (1–5) and the remaining 70 patients (6–75) were compared. To assess whether the time required for navigation and the operation time were constant in the remaining 70 patients, 20 patients, excluding the initial 5 patients from the initial group, were categorized as the semi-initial subgroup, and the required time for navigation and operative time were compared among the three groups (semi-initial: 6–25, intermediate:26–50, recent: 51–75).
Statistical analysis
The navigation records (inclination and anteversion) and the postoperative CT evaluation (inclination and anteversion) were compared using paired t-test. We compared the required time for navigation and the operative time between the initial 5 patients (1–5) and the remaining 70 patients (6–75) using unpaired t-test and among three groups (semi-initial, intermediate, and recent) using one-way analysis of variance (ANOVA). In all cases, p values < 0.05 were considered statistically significant.
Results
Accuracy of cup inclination and anteversion angles
We did not find any difference in the accuracy of cup inclination and anteversion angles between the navigation records (inclination: mean = 39.5 ± 2.6; anteversion: mean = 12.0 ± 4.5) and the postoperative CT evaluation (inclination: mean = 38.5 ± 3.4; anteversion: mean = 12.4 ± 4.6), Table 1. The average absolute error in measurement (postoperative CT-navigation record) was 2.6° ± 2.7° (inclination) and 2.8° ± 2.7° (anteversion). The measurement error of inclination within 5° and within 10° was 86.7% (65/75 cases) and 96.0% (72/75 cases), respectively. The measurement error of anteversion within 5° and within 10° was 88.0% (66/75 cases) and 97.3% (73/75 cases), respectively.
Results of inclination and anteversion.
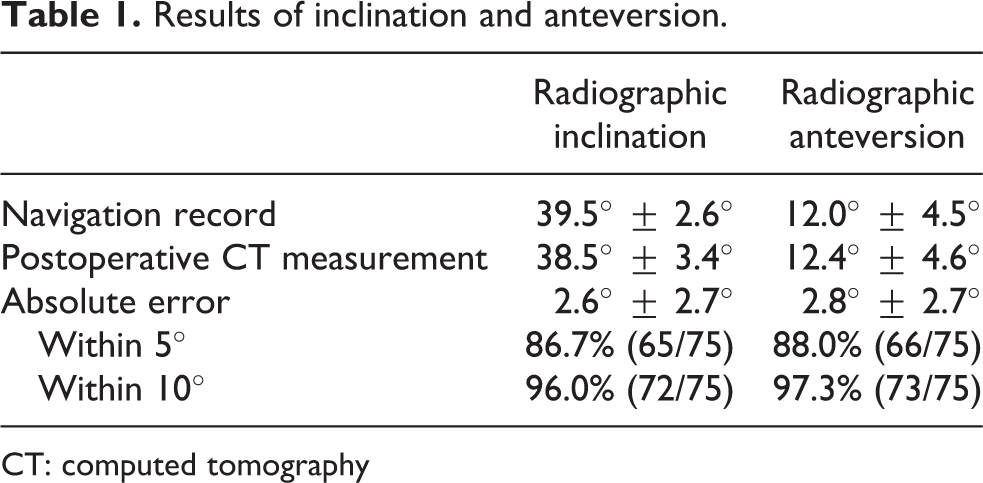
CT: computed tomography
Learning curve
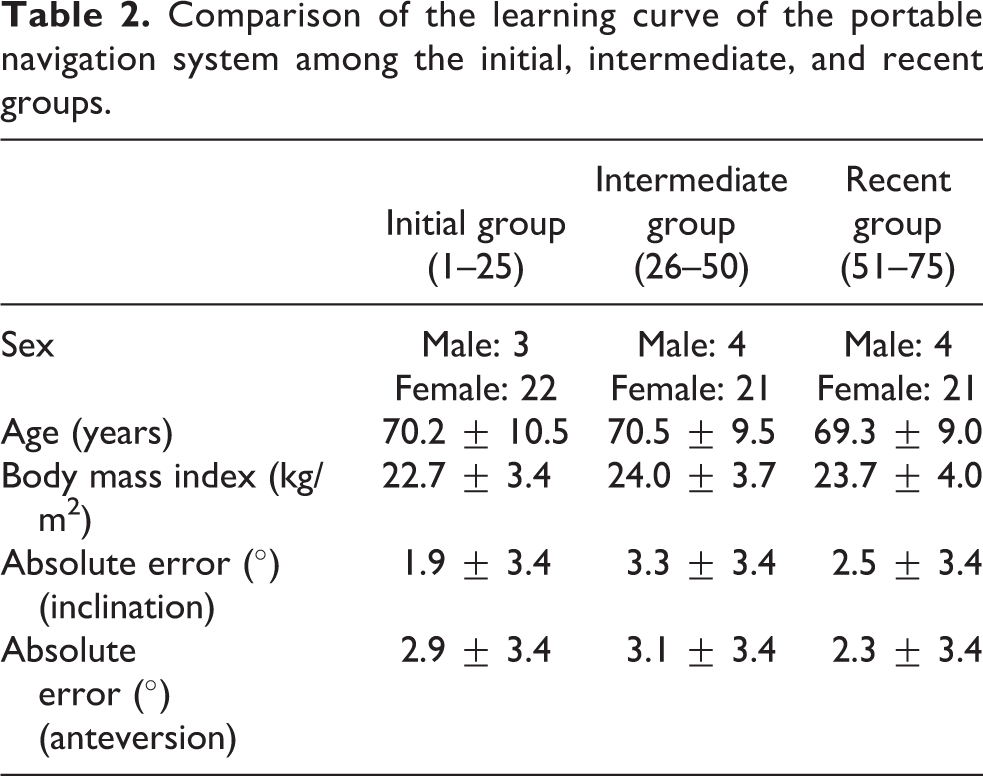
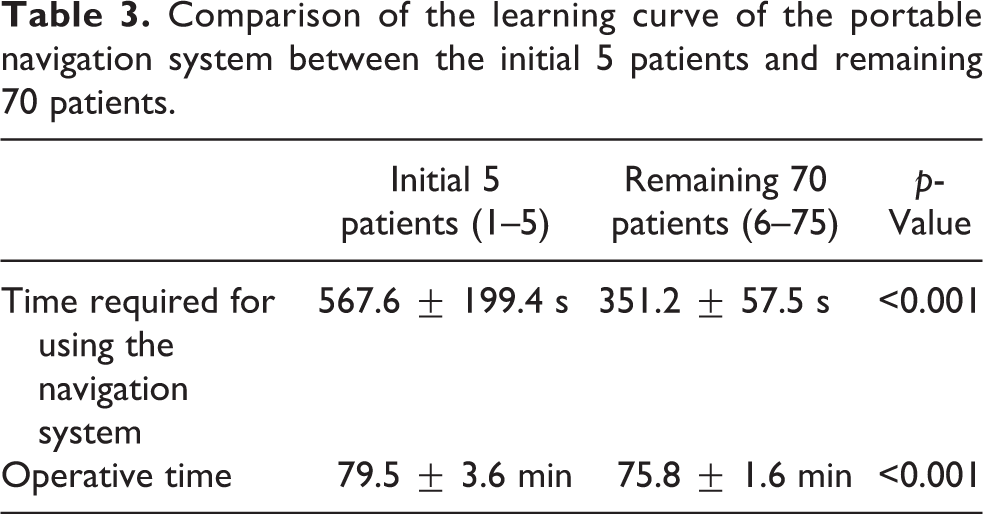
No significant differences in patient factors (sex, age, and BMI) were found among the three groups (Table 2). We also found no significant differences in the absolute error in measurement of both inclination and anteversion among the three groups (initial: 1–25, intermediate: 26–50, recent: 51–75; Table 2). The average time required for navigation and the operative time were 365.1 ± 90.3 s and 76.1 ± 1.6 min, respectively. Figure 2 shows the operative time in all patients according to the sequence of the surgical time period. The initial five cases required a relatively longer operative time with an average time of 79.5 min, but the operative time was constant after the initial five patients. The time required for navigation and operative time of the initial 5 patients are significantly longer than those of the remaining 70 patients (Table 3). However, there were no significant differences in the time required for navigation among the three groups (semi-initial:6–25, intermediate: 26–50, recent: 51–75; Table 4).

The operative time in all patients according to the sequence of surgical time period. The average operation time was 76.1 min. The initial five cases required relatively long operation time, but the operation time was constant after initial five cases.
Comparison of the learning curve of the portable navigation system among the initial, intermediate, and recent groups.
Comparison of the learning curve of the portable navigation system between the initial 5 patients and remaining 70 patients.
Comparison of the learning curve of the portable navigation systems among the semi-initial, intermediate, and recent groups.

Discussion
In this study, we investigated the cup orientation accuracy and learning curve of the disposable accelerometer-based portable navigation system in patients who underwent THA in the supine position. Our findings suggest that this navigation system enables accurate cup placement, has a short learning curve, and requires minimal time for use.
Several studies have investigated cup positioning in navigation THA. 22 Suksathien et al. found that 100% of the imageless computer-navigated cups were within the Lewinnek safe zone, whereas the only 48.4% of the non-navigated cups were within the safe zone. 22 Lin et al. reported the limitations of an imageless computer navigation and showed that the absolute difference between operative inclination and inclination on postoperative CT was 0° ± 2.8°, but anteversion difference was significant at 3.4° ± 3.6°. 23 We demonstrated that the average absolute error in measurement was 2.6° ± 2.7° (inclination) and 2.8° ± 2.7° (anteversion), indicating that this accelerometer-based portable navigation system has more accuracy for cup placement in anteversion, in comparison with the conventional imageless navigation systems. 23
Regarding the learning curve, our study demonstrated that accelerometer-based portable navigation provided no significant difference in the absolute error of cup orientation among the three sequential operative time periods. These results suggested that accelerometer-based portable navigation allows for consistency of component alignment independent of procedural experience. A recent study showed that the learning curve of CT-free navigation in terms of operative time was 14 cases. 24 Other study reported that the operation time using imageless navigation was reduced and became constant after initial 15 cases. 25 Our study demonstrated that the time for HipAlign® navigation and the operative time were constant in most cases, apart from the initial five cases. It was suggested that the learning curve for this system was less than five cases. Moreover, the average time required for navigation using this system was 365.5 s, which was relatively shorter than those of other studies, 26 –30 suggesting that the navigation adds between 4.5 min and 58 min to the operative time. The reason for the short learning curve of HipAlign was explained by the easy registration method. Basically, image-less navigation system required pointing bony landmark surface, but this accelerometer-based portable navigation system did not require any pointing. Therefore, the accelerometer-based portable navigation needs shorter learning curve. This study showed that the accelerometer-based portable navigation system obtained accuracy from the initial cases and had a short learning curve of less than five patients, which imply that it can be widely used in many clinics with low-volume THA cases.
The limitation of this study is that we did not have a control group that used other navigation systems. So, we should compare the accuracy of cup orientation and learning curve of single surgeon between the accelerometer-based portable navigation and other navigation in the near future.
Conclusion
Our study demonstrated that the accelerometer-based portable navigation system is a very useful device to be widely used for THA at supine position not only in hospitals with high volume of THA cases but also in clinics with low-volume cases, as it offers advantages of good accuracy, short learning curve, and minimal required time for use.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.