
Abstract
It is the role of the hip joint to support the superincumbent body weight while its complex range of movement, under a variety of stresses, allows the individual to undertake a wide range of physical activities. It is then perhaps not surprising that a recent anatomical study shows that the upper femur has a structure commensurate with the complexity of its movements. Mechanically, the upper femur consists of two separate bones: the combined femoral head and neck and the femoral shaft. Both bones consist of a mixture of two different types: cancellous bone and cortical bone, each with its own characteristics. Both bones are subjected to two different forces: those of weight bearing and movement and those of bone modelling. In the face of these complexities, this article tenders some theoretical considerations as to how this region functions and deals with these particular problems. From an anatomical viewpoint, the calcar femorale plays a central role in the mechanical structure of the femoral neck and is pivotal in the management of the stresses to which the region is subjected.
Keywords
Introduction
Numerous studies have attempted to define the bony architecture of the proximal femur in terms of human function. 1 Traditionally, descriptions of the upper femur include mention of two bony trabecular columns, one vertical and the other horizontal, which are said to convey the forces generated during physiological activity of the hip (Figure 1). The vertical column has its base in the lower medial femoral neck and ascends vertically into the femoral head. This column is said to convey a compression force. The horizontal column has its base at a bony buttress in the inner, anterior upper femoral shaft from which it extends horizontally to enter the anterior aspect of the femoral head. 2 This column is said to carry a tension force. There is, however, a third cancellous structure which is somewhat enigmatic; the calcar femorale.

Schematic diagram to show the configuration of the two trabecular columns within the femoral neck. Presently, the vertical column and the horizontal column are said to conduct a compression force and a tension force, respectively.
Harty 3 stated that ‘The calcar femorale was described over 100 years ago but precise knowledge concerning its location and nature was later lost, and today many clinicians are still confused on these points’. This may be because the literature on the subject is often conflicting, questionable and/or confusing.
Some of the confusion may have arisen because the term ‘calcar femorale’ has come to mean one of two things, depending upon the outlook of the individual. 4 The classical anatomical ‘calcar femorale’ refers to the vertical, quadrilateral plate of dense cancellous bone which develops in the posterior femoral neck, below but separated from, the lesser trochanter. It is not to be confused with the ‘orthopaedic calcar’, which is the lowermost and thickest point of the cortex constituting the medial wall of the femoral neck. 3 –6
Bigelow 7 noted that the anatomical calcar was termed as the ‘calcar femorale’, ‘Schenkelsporn’ or ‘thigh spur’ by Merkel in 1874. 8 He stated that, as he understood it, the objective of Merkel’s article was, following the tenets of Wyman, 9 ‘to prove the importance of the tissue in supporting the weight of the body and that the strength of the femur is due to this tissue and not to the braces of Wolff and Culmann’. Bigalow 7 recorded that this article, perhaps not surprisingly, leads to a spat between Wolff and Merkel, conducted through the literature. Wolff 10 countered Merkel by saying that ‘Merkel’s theory in no way agrees with Culmann’s calculations which may be accepted as beyond controversy and which prove that the “spur” is not at the point of greatest strain, nor yet where strength is most needed’. This being so Wolff felt that ‘Merkel had awarded to the “cancellous plate under the lesser trochanter” a wholly erroneous importance’.
This, however, did not seem to have resolved the issue with regard to the calcar femorale and the other internal trabecular structures of the upper femur. Dixon
11
stated that There is not yet agreement regarding the arrangement of the bony lamellae or the significance of their disposition; as to whether they are associated with the internal strain of weight bearing in the erect position or whether they are due to muscular action. It has also been urged that the strains and stresses to which the bone tissue is subjected are so complicated and so little understood that, at best, we can only guess at the significance of the arrangement of the bone elements.
What is the calcar femorale?
The upper end of the thigh bone may be looked upon as a tubular structure to the surface of which are fixed projecting masses (trochanters) for the attachment of muscles and ligaments. 11 The calcar is a vertical plate of dense cancellous bone which lies deep to the lesser trochanter but posterior to the neutral axis of the femoral neck. 5,12,13
All the dissections and scans of the calcar were performed by various investigators 1,3,7,11,12,14,15 who have, essentially, dissected the femoral neck in its longitudinal axis, that is, in the horizontal plane, and their findings have been relatively constant. They record that the calcar femorale is thick at its origin from the lower portion of the vertical trabecular column and becomes progressively thinner as it passes laterally through the substance of the trochanteric bulges until it reaches the cortical shaft of the femur, from which point it breaks up into thin, tenuous trabecular strands as it extends further towards the posterior wall of the greater trochanter. 7
Because of this, Bigelow
7
seems to have been in two minds when he wrote saying But the purpose of the osseous plate, whose structure and pathology it is the main object of this paper to discuss, may be at first a little less obvious. It plainly adds a certain strength to the bone, and yet in most bones it terminates beneath the trochanters in papery lamellae wholly inadequate to lend it material support.
Size and shape
Harty
3
noted that the calcar originates medially from the lower portion of the vertical trabecular column in the postero-medial portion of the femoral shaft, and it radiates laterally through the cancellous tissue towards the great trochanter. The calcar, he said, reaches its maximum length and thickness at the level of the upper margin of the lesser trochanter, diminishing progressively in size after that point. Superiorly the calcar femorale fuses firmly with the cortex of the posterior aspect of the femoral neck; distantly extends about two inches anterior to the lesser trochanter and then fuses with the posteromedial aspect of the diaphysis.
Development of the calcar
The calcar femorale is present in every femur which has an ossified lesser trochanter. 12 No calcar is visible in the infant femur but by the time the infant is 3 years old, bony lamellae are present on the deep surface of the cartilaginous lesser trochanter. 3 The calcar appears to be best developed during early adulthood and then gradually atrophies after middle age. 7,12 Nevertheless, although the distal (lateral) portion becomes partly resorbed, the system is maintained throughout life, its presence being revealed by roentgenogram and curettage. 12,14
The true neck of the femur
There have been a number of theories pertaining to the development and function of the calcar, few of which have stood the test of time. The upper portion of the femoral shaft expands to form the greater and lesser trochanters which provide muscle attachment to this region. The anterior wall of the femur at this level is thick and strong but the posterior wall is thin and seemingly very weak. The calcar femorale develops as an apparent cortical extension of the shaft into the neck, 12 as it attaches posteriorly to the inner neck of the upper femur in alignment with the medullary cavity of the femoral shaft. Bigelow 7 proposed that the calcar is, in fact, the true posterior wall of the upper femur which develops within the cancellous tissue of the region in order to maintain the continuity of the shaft and which, in association with the anterior wall, provides mechanical support to the region as a physiological internal shaft.
He noted that in one of the specimens, which he dissected, the dense plate (of the calcar) was the’continuation of the neck, completing the interval everywhere except at its upper part. In this form it adds greatly to the strength of this part of the femur, while the trochanters and their ridge erected upon it both reinforce it and give attachment to the muscles’.
However, maintaining his pessimistic approach, Bigelow 7 continued with the statement that ‘The true neck is often at best but an ineffectual attempt to bridge the interval beneath the trochanters while in the latter half of life it degenerates’.
Nevertheless, this concept of an internal physiological support was extended by Krause 15 and supported by Dixon 11 who proposed that the calcar was only part of a longer condensation which they termed as the ‘lamina femoralis interna’. This, they felt, extended from the lateral area where the calcar joined the posterior wall of the femoral neck to the femoral head, in association with the arching trabeculae of the femoral neck to provide an internal ‘physiological’ wall which provides the necessary support for the muscle action upon this region. These ideas do not seem to have gained much acceptance, particularly as Newell 4 decried theories on the calcar based on a two-dimensional assessment for the femoral neck by section or X-ray and there is little evidence to support the idea of a tubular structure passing through the femoral neck.
Steihl et al. 1 state that ‘Simplistic two-dimensional anatomical and force models may not adequately predict the stresses present in such a three-dimensional model’. 4,5,11 All express the need to assess the region three-dimensionally. In his paper, Garden 5 states that in basic outline the proximal end of the femur is striving towards a spiral form and, by stereo-radiography, the calcar femorale and the internal weight-bearing system are seen to be an upward and spiral continuation of laminae of the posteromedial cortex of the shaft conducting compression forces. Dixon 11 had a similar theory except that, from stereo-radiography and plain X-rays of the femoral shaft, he proposed that the internal weight-bearing system is composed of interdigitating spiral laminae running alternatively in opposite directions and those in each direction conducting either a compression or tension force, respectively.
Function of the calcar
Despite differing concepts and viewpoints, there is no doubt that the calcar femorale is involved in the transmission of forces through the femoral neck.
Farkas et al.
14
state that the calcar femorale contributes to the strength of the femoral neck and is ‘intimately involved in weight bearing’. They go on to state that roentgenographically it can be demonstrated that the calcar is the internal weight bearing system of the neck of the femur forming an angle of from 3 to 8 degrees with the perpendicular during weight bearing in youth and throughout middle age; a compression system and apparently the only spongy structure in the neck which serves weight bearing. The calcar’s alignment with the stress trajectories in the femoral neck and its higher radiographical density compared with the predominantly cancellous bone of the rest of the neck, indicate a significant mechanical role in the transmission of loads in the hip. These results suggest that it is capable of providing a support to the femoral neck and acting as a transitional structure to transfer stress from the trabecular bone of the femoral head and neck to the cortical bone of the femoral shaft. The calcar femorale can bear compression load and redistributes stress or load from the femoral head to the proximal femur. As part of a truss system, it can transform bending moment and torsional moment. It plays an important role in the proximal femoral loading system and is highly significant in the treatment of proximal femoral fractures.
Discussion
It is the function of bone to transmit the forces which move the body. One cannot, however, understand the development and shaping of living bone, which constitutes its anatomy, without understanding the complex relationships which exist between it and the forces to which it is subjected.
A pivotal name attached to the present day understanding of the anatomy and function of the upper femur in this respect is that of Julius Wolff, 17 who promulgated two theories in regard to the relationship of bone to the forces traversing it – his ‘Law of Bone Remodelling’ and his ‘Trajectorial Theory’. These terms are often used synonymously but, conceptually, they are completely different. Wolff’s ‘Law of Bone Remodelling’ considers the response of living bone to the physiological forces passing through it, whereas his ‘Trajectorial Theory’ relates to the actual path which these forces take through the trabecular bone, shown by the trabecular formations which depicts the mechanical processes taking place within it, with particular reference to the upper femur.
Wolff’s law
Wolff derived his ‘Law’ by studying the effects of physiological forces on the shape of the bones and their internal trabeculae after their fractures or osteotomies had healed. 18 His ‘Law of Bone Remodelling’ states: ‘Every change in the form and function of bone, or of their function alone, is followed by certain definite changes in their internal architecture, and equally definite alteration in their external confirmation, in accordance with mathematical laws’.
This ‘Law’ relates to the effect of a physiological force passing repeatedly through living bone and essentially states that bone will form in relation to the forces to which it is subjected and is applicable to bone in general. 18 ‘The response of the bone’, says Wolff, ‘is that it will adapt its shape and architecture in order to meet the physiological demands upon it’. 17
Avrunin and Tses, 19 however, note that, in formulating his ‘Law’, Wolff had incorrect ideas on skeletal biology, inasmuch as he based it on a static ‘mathematical’ relation between the trabecular architecture and the stress trajectories. In addition, they say, Wolff also refused to accept other facts that were available at the time. Despite this, Wolff promulgated his theories enthusiastically and widely, the result of which is that his ‘Law’ remains widely accepted, even today. Looking at the positive aspects, Avrunin and Tses go on to say that Wolff’s contribution to the popularization of the scientific discipline which has emerged, that is, Mechanobiology, is still highly esteemed as it has not only scientific but also clinical significance.
There is evidence that architectural adaptations follow a major change in bone loading, 20 and the concept and law which Wolff puts forward forms only one of the existing models that reflect the characteristics of skeletal mechanobiology. The ideas put forward more recently by Frost hold great sway. All modelling and remodelling of bone, he wrote, is undertaken by osteoblastic drifts, which add additional bone to the structure, or by osteoclastic drifts, which removes bone (Figure 2). The overall effect of the combined action of both these drifts is to sculpt the bone and ‘move it’ through the tissue space in order to align the bone with the force acting upon it and to develop the appropriate strength to meet the physical demands. 20

Schematic diagram showing how a deformed bone is remodelled through the tissues to align with the force and strengthen itself under the action of osteoblastic and osteoclastic ‘bone drifts’.
The modelling of bone is largely controlled by mechanical factors. The feedback mechanism for this process is governed by the strain within the bone. 20 –24 Generally, bone attempts to maintain the strain within it, arising from normal activities, to lie within a physiological range of somewhere between 0.0050 and 0.0015 unit strain. 20,25 Large mechanical loads deform or strain bone. Where strains exceed a modelling threshold level of about 0.0015 microstrain, modelling slowly lays down bone in order to align it with the applied stress and to strengthen it by increasing its thickness or diameter. As a result of becoming stronger, the bone will, in turn, reduce the level of strain within it back into the normal physiological range and the modelling stops. Nevertheless, if the strains within the bone remain too high, the probability of failure increases. 20
On the other hand, if the strains become too low, the bony structures will become, relatively speaking, unnecessarily robust in relation to the body’s requirement, and energy will be wasted in synthesis, maintenance and transport of the bone, and the modelling will stop. There is no response if the strains are below a minimal level, shown to be below 0.0008–0.0015 unit strain. 20,21 When strains within the bone stay below a lower remodelling threshold range, disuse remodelling permanently removes bone. 18
Wolff’s trajectorial theory
It has long been known that the upper femur contains the two trabecular columns, best seen on the anteroposterior radiograph of the pelvis (Figure 1), which are of mechanical importance. It was probably Ward, in 1834, 26 who first noted that the configuration of these internal columns resembled that of the supports holding the gas lamps to their stanchion, which were commonplace in London at the time (Figure 3). He proposed that the bony columns within the femoral neck individually conduct a tension and a compression force as did the gas lamp supports. The concept that, mechanically, the trabeculae within the femoral neck act in this way has prevailed until the present time.

Schematic illustration of Ward’s diagrams showing that the mechanical configuration of the bone within the upper femur resembles that of the supports for an old fashioned gas lamp, both having struts to carry the resultant tension and compression forces.
These ideas were later enhanced when, in 1866, HG Meyer, Professor of Anatomy, presented a series of drawings of the internal trabecular structure of various human bones at a meeting of the Natural Science Society in Zurich (Figure 4). 27 It was there that he began an association with Professor Carl Culmann, a German structural engineer and originator of the structural optimizing technique Graphic Statics. Culmann had told von Meyer that, as shown by Graphic Statics, his drawings of the trabecular structures within the upper femur resembled the internal stresses within a curved loaded Fairbain crane, a project which Culmann had been working on (Figure 5). Wolff later entered into association with Culmann and ultimately published his Trajectorial Theory which considers that ‘in the proximal end of the human femur cancellous bone is present only along the mathematical stress trajectories’, showing the paths of both tension and compression through the region. In addition, he was emphatic that in order to meet the mechanical requirements of Graphic Statics, these columns have to cross orthogonally (i.e. at 90°) within the femoral head so that they are not subjected to any shearing stress. 17

Representation of the trabecular patterns within the femoral neck from G von Meyer’s dissections.
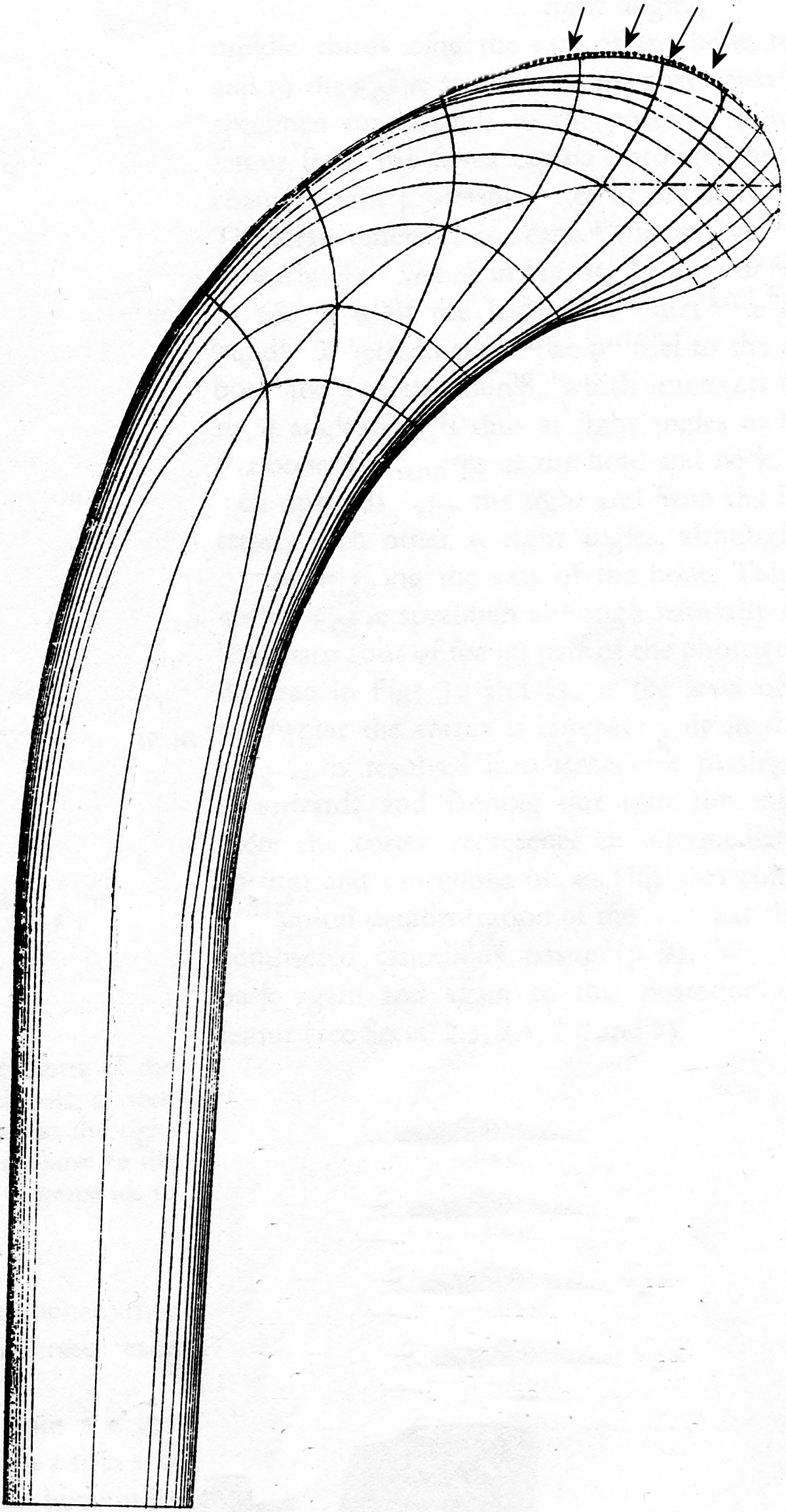
Schematic illustration, after K Culmann, of the tension and compression force lines within a curved Fairbain crane, as derived by Graphic Statics.
Wolff’s Trajectorial Theory, like Ward’s depiction of the stresses within the staunchion of the London gas lamps, considers the vertical trabecular column as conducting a compression force while the horizontal trabecular column conducts a reciprocal tension force.
This theory appears to apply reasonably well when the hip is considered to be in the extended (body upright) position during walking and limited hip flexion but it is acknowledged that it is not known how the bone of the upper femur conducts the, sometimes major, forces generated while the hip joint moves from full extension (standing and walking) to full flexion (squatting and climbing). 28 –30 In addition, the Trajectorial Theory itself has come in for a number of diverse criticisms, 31 particularly the idea that the horizontal column conducts a tension force. This has been rejected by a number of authors who consider that this column also conducts a compression force. 5,11,32 –36 As a final arbiter, the findings of a series of anatomical, three-dimensional dissections of the upper femur 2 question the Trajectorial Theory by revealing contrary anatomical findings inasmuch as they revealed that the two trabecular columns do not lie in the same coronal plane, rendering Wolff’s theory mechanically invalid. So, the main problem with the Trajectorial Theory is its limitations inasmuch as it only considers the forces within the upper femur two dimensionally, that is, those arising during standing and walking, whereas the upper femur is a three-dimensional structure. 1,4,5,11
During physiological activities, such as standing, walking, running, sitting, squatting and climbing, it is the function of the hip, with the leg below, to support the superincumbent body weight, regardless of the position of the joint. For this purpose, any force between the femur and pelvis must cross through the dome of the acetabulum. It is accepted that the force impinging upon the femoral head is the resultant of those forces arising from both gravity and muscular action. 37 As a result of this ‘resultant’ force acting on the femoral head, an equal, ‘reactive’ force arises within it. Both these forces, ‘resultant’ and ‘reactive’, are compressive in nature (Figure 6).

Schematic two-dimensional representation of the resultant force of weight bearing, showing its relationship to the internal vertical and horizontal trabecular columns at the times of full extension and full flexion of the hip joint.
According to Wolff’s Law, force precedes bone. Accordingly, it must be borne in mind that the internal structures of the femoral neck, namely, the two trabecular columns and the calcar, form in response to the strains generated by the (compression) forces traversing the region. The paths of the forces of weight bearing through the femoral head and neck can thus be visualized by following the trabecular structures within it.
The vertical trabecular column is associated with standing and walking. It begins just under the superior surface of the femoral head and passes down to the medial cortical wall of the femur at the junction of the femoral neck and shaft. It is confirmed by the dissections of the upper femur 2 and radiographs that, with the hip extended, the vertical resultant force initiated by standing passes through the dome of the acetabulum and impinges upon the superior surface of the femoral head (Figure 6(a)). This force is straight. On passing through the joint space, it sets up a reactive force within the femoral head which aligns with it. This reactive force is also straight and passes almost vertically down through the centre of the femoral head. The nature of both the resultant and reactive forces is that of compression, which generates a line of stress within the bone, the consequence of its passages through the femoral head and neck being the formation of the vertical trabecular column.
Following Wolff’s Trajectorial Theory, 17 the horizontal trabecular column is widely associated with a tension force during standing although it is difficult to see why this is so. The femoral dissections and radiographs confirm that this column begins just under the anterior surface of the femoral head 2 and passes horizontally, in a curvilinear fashion, across the inner cortical surface of the femoral neck to end in a small buttress on the inner cortex of the antero-superior femoral shaft. The dissections also show that when the hip is flexed the femoral head rotates vertically and the erstwhile anterior surface moves up into the femoral acetabular dome where it is directly under the resultant force of weight bearing (Figure 6(b)). As with standing, this resultant force sets up a reactive force within the femoral head which aligns with the resultant force. Again, both these forces are straight. The major difference between the standing and squatting postures is that during active squatting, the bony tissues of the upper femur move across this line of force. It is hypothesized that, as a result of this movement, a curved line of strain is generated within the bone, which stimulates a line of bone formation reflecting the arc of motion of the upper femur. It must be noted that, despite the femoral head rotating, the impinging resultant force remains the same; that of compression. It is then further hypothesized that it must be accepted that the horizontal trabecular column carries a compression force, not a tension force.
The recent three-dimensional anatomical dissections 2 showed that the calcar femorale is a thick, broad, strong plate of bone throughout its length and that its orientation is predominantly vertical (Figure 7). The photograph also shows that the calcar femorale has strong attachments to the lateral ends of both the vertical and horizontal trabecular columns as well as attachments to the surrounding bone of the upper femoral shaft. It is hypothesized that the calcar is involved with the forces traversing the upper femur in several ways.
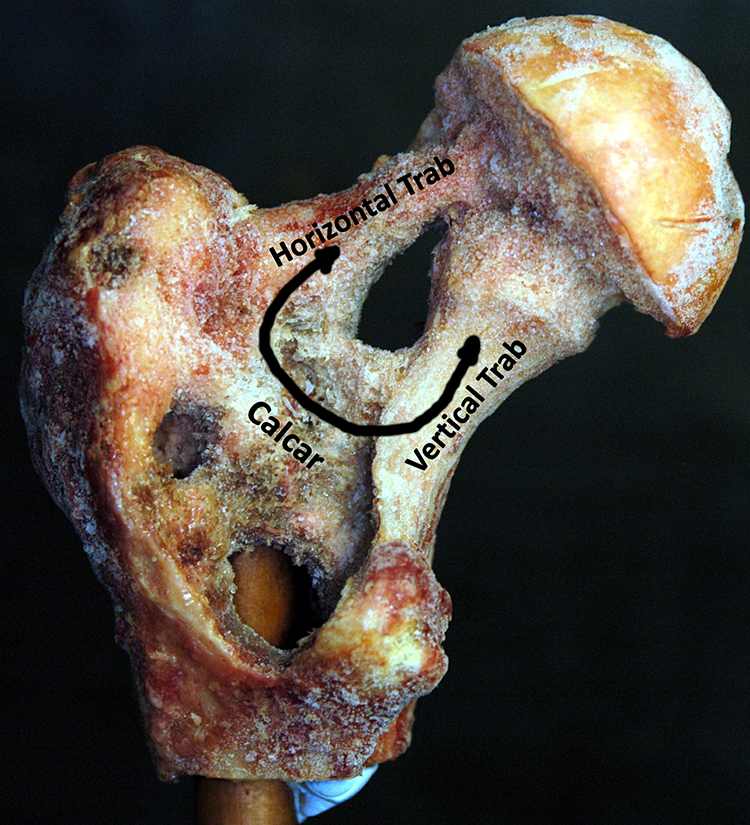
Photograph of a physical dissection of the upper femur. Note that the calcar is orientated obliquely upward and has substantial connections with both the horizontal and vertical trabecular columns and the upper femoral shaft. The double arrowed line shows the course of the hypothesized compression force through the calcar generated during the hip flexing and extending under load.
The junction between the femoral shaft and the femoral neck is not curved but angular. 38 This is demonstrated by the fact that, on an anteroposterior X-ray image of the human hip, straight, not curved, lines can be drawn down the middle of each of their shafts, the angle which they subtend being known as the ‘neck/shaft angle’. The dissections 2 show that the calcar lies along the line of this junction.
The change of direction between the femoral neck and femoral shaft suggests that, mechanically, this is an area of strong, as yet undefined, shear and rotatory stress within the bone, arising from the physiological movements of the hip. It is suggested that this junction can be classified mechanically as a ‘moment connection’, which is designed to accommodate such forces. 38 This being so, it is hypothesized that the calcar arises partially in response to these forces and provides a necessary internal support to help meet the physical strains of this ‘joint’.
The lateral end of the horizontal trabecular column lies antero-superiorly, and the lateral end of the vertical trabecular structure lies at the inner aspect of the medial neck/shaft junction. Figure 7 shows that the calcar stretches across between these ends of the two trabecular columns and has strong attachments to the ends of both. From this, it is hypothesized that the calcar acts to provide a base for the two trabecular columns, forming with them a unified internal trabecular structure which gives a necessary internal support, within the femoral head and neck, to carry the forces of weight bearing through them.
It is not clear exactly how the reactive force passes through the femoral neck as the resultant force transits across the antero-superior surface of the femoral head during flexion movements of the hip joint (Figure 8). It is noted, in Figure 6(b), that it is at full flexion that the resultant force is over the proximal end of the horizontal trabecular column. This suggests that, during flexion of the hip, the reactive force passes up from the lateral end of this column rather than going down it. This being the case it means that at the initiation of flexion, when the hip is fully extended and the reactive force is in the vertical column, the reactive force moves up through the calcar from the end of the vertical column to the lateral end of the horizontal column, before passing into it, confirming that the calcar and the two trabecular columns are one unified structure.
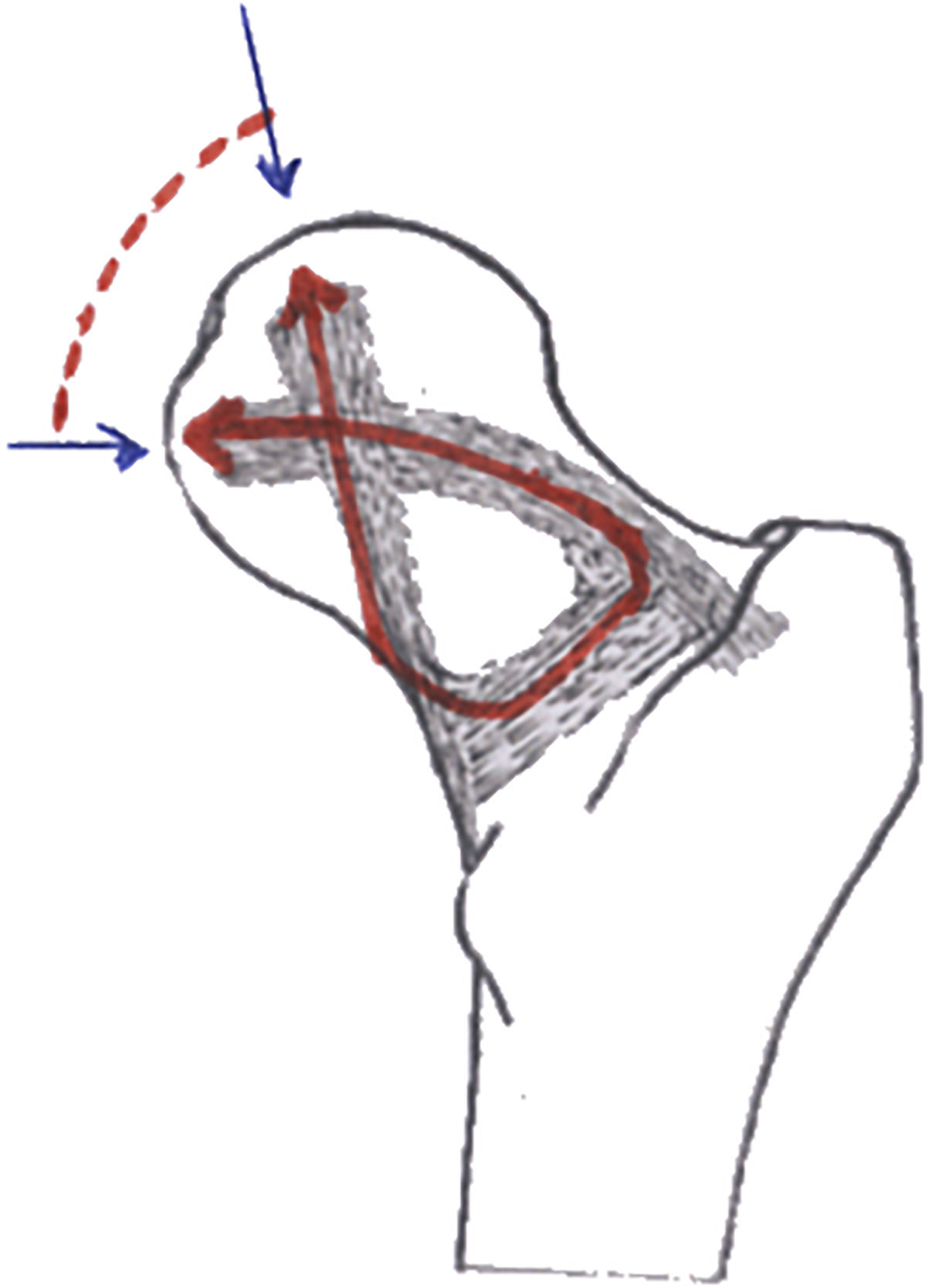
Two-dimensional depiction of the possible figure of eight course of the reactive compression force passing through the femoral head and neck during flexion and extension of the hip joint.
The calcar has strong connections with the upper femur laterally and medially suggesting that it is through these that the calcar disseminates the compression forces from the trabecular columns into the femoral shaft, particularly posteriorly where the cortex is particularly thin.
The upper femur consists of an admixture of cortical and trabecular bone. Wolff himself states ‘The cortex is involved in the architectural structure of the bone as much as is the cancellous tissue’. 17 While the trabecular bone may have formed an internal support structure of cancellous bone, it must be remembered that it is also the role of cortical bone to transmit forces acting upon it.
The majority of experimental studies of remodelling in bone have focused on cortical bone. 39,40 Only a limited number of studies have dealt with trabecular bone experimentally. As a result, the mechanisms of bone adaptation to mechanical forces in this substance are not well understood. Nevertheless, it has been shown that cancellous bone appears to respond in the same way to the applied forces as cortical bone does. 41
This being so the upper femur can be considered, anatomically, as being made up of three different elements – the cortical bone of the femoral shaft, the cortical bone of the femoral head and neck and the cancellous bone of the internal trabecular structures of the femoral head and neck.
Undoubtedly, the forces passing through the upper femur during activity are complex. Similarly, the forces responsible for the remodelling of the different elements of the bone of the upper femur must be equally complex. It is unlikely that a single force (e.g. that from simply standing) will satisfy all the remodelling requirements of both the cortical elements and the cancellous bone constituting the upper femur.
The actual forces responsible for modelling and remodelling the cortical bone of the upper femoral shaft and femoral neck and maintaining the neck shaft angle, from foetus to adult, are unknown. It is nevertheless hypothesized that at least two separate resultant forces are required for the cortical bone alone, one for the shaft and one for the neck. It is probable that these two forces are constant and overriding as the shape of the femur and the neck/shaft angle, once formed, remain relatively constant through life.
It is known that the cortical and cancellous bone of the upper femur share the load passing through the hip joint, 39,40 although the exact proportions in which they do it are unclear. It is hypothesized in this present article that, constrained by the more or less fixed shape of the cortical bone of the upper femur, which has its own modelling stimuli, the compression force generated by the physiological actions of the hip, in whole or in part, passes through the region in such a way that (a) the cancellous bone generated by this force fulfils the need for additional, appropriate reinforcement of the upper femur and (b) the remodelling of both the cortical and the cancellous bone, in the face of these two different modelling stimuli, is balanced.
Conclusion
The calcar has a central role in dealing with the complex forces which occur at the femoral shaft/neck junction of the femur. The anatomical study suggests that, in addition to the local stress, it receives a large proportion of the forces of weight bearing coming down through the femoral neck and transmits them to the upper femur.
While this is occurring, it must be borne in mind that both the cortical and trabecular bone of both the upper femoral shaft and the femoral neck are affected by two types of forces: constant modelling forces which maintain the shape of the bone and intermittent motor forces which bring about the movements of the hip. It is hypothesized that both have different modelling effects but, as the external shape of the upper femur remains much the same, some compromise between them is present. It is suggested that this takes the form of developing the system of trabecular bone within the femoral neck which conducts the forces moving the body in such a way that the combined modelling effects of forces are balanced and have the least possible effect on the shape of the bone.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.