
Abstract
Purpose:
Distal metaphyseo-diaphyseal humeral fractures are challenging particularly if open, comminuted, or associated with nerve injury. In cases of open distal complex metaphyseo-diaphyseal humeral fractures inamenable for traditional methods of fixation, retrograde intramedullary locked humeral nail with a new lateral condylar point of entry has been proposed.
Methods:
Two phases of study were conducted; phase I comprised computerized tomography evaluation of right humeri of 120 adult subjects, while phase II entailed prospective analysis of 18 patients who sustained firearm injuries resulting in open distal metaphyseo-diaphyseal humeral fractures associated with radial nerve injuries. All patients were surgically managed using lateral condylar retrograde humeral nailing with primary radial nerve exploration.
Results:
Distal sagittal medullary diameter of the humeral medulla was the narrowest in comparison to axial and coronal medullary diameters in phase II, which matched the results of phase I. The mean postoperative disability of the arm, shoulder, and hand score was 11.2 ± 6.4. Only five patients underwent subsequent successful tendon transfer.
Conclusions:
Lateral condylar retrograde humeral nail with early radial nerve exploration in cases of high-energy distal metaphyseo-diaphyseal humeral fractures yielded good results regarding union and spontaneous radial nerve recovery or later on reconstruction.
Introduction
Humeral fractures account for 1–3% of all adult fractures. 1 Surgical management is indicated for such fractures when they are irreducible, pathologic, associated with vascular or nerve injuries, associated with ipsilateral forearm fractures (floating elbow), or when the fracture pattern is unstable (short oblique or transverse) in active adult patients. 2,3 These particular fractures may be associated with devastating complications whether in the initial trauma setting or consequent to treatment. The most disabling complication is radial nerve injury, which is estimated to take place in almost 11–12% of cases of which 12.4% complicates treatment. 4,5 Lim et al. have found that radial nerve injury secondary to plate osteosynthesis of humeral shaft fractures ranges from 5.1% to 17.6%. 6
Open humeral diaphyseal fractures magnify the challenge imposed on the treating surgeon. Classically, when radial nerve injury complicates open humeral fractures resulting from firearm injuries, the treatment protocol should be staged: (1) primary radical soft tissue and osseous debridement and (2) secondary osteosynthesis of the fracture with/without bone shortening, and finally neurorrhaphy, nerve grafting, or tendon transfer procedure according to the underlying situation. 7
Various surgical approaches and diversity of implants have been proposed for surgical management of humeral shaft fractures. One of the most appealing options, that is advantageous both biologically and biomechanically, is the intramedullary locked humeral nail. 8 This treatment modality could be the method of choice in cases of pathological fractures, segmental fractures, severely comminuted types 12C1, 12C2, and 12C3 according to Orthopaedic Trauma Association (OTA)/Arbeitsgemeinschaft für Osteosynthesefragen (AO) classification system when there are adequate proximal and distal humeral fragments for application of the locking screws, and in open fractures types I–IIIA according to the Gustilo and Anderson classification. 9,10 Intramedullary locked humeral nails provide well-defined biological advantages via minimal invasive technique of insertion, leaving fracture hematoma undisturbed and preserving periosteal blood supply. These advantages could be provided with some other methods of fixation but with increased risk of iatrogenic nerve injuries. 11 Biomechanically, they provide immediate stable load sharing construct in addition to neutralizing torsional, bending, and shear stresses. Consequently, the patient gets immediate pain relief, earlier rehabilitation, and better nursing. 12
Nevertheless, the use of antegrade humeral nail carries the potential risk of rotator cuff injury, shoulder impingement, injury of axillary nerve, circumflex arteries, or biceps tendon irritation, which could result from proximal screws insertion. 12 –15
When retrograde humeral nail is applied, the distal part of the humerus should be intact allowing proper insertion of the nail to avoid the potential complication of longitudinal shuttering of the humeral shaft. 12 Complex distal humeral fractures represent an obstacle for both retrograde humeral nail insertion and application of the distal locking screws of the antegrade humeral nail. In such situations, plating and external fixation seem rational alternatives. However, in cases of defective soft tissue coverage or massive energy trauma, intramedullary nail fixation serves a good solution. Based on these facts, a new entry point through the lateral humeral condyle has been proposed to overcome such obstacles.
Our hypothesis is that performing osteosynthesis using retrograde locked humeral nail from lateral condylar entry point represents an alternative surgical option for management of high-energy distal humeral diaphyseal fractures with the facilitation of future radial nerve management without adding more fibrosis to the injury zone. All patients recruited for this study have signed full informed consent and our institution’s human ethical committee approval was obtained.
Methods
This study was conducted in the Department of Orthopedic Surgery and Department of Radiology of our center in a two-arm fashion. Phase I of the study took place in the period from February 2014 to February 2015 by the third author as a preliminary radiological step in preparation to phase II. One hundred twenty adult subjects, who were initially scheduled for computerized tomography (CT) examination of the right upper limb for different medical indications, were included after obtaining individualized full informed consent implying their willing and approval to participate in this study and were allocated equally into two groups according to gender with variable ages and heights. They underwent CT evaluation of their right humeri for determination of specific angles and dimensions that were relevant to phase II of the study. Phase II of the study comprised a prospective analysis of 18 patients who were initially diagnosed as having open fractures of the distal humerus (graded as Gustilo and Anderson types IIIA) and managed using retrograde humeral nail with a modified distal humeral entry technique. All patients were operated in the period from March 2015 to March 2016. All surgical procedures were performed by the first and the fourth (senior) authors, while the patient clinical and radiological follow-up was done by the second author.
Phase I (radiological evaluation)
One hundred twenty subjects, allocated equally into two groups according to their gender, underwent CT evaluation of their right humeri. Multislice CT was done for all subjects using 16-slice multidetector CT (MDCT) machine (GE bright speed, GE Healthcare, Waukesha, Wisconsin, USA) with the same examination protocol using 64× 0.5 mm collimation scanner with a gantry rotation speed of 400 ms/rotation, image thickness 0.5 mm, standard pitch factor of 0.641, and reconstruction interval 0.5 mm. Each scan was obtained with a tube voltage of 120 kV and 250 mA.
Measurements
Axial cuts were taken of the upper limb from above the shoulder joint down to below the elbow joint. Images were transferred to a separate advanced workstation with commercially available software that allowed the following measurements (Figures 1
to 3): Humeral length was measured on coronal reconstructed images. Angle between the outer cortex of lateral column and the diaphysis (intercortical angle (ICA)). Angle between the medulla of lateral column and the diaphysis (intermedullary angle (IMA)). Diameter of the medullary canal at the lateral column on axial lateral column diameter (ACD), coronal lateral column diameter CCD), and sagittal lateral column diameter (SCD) images. Diameter of the medullary canal at the diaphysis on axial diaphyseal medullary diameter (AMD), coronal diaphyseal medullary diameter (CMD), and sagittal diaphyseal medullary diameter (SMD) images.

Coronal reconstructed MDCT image of the right humerus showing the way of measurement of ICA and IMA. ICA: intercortical angle; IMA: intermedullary angle; MDCT: multidetector computerized tomography.

Coronal reconstructed MDCT image of the right humerus showing the way of measurement of lateral and medial distances to the center of lateral column medulla. MDCT: multidetector computerized tomography.

Axial reconstructed MDCT images of the right humerus showing ACD (right) and AMD (left). MDCT, multidetector computerized tomography; ACD: axial lateral column diameter; CCD: coronal lateral column diameter; AMD: axial diaphyseal medullary diameter.
The center of the most appropriate area for nail insertion according to templating portraying the most distal part of the lateral column medulla with an estimation of the distance from the lateral and medial cortices to the center of this exit.
Phase II (clinical study)
A prospective analysis of 18 patients (14 males and 4 females) with a mean age of 37.4 ± 11.6 years (range 22–60) who sustained open fractures of the distal humerus secondary to firearm injury (FAI) (graded as Gustilo and Anderson type IIIA) and managed using retrograde humeral nail with a new entry technique was conducted (Table 1). All patients recruited for this study were thoroughly evaluated both clinically and radiologically. Clinically, all patients were assessed regarding the associated wound with the evaluation of its size, nature and cleanliness, peripheral nerves affection in addition to the peripheral vascular status. Radiologically, at least two views perpendicular to each other were obtained to accurately estimate the type and pattern of the fracture and the integrity of the distal humeral lateral column. In addition, MDCT scan of the affected humerus was performed to all patients to facilitate preoperative planning.
Patient demographic data.a

aAll patients sustained firearm injury. All patients had radial nerve injury.
Inclusion criteria
Patients’ age ≥18 years at the time of injury. FAI. Primary radial nerve injury. The minimal proximal extension of the fracture equals the maximum width of the distal humerus (Figure 4).

Anteroposterior radiograph of the distal humerus demonstrating the maximum width of the distal humerus (line A) with the equivalent line (line B), which represents the minimal required length of the lateral column for application of lateral condylar retrograde humeral nail.
Exclusion criteria
Previously malunited fractures of the same humerus obviating the use of intramedullary nail. Skeletally immature patients. Intra-articular extension of the fracture. Fractures involving lateral supracondylar ridge. Generally unfit patients for receiving general anesthesia.
Postoperatively, all patients were evaluated both clinically and radiologically. Clinically, disability of the arm, shoulder, and hand score (DASH) 16 and visual analog scale (VAS) pain score were used for evaluation. In addition, the British Medical Research Council’s muscle testing scale was used for evaluation of the motor recovery of the radial nerve. 17 Radiologically, bony union and stability of fixation were evaluated.
Preoperative planning
All patients recruited for this study were subjected to standard preoperative planning by obtaining true anteroposterior and lateral views of the injured humerus including both shoulder and elbow joints. The employed humeral nail radiolucent overlay template (specially designed for the nails used; Treu, Germany) was routinely extrapolated on both views in the manner displayed in Figure 5. In this way, the following data could be obtained and preoperatively determined: the appropriate diameter of the nail to be used, the exact entry point of the nail through the extra-articular portion of the lateral humeral condyle, and the suitable nail length.

(a) Templating of the retrograde humeral nail on both A/P and lateral X-ray views (courtesy El Shafie M) and (b) the starting point of nail entry on a humeral bone demonstrating that the entry point does not violate the articular surface.
Surgical technique
After induction of general anesthesia, the patient was positioned in the supine beach chair position, while the whole involved upper limb completely scrubbed, draped, and supported on a radiolucent side table to allow proper manipulation, reduction, and nail insertion. The first step in the procedure entailed thorough debridement of the wounds resulting from the initial injury (Figure 6). This was followed by exploration of the radial nerve through the initial wound or through an extension to the anterolateral approach. Radial nerve was then either neurolyzed (if found in continuity) or tagged if initially disrupted for later on reconstruction. Regarding fracture fixation, the same surgical technique adopted by the senior author that was initially published in 2002 was followed 18 (Figures 7 and 8). A small stab incision was centered 1–1.5 cm distal and medial to the tip of the lateral humeral epicondyle. This corresponds to the proposed entry point according to the preoperative templating. The entry point was initially created in an extra-articular fashion using the awl of the humeral nail paralleling the humeral lateral column medulla, followed by introducing a curved guide wire to bypass both the lateral column and the diaphyseal medullae. This was followed routinely by opening the medulla of both the lateral column and the diaphyseal medulla using flexible reamers with increasing increments to facilitate the introduction of the nail. An interlocking intramedullary humeral nail (Treu, Germany) was then introduced in a retrograde fashion after removal of the guide wire (as the used nail was non-cannulated in all cases) in a gentle rotatory movement until the top end of the nail was seated flushed with the distal humerus. This nail has an angle of 5° at the bend between its proximal and distal parts. This system of nails provides solid noncannulated (6.5–9.5 mm in diameter) and cannulated (8–10 mm in diameter) nails with two proximal and two distal locking screws. The most proximal humeral locking screw (now the most distal) was placed in a diagonal manner in a dynamic hole using the proximal aiming device so that it bypasses the superior margin of the olecranon fossa and the most distal locking screw (now the most proximal) was placed from anterior to posterior percutaneously in a free-hand style.

Clinical condition of the patient.

Preoperative X-rays.

Immediate postoperative X-rays.
In cases associated with crushed radial nerve injury, tendon transfer surgery was performed 6 months later if no nerve recovery was reported to regain satisfactory motor power comprising flexor carpi ulnaris transfer to the extensor digitorum communis, palmaris longus transfer to the rerouted extensor pollicis longus, and the pronator teres to the extensor carpi radialis brevis.
Postoperative rehabilitation
All patients were instructed to undergo passive range of motion (ROM) exercises of the shoulder and elbow starting from the first postoperative day until day 14 under the supervision of an upper limb professional physiotherapist. This was followed by protected active ROM for the next 4 weeks. Gradual unprotected active ROM was first allowed according to the progress of bony union, which was monitored sequentially on monthly based radiographs.
Statistical analysis
All data of both arms of the study were analyzed with the use of Statistical Package for Social Sciences) 13.0 for Windows. Average values were presented as means ± standard deviation. The χ 2, independent sample t, Mann–Whitney, and Pearson’s correlation tests were used for statistical analysis of the data. When the p value was <0.05, the result was considered statistically significant.
Results
The results of phase I of the study are outlined in Tables 2 and 3. Regarding the MDCT diameters of the lateral column medullary canal in all planes, there were no significant differences between the two examined groups. Regarding AMD and CMD group I, male group showed statistically greater dimensions in relation to group II (female group) (p < 0.001). On the other hand, the SMD showed a statistically significant increase in the male group only when measured just proximal to the olecranon fossa (p = 0.037). There were statistically significant differences between both groups regarding the center of the entry point in favor of male group laterally and the female group medially (p < 0.001).
Results of phase I of the study (radiological evaluation).a

ICA: intercortical angle, IMA: intermedullary angle. ACD: axial lateral column diameter, CCD: coronal lateral column diameter, SCD: sagittal lateral column diameter.
aIndependent samples t-test for quantitative data between both sexes.
bSignificance level at p value <0.05.
Results of phase I of the study (radiological evaluation).a

AMD: axial diaphyseal medullary diameter, CMD: coronal diaphyseal medullary diameter, SMD: sagittal diaphyseal medullary diameter.
aIndependent samples t-test for quantitative data between both sexes.
bSignificance level at p value <0.05.
When analyzing group I subjects, the distal SMD was negatively correlated to the age of the patients (p = 0.001). There was a statistically positive correlation between the ICA on one hand and IMA, lateral distance to enter the medulla and medial distance to enter the medulla on the other hand (p < 0.001, 0.007, 0.021, respectively). Similarly, the IMA was positively correlated to the lateral distance to enter the medulla with statistical significance (p = 0.014). The SCD showed a statistically significant negative correlation to both lateral and medial distances to enter the medulla (p < 0.001). The lateral distance to enter the medulla showed a statistically positive correlation to the medial distance to enter the medulla (r = 0.875; p < 0.001). The distal SMD was negatively correlated to both the lateral and medial distances to enter the medulla with no statistical significance, while the proximal SMD was negatively correlated to both the lateral and medial distances to enter the medulla but with statistical significance (p < 0.001). The proximal SMD showed a statistically positive correlation to the SCD, CMD, and distal SMD (p = 0.002, 0.046, 0.004, respectively).
As for group II patients, the distal SMD showed a statistically significant negative correlation to age (p = 0.006). The IMA showed a statistically positive correlation to both the lateral and medial distances to enter the medulla (p = 0.013, 0.02, respectively). The ACD was negatively correlated to the medial distance to enter the medulla (p = 0.04).
Both AMD and CMD showed a statistically significant positive correlation to the lateral distance to enter the medulla (p = 0.034, 0.027, respectively). The SCD showed a statistically negative correlation to both lateral and medial distances to enter the medulla (p < 0.001). The lateral distance to enter the medulla was positively correlated to the medial distance (p < 0.001). The proximal SMD showed a statistically negative correlation to both the lateral and medial distances to enter the medulla (p = 0.006, 0.001, respectively).
The proximal SMD was significantly positively correlated to each of AMD, CCD, SCD, and distal SMD (p = 0.043, 0.042, 0.003, 0.002, respectively).
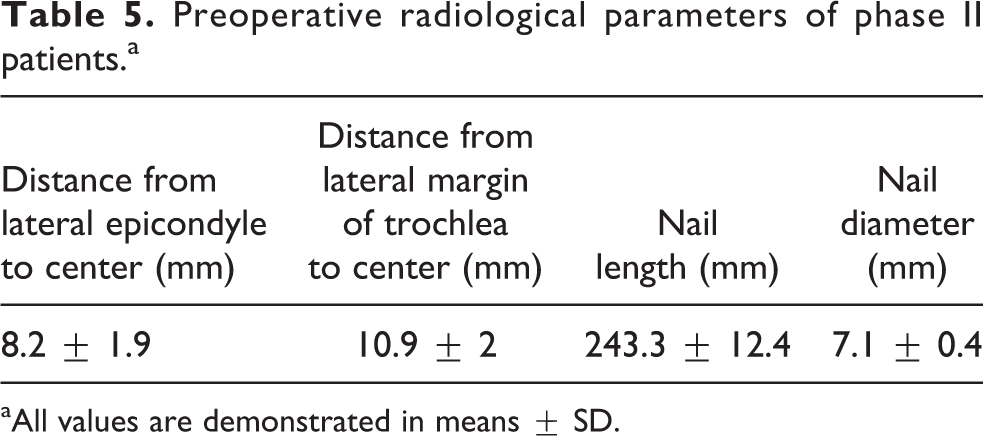
Regarding phase II (Tables 4 –7), patients had 11 right and 7 left affected humeri. The dominant limb was right in 13 and left in 5 patients. The mean time lag to the index surgery was 5.2 ± 8.9 days (range 0.2–30). Initial debridement with exploration of the radial nerve and insertion of the retrograde humeral nail constituted the procedure in 11 cases, while secondary insertion of the nail was the status in 7 cases. In only two cases (11.1%), there were other associated injuries including forearm and femoral fractures. The radiological dimensions of the distal part of the diaphyseal medullary canal showed that the distal SMD was the narrowest in comparison to the AMD and CMD (8.4 ± 0.5 mm, 10.9 ± 1.6 mm, 11.1 ± 1.6 mm, respectively), which emphasized the radiological results of our study. On the other hand, the ACD, CCD, and SCD were nearly similar (13.1 ± 1.9 mm, 12.1 ± 1.2 mm, 12 ± 2.1 mm, respectively). The mean diameter of the used nail was 7.1 ± 0.4 (range 6.5–7.5 mm), which means that the most suitable nail diameter to be used with this technique is 7 mm. No single case exhibited a narrower lateral column or lateral medullary diameter that necessitated the use of narrower nail than 6.5 mm. The mean length of the nails used was 24.3 ± 1.2 cm (range 22–26).
Preoperative radiological parameters of phase II patients.a

ICA: intercortical angle; IMA: intermedullary angle.
aAll values are demonstrated in means ± SD.
Preoperative radiological parameters of phase II patients.a
aAll values are demonstrated in means ± SD.
Postoperative results of the patients of the study.a

All values are demonstrated in means ± SD. ROM: range of motion; DASH score: disability of arm, shoulder and hand score.
aAll values are demonstrated in means ± SD.
bThe (−) sign means lag of extension.
Results of radial nerve surgery in phase II patients.
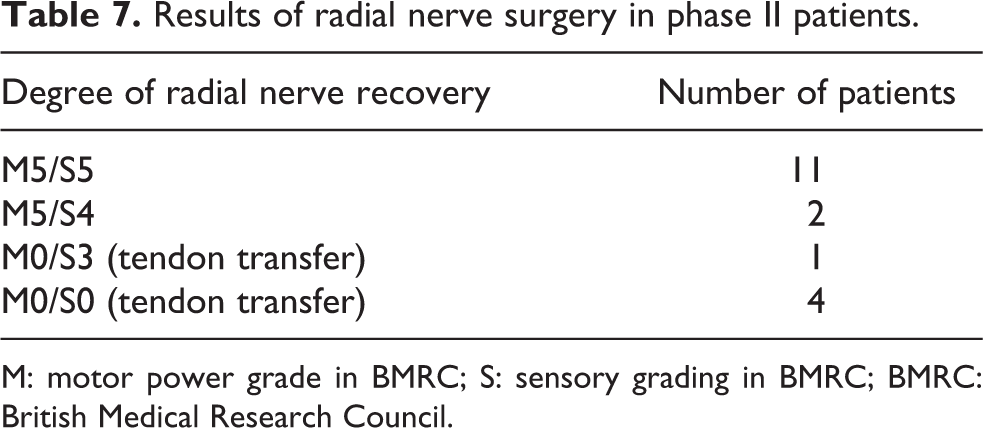
M: motor power grade in BMRC; S: sensory grading in BMRC; BMRC: British Medical Research Council.
All patients included in this study were followed up for a mean period of 26.7 ± 6.2 months (range 24–36) and all went to full union at a mean time of 4.9 ± 1 months (range 3–6) (Figure 9). The mean elbow active ROM (extension lag/maximal flexion) was −6.1 ± −4°/120.3 ± 5.8°. The shoulder joint showed a full ROM in comparison to the other side. The average DASH score was 11.2 ± 6.4 (range 4.2–21.7). The mean VAS was 2.1 ± 0.8 (range 1–3). Radial nerve injury ranged from contusion 13 to crushing 5 with no cases of nerve transection. Nerves spontaneously recovered in 13 patients during follow-up achieving full motor recovery and variable sensory recovery, while the other five patients needed tendon transfer, which was eventually performed with good results.

Follow-up X-rays 1.5 and 6 months postoperatively.
Apparently, the diameter of the nails used in our patients showed a statistically positive correlation to both AMD and SMD (p = 0.015, <0.001, respectively). The AMD showed a statistically positive correlation to the ACD and the CCD (p = 0.039, 0.011, respectively). Similarly, the CMD showed a statistically positive correlation to ACD, CCD, and SCD (p = 0.002, 0.002, 0.03, respectively). The mean time estimated for delay to the index surgery in cases of other injuries association (27.5 ± 3.5 days) was statistically longer than isolated humeral fracture cases (2.5 ± 3.9 days) (p = 0.024).
Recovery of the associated radial nerve injury showed statistically negative correlation to the DASH score value (p < 0.001). In some cases of the study, the most distal nail screw (the most proximal in location in the arm) might have been longer than should be however; this resulted in no complications regarding nerve irritation or injury. In all cases included in this study, no infection, nonunion, failure of fixation, iatrogenic nerve, or vascular injury was encountered. Only two cases of varus malunion were seen clinically despite not evaluating the postoperative radiological angle of the distal metaphyseal–diaphyseal segment. The capitellar articular surface was never violated with no subsequent radiocapitellar osteoarthritis.
Discussion
The use of locked intramedullary nails for humeral shaft fractures is advantageous both biologically and biomechanically. Relatively, recent studies have shown that rates of union in comminuted humeral fractures after application of intramedullary nails range from 92% to 100% in periods of 6–13 weeks. 9,12 When dealing with distal humeral diaphyseal fractures, retrograde locked humeral nailing has been shown to provide more initial stability to both bending and torsional stiffness. 19
Extremely narrow medullary canals represent a contraindication for intramedullary humeral nailing for fear of iatrogenic shuttering or nail jamming. Accordingly, extensive research has been conducted on both anatomical and radiological bases to further extrapolate the dimensions of the humerus bone. Pospula et al. have found that the medullary cavity was at its narrowest level at the supracondylar area averaging 7.5 mm. 20 Akpinar et al. had similar results to Pospula et al. 21 Murdoch et al. have estimated the medullary cavity diameter to be 12.1 ± 2.6 mm. 22 Regarding anatomical parameters of the distal humerus, the lateral column of the distal humerus normally constitutes an angle of 20° with the central axis of the humeral diaphysis and the lateral column forms an angulation in the sagittal plane with the humeral diaphysis of about 40°. 23 –25
In this study, the senior (fourth) author had proposed a new entry point for the retrograde humeral nail that was initially used for cases of pathological humeral fractures and was published earlier. 18 However, the indications have expanded to include high-energy distal humeral fractures with intact lateral column, which precludes the use of traditional antegrade or retrograde locked humeral nails. An extensive radiological assessment of the distal humerus has been conducted by the third author, which confirmed the applicability of this technique with the traditional humeral nails with an average diameter of 7 mm through the lateral humeral condyle after templating with an entry point located posterior to the capitellar articular surface and within 5.8 ± 1.5 mm from the lateral trochlear margin in males or 7.8 ± 2.2 mm in females. The continuum of the medulla of the lateral column of the distal humerus with the diaphyseal medullary canal matches the design of the proximal part of the humeral nail (Treu, Germany) with the point of nail inclination copes with the meta-diaphyseal junction. We have found an angle between the medullary canal of the lateral column and that of the distal humeral diaphysis of 149.8 ± 8.9° in males and 150.7 ± 6.2° in females, which allows the easy introduction of the antegrade humeral nail in a retrograde fashion, provided that the inclination of the proximal part of the nail to the distal part is 5°.
According to the radiological phase of the study, the narrowest humeral medullary diameter was the distal SMD, which was 7.4 mm in males and 7.3 mm in females. On the other hand, in the second phase, the narrowest medullary diameter was the distal SMD, which was 7.5 mm. Accordingly, the narrowest medullary diameter that could be appropriate for the application of this technique would be 7.3 mm, provided that the narrowest solid nail diameter is 6.5 mm.
There is strong evidence in the literature that union is delayed in both high-energy humeral fractures (average of 18.7 weeks) and in open fractures (19.7 weeks) regardless of the type of fixation used. 26,27 This copes with our results as the mean time required for union in our series was 4.9 ± 1 month (almost 20 weeks).
To overcome the problematic cases of distal humeral fractures at the meta-diaphyseal area, various fixation techniques have been advocated. Flexible retrograde intramedullary nails have been used with achieving an average time of union of 7.2–10.5 weeks. However, nonunion takes place in variable percentages (4–25%) owed to over distraction, inability to provide rotational stability or rarely due to osteolysis at the fracture site by titanium particles reaction. 26 Additionally, angular stable fixation has been successfully used but with the classic drawbacks of the plate fixation, including extensive approaches, nonunion, and infection. 27
In a comparative study between retrograde and antegrade humeral nailing, iatrogenic fissuring at the nail insertion site of 5% has been reported. 28 We have not encountered such complication in our series, which may be due to the cancellous nature of the entry point. One of the most common complications encountered when dealing with humeral shaft fractures is the malunion, which could be accepted up to 30° of varus, 20° of anterior angulation, and 15° of internal rotation, which could be compensated by the free shoulder and elbow motion. 3,29 We only encountered two cases of varus malunion in our series.
Radial nerve injuries represent one of the most common complications associating humeral shaft fractures, particularly at the meta-diaphyseal area. At this area, the nerve is relatively immobile increasing the vulnerability for traction and tension injuries. 4 –7 In cases of open fractures secondary to firearm injuries, complete radial nerve transection or disruption with or without nerve defect is usually seen. In such cases, there is a general agreement about the necessity of radial nerve exploration but still to repair or graft on a primary basis is a point of controversy. 30 Some authors advocate secondary repair or reconstruction claiming that the zone of injury will be clearly demarcated paving the way for getting more healthy nerve stumps maximizing the chances of healing. When secondary repair or grafting is undertaken in such cases, the results become better up to 70%. 30,31 Some other authors preclude secondary repair claiming that delaying nerve repair or grafting for more than 3 months reduces the capacity of motor axons regeneration into the distal nerve stump by about 35%. 32 This could be attributed to the diminished capacity of the chronically affected Schwann cells to respond to the axonally derived neurotropic signals, which has been shown to be reduced significantly after 2 months of injury. 33
Postoperatively, EMG and NCV studies usually parallel the clinical findings and their, at best, expectations precede the clinical improvement by only 1 month. 30 In our study, we adopted a strategy of primary exploration at the initial debridement or fixation followed by conservative treatment or follow-up in cases of intact nerve bundle or later on tendon transfer in cases of nerve disruption or crushing. The average time of full nerve recovery in our series was 5.8 ± 3.9 months, which coapts with the findings of Ring et al. 30
The use of intramedullary humeral nail (lateral condylar humeral nailing in this study) minimizes the mobilization and irritation of the initially traumatized radial nerve thus neutralizes the negative role of fixation method on nerve recovery. However, there are considerable risks of jeopardizing the lateral collateral ligament of the elbow, radiocapitellar joint in cases of more distal nail insertion in addition to possible iatrogenic distal humeral fracture.
As all patients recruited for the second phase of the study sustained open humeral fractures together with radial nerve injury secondary to FAI, the authors recommended simultaneous exploration to the radial nerve for assessment of the magnitude of nerve injury, in addition, to further anticipate the second step being either observation or later on reconstruction. But in cases of closed fractures, the authors recommend no exploration of the nerve until the passage of 6 weeks from the time of injury.
This study has limitations that could be confined to the lack of radiological evaluation of the left humeri in the radiological phase of the study, the small number of the patients included in the clinical phase of the study in addition to lack of the control group. The authors believe this modified entry technique for a retrograde humeral nail with early radial nerve exploration in cases of high energy distal humeral fractures yields good results regarding union and radial nerve recovery with minimal or no complications.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.