
Abstract
Purpose:
This study aims to determine the prevalence of malnutrition among orthopaedic oncology patients with malignant tumour during preoperative period.
Methods:
This is a prospective observational study involving patients from the orthopaedic oncology unit who were undergoing surgery. They were assessed with Patient Generated Subjective Global Assessment (PG-SGA), Malnutrition Screening Tool (MST) and 3-minute Nutritional Screening (3MinNS) questionnaires. Anthropometric data such as body mass index, mid upper arm circumference (MUAC) and blood parameters such as serum albumin, total lymphocyte count and haemoglobin were also investigated. Patients were then followed up for 3 months. Post-operative complications were divided into infectious and non-infectious groups. Length of stay and unplanned readmission were also documented.
Results:
Prevalence of malnutrition ranged from 13.3% to 45.8% under different nutritional assessment methods. Patients who were determined as malnourished were significantly associated with both infectious and non-infectious post-operative complications (p < 0.001). PG-SGA and 3MinNS values were also significant in univariate and multivariate analysis, respectively. Low serum albumin (<35 g/L) was associated with post-operative infectious complications, especially surgical site infection (p < 0.001), prolonged hospital stay (p = 0.009) and unplanned readmission (p = 0.017). 3MinNS and Charlson Comorbidity Index were predictive of non-infectious complications, whereas serum albumin and the presence of metastasis were predictive of infectious complications.
Conclusion:
This pilot study of patients with soft tissue and bone sarcoma of upper and lower limbs showed that malnutrition is a significant independent factor related to infectious and non-infectious complications which leads to unplanned readmission and prolonged length of stay. Periodic screening using the PG-SGA or 3MinNS questionnaires, MUAC and evaluation of serum albumin levels is recommended during clinic session and pre-surgery assessment rounds to identify those predisposed to malnutrition and help in reducing incidence of post-operative complications.
Keywords
Introduction
Cancer is the third most common cause of death in Malaysia. Cancer and its related therapy may lead to malnutrition through changes in metabolic response of the host, with increased protein catabolism, degradation of muscle and increased lipid oxidation. 1 Malnutrition among hospitalized patient is often overlooked. Less attention is given to the nutritional status of cancer patients as clinical management mainly focuses on surgical and oncological treatment only.
About 85% of cancer patients are unknowingly affected with malnutrition. Malnutrition is determined using several methods including serologic laboratory markers, anthropometric measurement and standardized nutritional scoring systems. The aim of nutritional screening is to distinguish patients who are already malnourished from those predisposed to malnutrition and offer early intervention. A study by Cross et al. in 2014 recommended the screening of patients undergoing orthopaedic surgery with evaluation of serum albumin levels and total lymphocyte count (TLC) and using standardized nutritional screening tools. They also suggested delaying surgery for malnourished patients until the malnutrition is addressed with proper early nutritional intervention. 2
Malnutrition is related to impaired wound healing with prolonged inflammation phase, reduced proliferation of fibroblast and collagen synthesis and angiogenesis. 3 Many studies have shown that malnourishment is associated with poor outcome for patients undergoing elective surgery, amputations and joint arthroplasty. Malnourishment is also associated with slow wound healing with persistent discharge, superficial and deep wound infection and wound breakdown. 4,5 Untreated malnutrition leads to cancer cachexia, which is characterized by depletion of lean body mass, muscle wasting and impaired immune, psychological and physical functions. Hence, early detection and intervention is the key to prevent post-operative morbidity and mortality. 6
Other than that, malnutrition is also postulated to cause increased post-operative infection, especially nosocomial infection, and is related to post-operative complications such as pneumonia, wound infection, acute renal failure and prolonged ventilator support. 7
A study by Hingorani et al. involving children with localized osteosarcoma reported that wound infection or slough was found in patients with low body mass index (BMI) at diagnosis. 8 Nonetheless, there is still lack of literatures reviewing nutritional status for orthopaedic oncology patients. Therefore, the objectives of this study were to determine the prevalence of malnutrition among orthopaedic oncology patients and the usefulness of three main malnutrition assessment methods including questionnaire scoring assessment, anthropometric and biochemical blood parameters in determining malnutrition and its relationship to post-operative complications.
Methodology
This study is approved by the hospital Medical Research Ethics Committee (MREC ID NO. 2017316-5056). It is a prospective observational study. Data collection was performed over a period of 18 months. Consent was obtained from all patients.
All orthopaedic oncology patients with malignant bone and soft tissue sarcoma or metastatic bone disease who were undergoing surgery were recruited. Three main methods of nutritional screening were conducted for the patients, 1 day before surgery consisting of nutritional assessment questionnaires, anthropometry measurements and biochemical blood tests.
At the moment, there is no standard routine practice of any nutritional assessment in our centre prior to surgery. This is the first time all patients received such nutritional evaluation 1 day prior to surgery. There is no delay of surgery despite having malnutrition detected.
Nutritional assessment questionnaires include Patient Generated Subjective Global Assessment (PG-SGA), Malnutrition Screening Tool (MST) and 3-minute Nutritional Screening (3MinNS) tools, all of which have been validated. PG-SGA group A refers to normal nutritional status, group B refers to moderately malnourished and group C refers to severely malnourished. Anthropometric measurements include body weight, height and mid upper arm circumference (MUAC). MUAC was measured at midpoint between the tip of acromion process and the olecranon process of the upper arm, using measuring tape.
Preoperatively, the patients’ blood was drawn and subjected to a few assessments including full blood count, renal profile, coagulation profile and liver function test. TLC, serum albumin and haemoglobin levels were the biochemical nutritional markers analysed. Patients who were malnourished with serum albumin <35 g/L were started on oral high-protein diet post-operatively. Patients were then followed up for 3 months. Any post-operative complication within 3 months was documented.
The primary outcome for this study is the post-operative complication. Post-operative complications were grouped into infectious and non-infectious complications. Infectious complications include surgical site infection (SSI) further classified into superficial, deep and implant site infections, nosocomial sepsis, respiratory infection and bacteremia. Non-infectious complications include wound seroma and haematoma which resolved without any antibiotic treatment, cardiovascular events, respiratory problems other than infection, renal failure, deep vein thrombosis and others. The secondary outcomes include length of hospital stay and unplanned readmissions. The relationship between malnutrition with the primary and secondary outcomes was analysed separately using χ2 test and univariate and multivariate logistic regression analysis.
Results
A total of 85 patients were recruited into this study, consisting of 43 male and 42 female patients. The demographic data are listed in Table 1.
Demographic and main characteristics of the sample population.
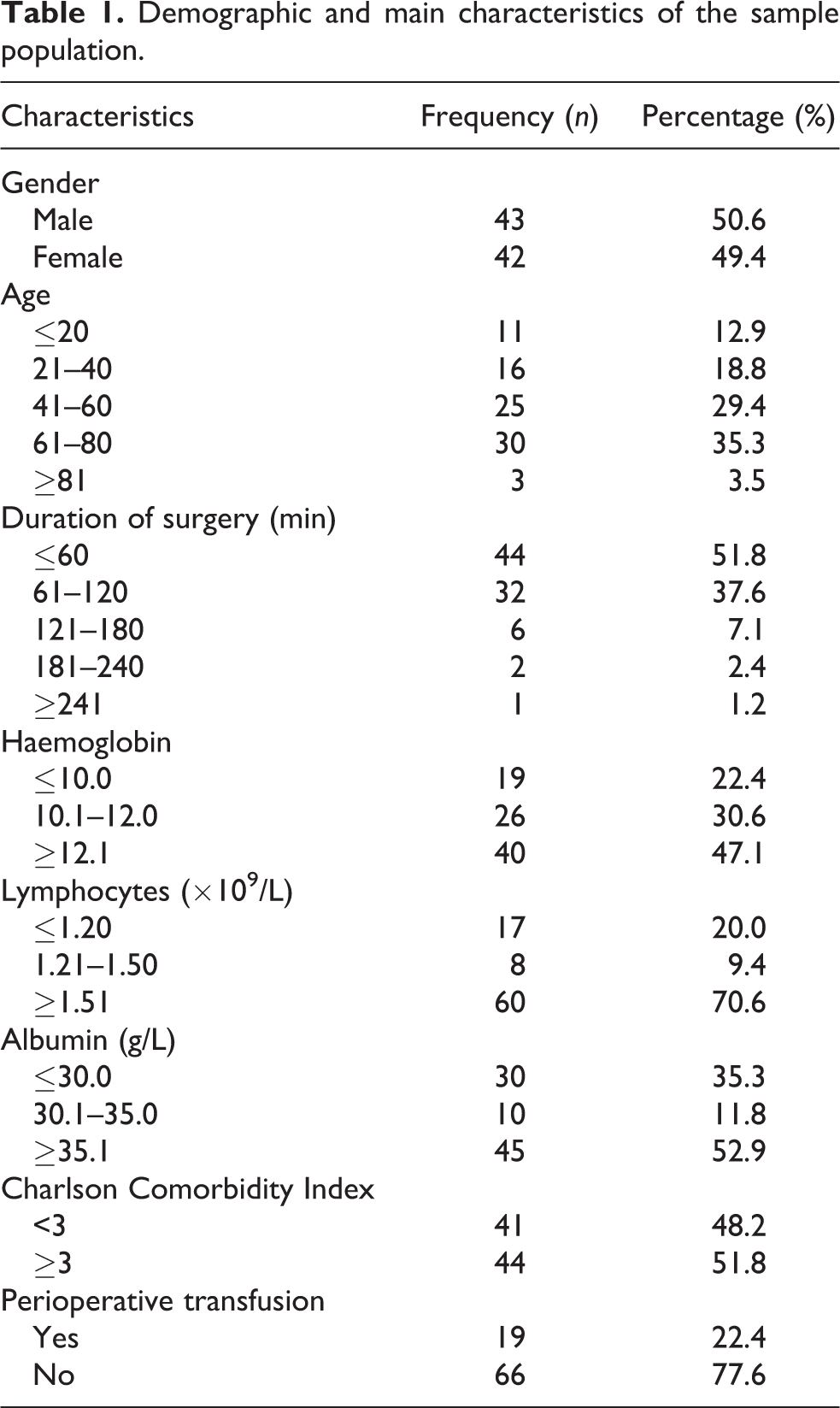
The prevalence of malnutrition was expressed as a function of a few different indicators including questionnaire scoring systems, anthropometric and quantitative biochemical blood parameters as listed in Table 1. Under PG-SGA scoring, the prevalence of malnutrition was at 45.88% compared to 3MinNS and MST scorings which rated it at 23.53% and 29.41%, respectively. The prevalence under anthropometric methods, namely, BMI and MUAC, was at 13.33% and 15.29%, respectively. The albumin levels represented the highest percentage of prevalence at 44.71%. Overall, the prevalence of malnutrition in our sample population ranged from 13.33% to 45.88% using different screening tools.
Seventeen (20%) patients developed post-operative infectious complications and 13 patients (15.3%) had non-infectious-type complications. Table 2 presents that six patients had superficial SSI, three patients had deep SSI and two patients developed implant infection. All patients with SSI recovered except for one with implant infection who had to have the endoprosthesis removed.
Infectious complications among the patients who were malnourished.
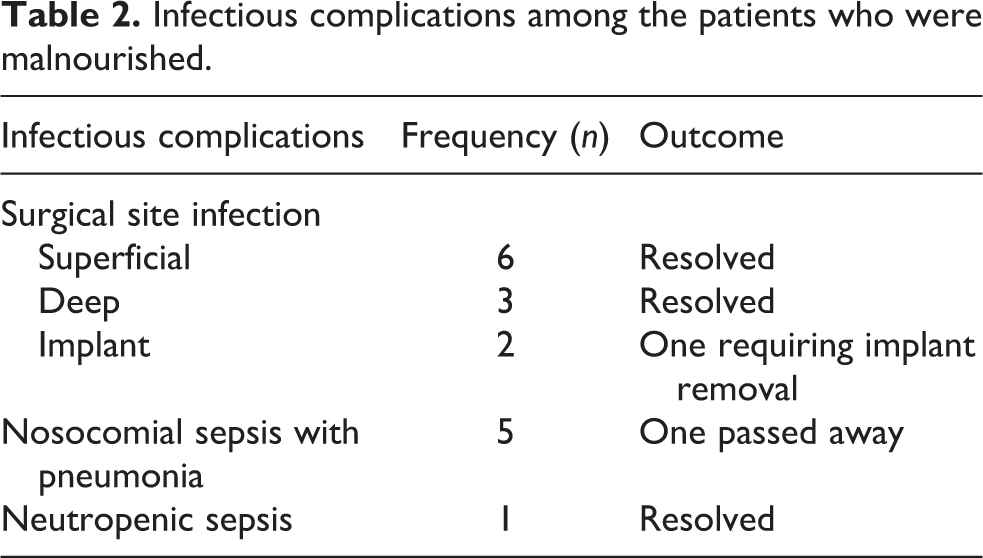
Five patients had nosocomial sepsis with pneumonia and one had neutropenic sepsis. The non-infectious complications are presented in Table 3, which include wound seroma, wound haematoma, cardiac arrest, pulmonary embolism, deep vein thrombosis, intensive-care unit (ICU) admission for hypovolaemic shock and multi-organ dysfunction, delirium and cement embolization syndrome. A total of six patients had both infectious and non-infectious complications.
Non-infectious complications among patients who were malnourished.

The relationship between malnutrition and post-operative complications was analysed using the χ2 test and logistic regression univariate and multivariate analysis.
Under the PG-SGA, MST and 3MinNS questionnaires, all three showed significant relationship between malnutrition and post-operative complications (p-value <0.001) as presented in Table 4. Univariate analysis showed that PG-SGA had the highest odds ratio (OR) of 13.75 compared to MST and 3MinNS at 2.59 and 1.69, respectively. Thus, PG-SGA seems to be the most predictive, showing 13 times higher risk of infectious complications compared to the normal group. For non-infectious post-operative complications, MST and 3MinNS questionnaires were more predictive with an OR of 3.42 and 1.85, respectively (p-value <0.001). However, malnutrition was not related to the non-infectious post-operative complications under PG-SGA, as presented in Table 5.
Distribution of infectious and non-infectious post-operative complications according to different nutritional parameters and main characteristics.a
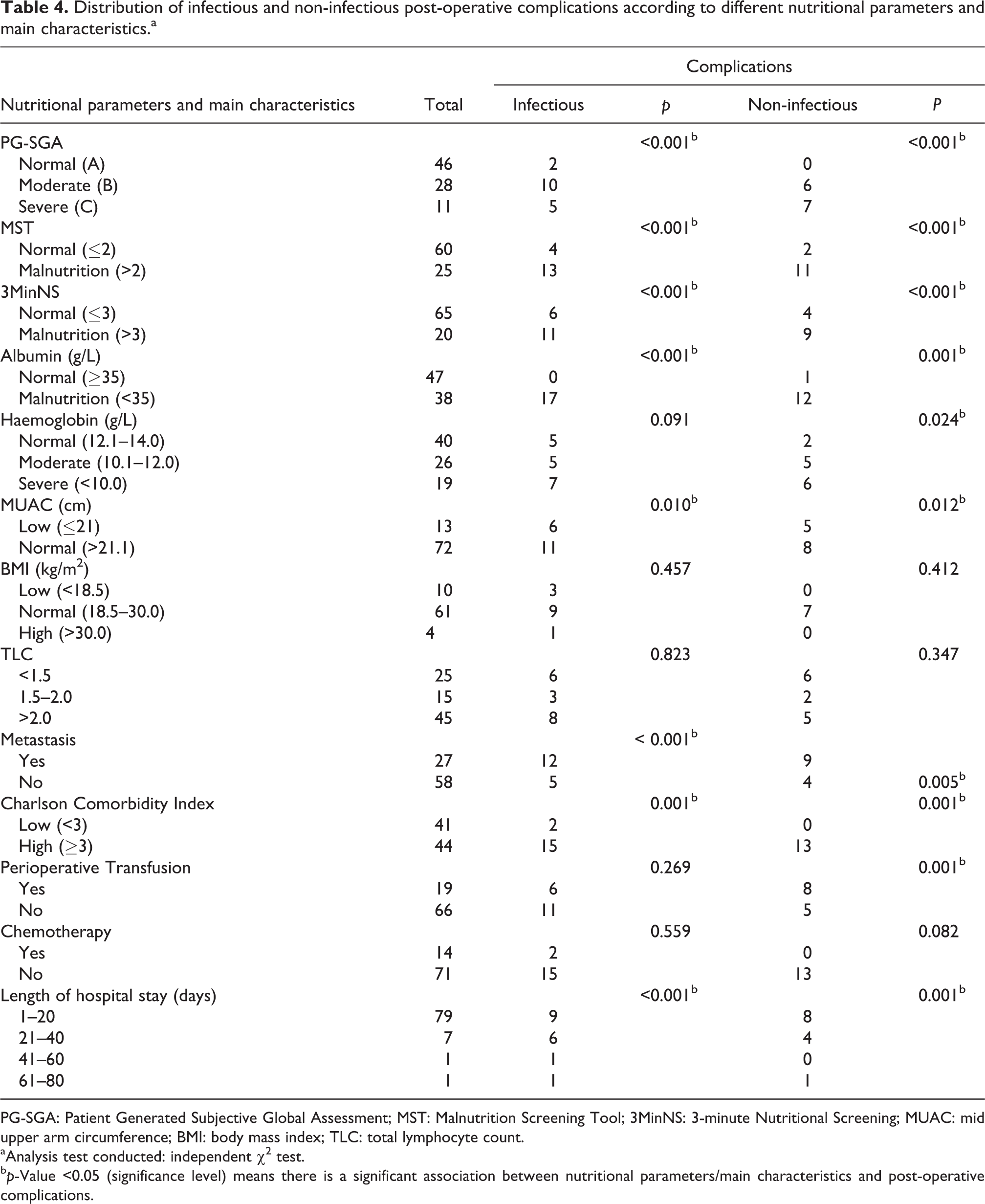
PG-SGA: Patient Generated Subjective Global Assessment; MST: Malnutrition Screening Tool; 3MinNS: 3-minute Nutritional Screening; MUAC: mid upper arm circumference; BMI: body mass index; TLC: total lymphocyte count.
aAnalysis test conducted: independent χ2 test.
b p-Value <0.05 (significance level) means there is a significant association between nutritional parameters/main characteristics and post-operative complications.
Univariate analysis of risk factors for post-operative complications.a

PG-SGA: Patient Generated Subjective Global Assessment; MST: Malnutrition Screening Tool; 3MinNS: 3-minute Nutritional Screening; MUAC: mid upper arm circumference; BMI: body mass index; TLC: total lymphocyte count; OR: odds ratio: CI: confidence interval.
aAnalysis test used: binary logistic regression.
b p-Value <0.05 (significance level): Risk factor contributed significantly to the occurrence of infectious/non-infectious outcome.
In the anthropometric method, there was significant relationship between low MUAC and post-operative complications (p-value <0.001) in infectious complications and non-infectious complications (p = 0.012). Low MUAC showed 4.75-folds risk for infectious complications and 5.00-folds risk for non-infectious complications in univariate analysis. In contrast, no significant relationship was demonstrated between low BMI and post-operative complications (75 of 85 patients’ data for BMI were available, while 10 patients’ body weight and height were not measured). Majority of patients with post-operative complications had a normal BMI.
Forty-seven patients had serum albumin levels of more than 35 g/L compared to 38 patients with albumin levels of less than 35 g/L. None of the patients with normal albumin levels had infectious complications and only one of them had non-infectious complication. Among those with hypoalbuminemia, 17 had infectious complications and 12 had non-infectious complications. Serum albumin level was significantly associated with post-operative complications as shown in Tables 4 and 5 (p-value <0.001). Univariate analysis shows an increase in a unit of albumin leads to the occurrence of infectious complication by 0.82-folds and non-infectious complication by 0.85-folds (p < 0.001). There was no significant relationship between post-operative complications and TLC. Lower preoperative haemoglobin level was weakly related to non-infectious complications (p = 0.024). However, it was not associated with any infectious complications.
Twelve of 27 patients with metastasis had infectious complications while 9 of them developed non-infectious complications. For those without metastasis, only five of them developed infectious complications while four of them had non-infectious complications. The presence of metastasis preoperatively was significantly linked with post-operative complications (p-value <0.001) for infectious complications and non-infectious complications (p = 0.005).
Patients were also classified into two groups using the Charlson Comorbidity Index (CCI). Fifteen post-operative complications were found in those with higher scores. Higher CCI was also significantly associated with post-operative complications (p < 0.001). Fourteen patients received neoadjuvant chemotherapy, while 71 patients did not. Chemotherapy itself had no relationship with post-operative complications (p > 0.05).
Multivariate analysis performed on the three questionnaires showed that 3MinNS was the most accurate among the three as presented in Table 6. 3MinNS values were significant (p < 0.001) with an OR of 1.69. For non-infectious complications, 3MinNS gave the only significant values with an OR of 1.50 (p = 0.019).
Multivariate analysis to compare the three questionnaire scoring tools in relationship to postoperative complications.

PG-SGA: Patient Generated Subjective Global Assessment; MST: Malnutrition Screening Tool; 3MinNS: 3-minute Nutritional Screening; OR: odds ratio: CI: confidence interval.
a p value < .05.
Multivariate analysis was also performed on the questionnaires, anthropometric and biochemical methods. 3MinNS showed to be significant in predicting both infectious and non-infectious complications, while serum albumin was the most predictive for infectious complications with a higher OR of 0.882 (p = 0.032). Hence, after multivariate analysis, 3MinNS and serum albumin were found to be the two most important methods for assessing relationship of nutritional status and post-operative complications (as shown in Table 7).
Multivariate analysis to compare three methods, that is, questionnaire scoring method, anthropometric method, biochemical method to assess nutritional status with relation to postoperative complications.
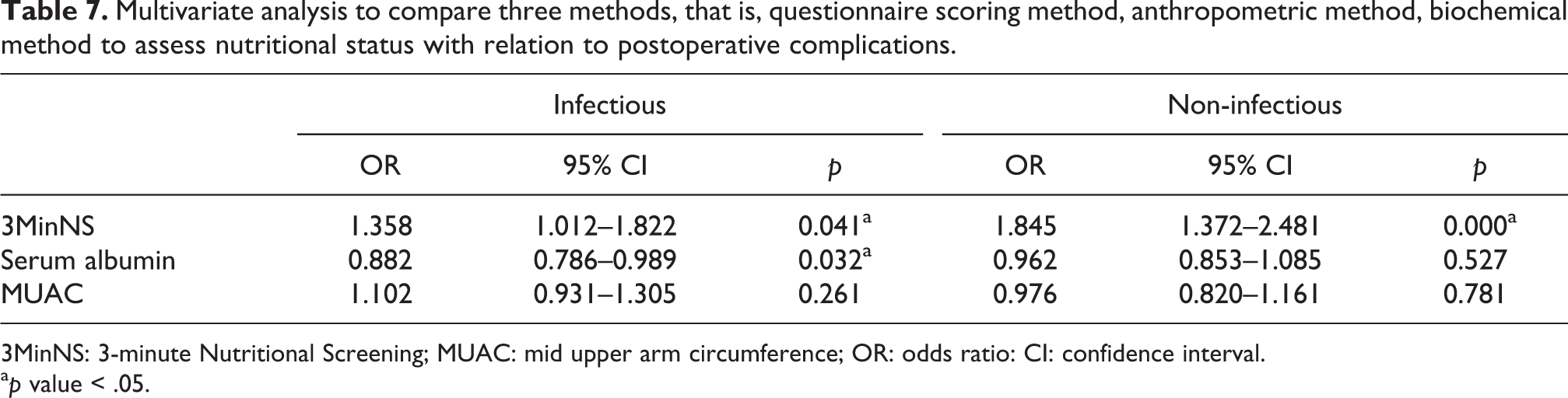
3MinNS: 3-minute Nutritional Screening; MUAC: mid upper arm circumference; OR: odds ratio: CI: confidence interval.
a p value < .05.
Analysis against other possible confounding variables showed that malnutrition was still the paramount factor in affecting surgical outcomes. Serum albumin levels and the presence of metastasis were significant in predicting infectious complications as presented in Table 8. Serum albumin level is more predictive of the two, with higher OR of 0.81 than the presence of metastasis with an OR of 0.11, although both were statistically significant. As for non-infectious complications, both 3MinNS and CCI were significant with OR of 1.53 and 1.37, respectively.
Multivariate analysis to compare significant nutritional parameters against other possible confounding variables in relation to postoperative complications.

3MinNS: 3-minute Nutritional Screening; OR: odds ratio: CI: confidence interval.
a p value < .05.
The secondary outcome in this study demonstrated that there was a significant increase in the risk of readmission for those who were malnourished with low albumin levels (OR: 6.98, confidence interval (CI): 1.407–34.633, p = 0.017). In addition, using albumin levels categorized as continuous data, the relationship between albumin level and length of stay was proved to be significantly associated with post-operative complications (OR: 0.88, CI: 0.798–0.968, p = 0.009). An increase in one unit of albumin leads to a drop in the odds of prolonged stay of more than 20 days.
Discussion
The role of malnutrition in affecting outcomes of orthopaedic surgery is widely described. 9 This is a first pilot study among patients with soft tissue and bone sarcoma of upper and lower extremities. Multiple factors leading to malnutrition, which act in isolation or in tandem include inadequate intake, increased energy and protein requirement and continuing losses. 5,10 European Society for Parenteral and Enteral Nutrition has published a guideline on diagnosis and management of nutrition of cancer patients. 11
Patients with sarcoma of the limbs are able to feed themselves and rarely have digestive complications, therefore nutritional intake should not be an issue. From our observation, the deterioration of nutritional status was mostly due to the anorexic and cachexic effects of the tumours itself. Cancer cachexia is postulated to occur via few mechanisms. The first is the pro-inflammatory cytokines produced which causes alteration in protein, fat and glucose metabolism, leading to insufficient utilization of the substrates. 12 Proteolysis inducing factor and lipid mobilizing factor have also been discussed in various studies for the pathophysiology of cancer cachexia. 1,6,13,14 The second mechanism is the excessive use of nutrients by the tumour cells for active replication, which leads to depletion of reserves. The third mechanism is the reduction in food intake which could be related to the anorexic signals induced by the tumours.
Other than the pathological factors above, socio-economic and hospital factors may also cause deterioration in nutritional status. Socio-economic factors include patients’ single status, poor family support and insufficient income. As for hospital factor, a study by Kondrup et al. reported multiple underlying causes for insufficient hospital care influencing nutritional status, including lack of instructions to tackle with it, lack of basic knowledge, patient-related aspects and food provision system. 5,15
Nutritional assessment is not a routine and compulsory practice in our centre. All patients did not receive any nutritional intervention since diagnosis was made due to lack of awareness of its importance. This study aims to determine a reliable indicator of malnutrition and justify the need to intervention.
Assessment of nutrition is frequently overlooked by surgeon and nurses. There are multiple methods to assess nutritional status among cancer patients including questionnaires, quantitative biochemical methods and anthropometric measurements. Simple, convenient and reproducible screening tools would be useful for health personnel who are busy with multiple tasks at hand. In addition to the catabolic effects, patients tend to wear down during long investigations, referral and treatment processes before surgery. A new concept of ‘parallel pathway’ emphasizes on early detection and intervention of nutritional deficiency while waiting for metabolic workup to delay the onset of cachexia. 16 Malnutrition could also affect performance status, immune functions, muscle functions, quality of life and mortality. 17,18 Proper management of nutritional status would reduce treatment cost as shown in a nutritional intervention program with its budget impact in United States. 19
The advantages of using questionnaire scoring tools include the ability to measure outcome following nutritional intervention, detect subtle changes through serial measurement and allow prioritization of patients for nutritional support.
The Oncology Nutrition Dietetic Practice Group of the American Dietetic Association has accepted the use of PG-SGA as the standard for assessment of nutritional status among patients with cancer. 20 Our result showed patients in malnourished group (PG-SGA group B and C) were 13.75-folds at higher risk of post-operative infectious complications based on univariate analysis. This finding corresponds with a 3-month multicentre prospective observational study done in nine French cancer centres by Antoun et al. They reported that malnourished patients were linked with major infectious and non-infectious complications (p = 0.04) and prolonged duration of stay (p < 0.001). 21
The overall results show that PG-SGA and 3MinNS are both effective in univariate analysis with 3MinNS having better significance in multivariate analysis. 3MinNS scoring tool is simple, quick and concise with summative scores and cut-off points for subsequent actions. It includes shorter history and physical examination and easier to be practised by anyone who had basic medical knowledge. We advise the use of 3MinNS in a busy clinic setting where patients can be screened quickly and yet effectively. As for PG-SGA, it involved more detailed history and physical examination and required longer time to complete the assessment. Hence, we suggest its use only in ward setting where patient can be assessed by experienced and trained personnel within a conducive time and space that allows longer interaction. The use of any of the above two questionnaires would be beneficial in optimizing nutritional status of orthopaedic oncology patients.
Next, in anthropometric method, our result showed that MUAC was also significant in predicting post-operative complications. We recommend the use of MUAC as it can be easily measured, convenient and reproducible. The loss of muscle is a gradual process and might not manifest early in the course of disease. It should be used in combination with questionnaire tools or biochemical marker serum albumin. MUAC was shown to correlate positively and significantly with BMI in a previous study but this does not concur with our findings. 22 There is no significant link between BMI and post-operative complications in this study. BMI is not practical as it is not measurable in bedridden patient secondary to fracture or generalized malaise and can be affected by tissue oedema. However, this is contradicted by a study by Hingorani et al. where BMI was shown to be associated with wound infection after surgery. 8
Lastly, we had shown the significance of biochemical marker serum albumin in predicting post-operative complications, length of stay and unplanned readmission. From the multivariate analysis, serum albumin is the sole factor related to infectious complications with an OR of 0.81. A meta-analysis review involving 25 observational studies reported at least 2.5-folds risk of SSI in orthopaedic surgery or arthroplasty patients with low albumin levels of less than 35 g/L. 23 A study in Mahidol University Thailand showed that 29% of patients with hypoalbuminemia developed post-operative complications and none of those with normal albumin levels had any complications. 24 Hu et al. found that hypoalbuminemia <35 g/L was significant with the highest coefficient in multivariate analysis linked to post-operative mortality. 25 We recommend routine use of serum albumin together with questionnaire tools in every oncology patients. Serum albumin is the easiest and best objective way which can detect and monitor the trend of nutritional profile before and after surgery.
The use of TLC combined with albumin levels to predict post-operative outcomes has been studied by Greene et al. 26 However, we could not demonstrate any significant results with the TLC as shown in a few studies. Kuzuya et al. reported the lack of relationship between TLC and nutritional status among the elder population in their study. 27
Length of stay is a surrogate marker for patients’ general well-being during admission. Prolonged admission could lead to many problems including increased cost of treatment, delayed return to work, nosocomial infection and psychological issues such as depression. 28,29 In a systematic review, Gupta et al. discussed the role of nutritional status on the length of stay. Any drop in a unit of serum albumin level in this review was associated with prolonged hospital stay of more than 20 days. Our results had shown significant relationship between length of stay and unplanned ICU admissions with low serum albumin level as other studies 29 –31
There are few mechanisms explaining pathophysiology of malnutrition and infection. First is the lack of protein substrate which causes poor angiogenesis and delayed wound healing. Second would be the lack of oxygenation from pulmonary oedema secondary to hypoalbuminemia and third space fluid loss. Third is a possible defect in host defence mechanism with decreased number of natural killer cells and complement proteins. 3,32
SSI is the most dreaded complication in any orthopaedic surgery. Eleven of 17 infectious complications in this study are SSIs. From the univariate analysis, malnutrition was significantly associated increased risk of infectious complications using the 3MinNS questionnaire (OR: 1.69), MUAC (OR: 4.75) and serum albumin (OR: 0.82). Many publications related to arthroplasty field have shown the relationship of malnutrition with post-operative infection. 26,33,34 Yi et al. found 7% infection rate in patients having one or more parameters of malnutrition versus only 1% in those who were normal. 35 Persistent wound drainage was more commonly seen in malnourished patients leading to deep infection later. 34 Malnutrition was also shown in other oncology fields such as gynaecological cancer and gastrointestinal cancers to be related to infectious complications. 36 –40
The non-infectious complications refer to post-operative events or complications which arise primarily or secondary to the tumour itself. In this study, it includes deep vein thrombosis, pleural effusion, pulmonary embolism, wound seroma or haematoma where regular aspiration was performed without antibiotic coverage, liver transaminitis, ICU admission, non-organic cause post-operative delirium and bone cement embolization syndrome. Our results showed significant relationship between malnutrition and non-infectious post-operative complications. This is concurrent with results from other studies. 37,41
There were few limitations to this study. Firstly, the heterogeneity of the sarcoma types may have different sizes and clinical behaviour leading to different types of surgery being performed. Next, patient with secondary metastatic bone disease may have different clinical course and treatment response based on its primary. Other confounding variables in our data which could affect post-operative complications include chemotherapy and perioperative transfusions. However, our results had shown no significant relationship for chemotherapy factor. This might be due to different types of chemotherapy regime given to only small numbers of patients. We suggest separate larger study on this chemotherapy factor alone which might give different results. Perioperative transfusion was associated with post-operative non-infectious complication from univariate analysis in this study. Multiple level II and level III studies in spine surgery, fracture surgery and arthroplasty had shown increased infective complications with perioperative transfusion. 42 Morris et al. reported blood transfusion was related to wound infection among patients with lower extremity oncology surgery. 43 Exact mechanism remains unclear. Blumberg and Heal reported immuomodulation effects with increase in CD8 cells and decrease in macrophages and natural killer cells’ function after transfusion. This shift may impair the innate and cellular immune response and increase susceptibility to infection. 44
Also, the presence of metastasis and higher CCI are both shown to increase the likelihood of post-operative complications in logistic regression analysis. Patients with metastasis are usually in late stages of the disease and appeared frail and immunocompromised after succumbing to the chronic catabolic effects of tumour burden and related chemoradiotherapy. Therefore, these patients are generally nutrition depleted and prone to develop post-operative complications. A further study with larger samples shall be conducted to stratify the patients into different groups. Nonetheless, nutritional status remains the most important factor among all after multivariate analysis as shown in Table 8. Similar results were also reported by Huang et al., where comorbidities was itself a confounding factor, but malnutrition was still the main predictive factor in post-operative complications after multivariate regression analysis. 41 Chemotherapy with its side effects also leads to malnutrition among patients. However, the use of chemotherapy as neoadjuvant therapy was not significantly related to any post-operative complications. With the significant relationship being shown between malnutrition and post-operative complications, we had since raised awareness among the healthcare personnel about the importance of early detection, prevention and intervention for this group of patients.
Conclusion
Malnutrition is common among orthopaedic oncology patients and has a significant relationship with post-operative infectious and non-infectious complications. It is therefore important for surgeon to initiate an early screening program by the combination of methods to improve nutritional status which itself is a modifiable factor. Ideal preoperative evaluation methods analysed from this study are 3MinNS or PG-SGA questionnaires, MUAC and serum albumin level.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.