
Abstract
The quadrilateral space is bounded by the teres minor superiorly, the teres major inferiorly, the long head of the triceps medially and the shaft of the humerus laterally. The axillary nerve and posterior circumflex humeral artery pass through this space to enter the posterior compartment of the upper arm. Quadrilateral space syndrome (QSS) is caused by entrapment of the axillary nerve or its main branches and/or the posterior circumflex humeral artery in the quadrilateral space by internal or external compression. QSS can often be difficult to diagnose, given that patients may present with non-specific symptoms. As such, patients may be misdiagnosed with more common disorders of the shoulder. We report a case of QSS masquerading initially as rotator cuff pathology with positive impingement signs.
Introduction
The quadrilateral space is bounded by the teres minor superiorly, the teres major inferiorly, the long head of the triceps medially and the shaft of the humerus laterally. Compression or obliteration of this space entraps the axillary nerve, and posterior circumflex humeral artery gives rise to a constellation of clinical signs and symptoms called quadrilateral space syndrome (QSS). 1 QSS can often be difficult to diagnose, given that patients may present with non-specific symptoms. As such, patients may be misdiagnosed with more common disorders of the shoulder. We present such a case, in which a patient with QSS presented with signs and symptoms mimicking a rotator cuff tendinopathy.
Case report
A 48-year-old salesman without any significant medical or surgical history presented to us with a history of left shoulder pain for 2 months in the non-dominant arm without history of trauma. There were no swellings, skin redness or muscle atrophy of the left shoulder. Active abduction was limited by pain, but passive global range of motion (ROM) was full. Abduction, internal and external rotation were generally weaker at Medical Research Council (MRC) grade 4 attributable to pain coupled with positive subacromial impingement test. Plain radiograph of the left shoulder was normal. The clinical diagnosis was that of a rotator cuff tendinopathy with a possible tear. A subacromial injection of steroid and local anaesthetic was given to the patient, which resulted in good relief of the pain. He was started on a structured physiotherapy program consisting of rotator cuff strengthening and periscapular stabilization exercises.
At the repeat visit 2 months later, the patient’s pain resolved with good active ROM. However, he complained of weakness of the left shoulder. Clinical examination revealed mild deltoid muscle atrophy and persistent weakness of abduction and external rotation at MRC grade 4. Following this, a magnetic resonance imaging (MRI) scan was performed and this showed only mild insertional tendinosis of the distal supraspinatus tendon with no tears and mild subacromial bursitis. However, there were significant findings of deltoid muscle oedema with fatty infiltration and atrophy of the teres minor noted in the scan (Figures 1 and 2). No focal lesions, paralabral cyst or aneurysm were seen in the quadrilateral space (Figure 3). At this time, QSS becomes the main differential diagnosis.

Axial cut from the MRI of the left shoulder with the black arrow showing the deltoid muscle atrophy with fatty infiltrations. MRI: magnetic resonance imaging.

Sagittal cut from the MRI of the left shoulder with the black arrow showing the teres minor muscle atrophy with fatty infiltrations. MRI: magnetic resonance imaging.
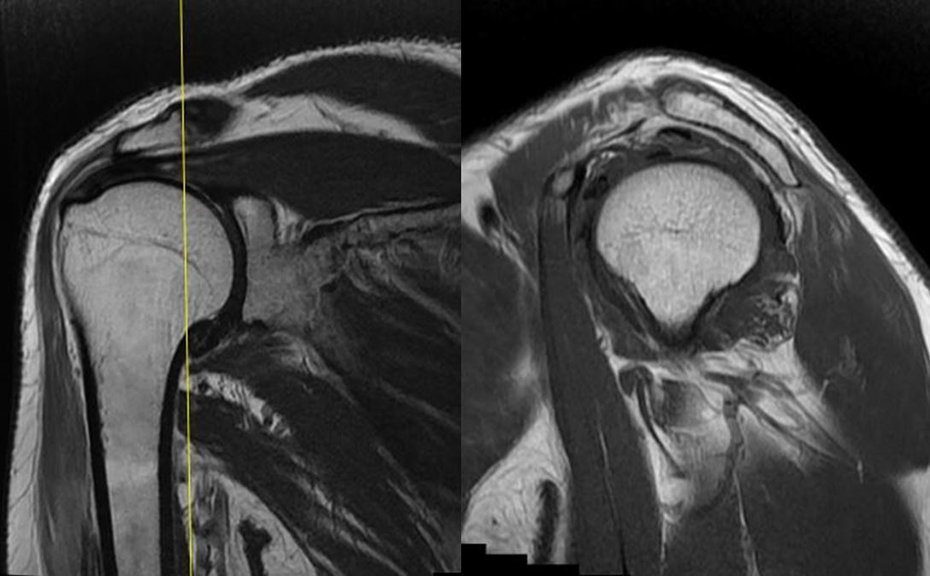
Coronal and sagittal cut from the MRI of the left shoulder showing the quadrilateral space of the shoulder with no obvious focal lesions in the space causing compressive effect. The atrophy of deltoid on coronal cut and teres minor on sagittal cut of the MRI films can be appreciated here as well. MRI: magnetic resonance imaging.
Follow-up studies with nerve conduction study (NCS) showed left axillary neuropathy, and electromyography (EMG) showed active denervation potentials from the deltoid and teres minor. There were no denervation signals from other muscles of the C5 myotome. Ultrasound showed fasciculations from the teres minor muscle and disturbed the architecture of the deltoid muscle. At this juncture, clinical findings aided by imaging and nerve tests confirmed that the patient was suffering from left shoulder QSS.
The patient was treated conservatively with physiotherapy with a view for surgical decompression should the QSS not respond to conservative care or progressively worsening. The prescribed physiotherapy treatment emphasizes on internal mobilization of the humerus, stretching into horizontal adduction and internal rotation and posterior rotator cuff strengthening with soft tissue massage techniques to the quadrilateral space. 2,3 He returned at 3 months (6 months post-index review) with no pain but mild aches when lying on the left shoulder. He was able to perform his activities of daily living well without pain despite the persistent weakness. Clinically the deltoid was wasted (Figure 4), deltoid and teres minor power were weak at MRC grade 4 although ROM was full and painless. He chose to continue physiotherapy with close monitoring. At his latest follow-up 1 year later, the left shoulder remained the same with persistent deltoid (abduction) weakness and teres minor (external rotation in 90° abduction) weakness of MRC grade 4. He had compensated well and does not have any pain in performing his work and activities of daily living.

Posterior view of the patient with obvious wasting of the left shoulder deltoid muscle.
Discussion
QSS was first described in 1983 by Cahill and Palmer in a series of 18 patients. 1 They described a collective symptomology of gradual and atraumatic onset of pain and paraesthesia, aggravated by flexion and external rotation of the humerus from the compression of the neurovascular bundle in the quadrilateral space. They highlighted the difficulty in diagnosis of this condition, given the atypical symptoms. 1 Good results were reported with surgical management, provided a conclusive diagnosis was reached. Following that, sporadic case reports ensued describing the various causes and presenting symptoms of QSS highlighting the difficulties in reaching a conclusive diagnosis. 2 –9 We report a case of QSS masquerading initially as rotator cuff pathology with positive impingement signs.
Clinical diagnosis of QSS is difficult to make because of the vague presenting complaint of shoulder pain coupled with shoulder weakness which is difficult to diagnose as deltoid and teres minor weakness can be masked by surrounding muscle groups that compensate for their function. It is reported to be commonly associated with patients aged 20–40 years and typically involving the dominant shoulder. 10 Several causes for internal compression within the quadrilateral space have been previously identified such as aneurysm, schwannoma and fibrous bands. 1 –9,11 More common external compression causes include hypertrophied muscular boundaries, paralabral cysts, ganglion cyst and less common mechanical causes, such as an osteochondroma and a bony spike from malunion of a previous scapular fracture. 1 –9,11 Compression may also be functional, with compression of the neurovascular structures in abduction and external rotation. 1,11 Treatment is usually non-surgical initially with symptomatic care, physical therapy and change of lifestyle. Patients with persistent symptoms not responding to conservative care or competitive athletes should then be offered surgical decompression as surgical results have been shown to yield positive outcomes. 1,11
This case was interesting for two reasons. First, the initial presentation of QSS “masqueraded” as rotator cuff tendinopathy. The second point of interest was the resolution of the rotator cuff tendinopathy leading to further investigations of the persistent weakness of shoulder.
The classic approach to differential diagnoses of shoulder pain is to classify possible causes according to the main common categories of impingement and rotator cuff pathologies, acromioclavicular joint pathologies, shoulder joint instability and degenerative conditions. However, it is not unusual for patients to have more than one contributing factors such as rotator cuff tear and acromioclavicular joint arthritis. Typically, the presenting clinical picture guides the clinician’s diagnostic and management strategies. This case illustrates the importance of being vigilant for other clinical features suggestive of a different contributing pathology. For example, while it was easy to attribute the shoulder weakness to pain from rotator cuff tendinopathy, these features were, in retrospect, a telltale sign for muscle weakness from axillary neuropathy. In this particular case, the authors resolved this issue by injection of steroid and local anaesthetic to alleviate the pain from rotator cuff tendinopathy. Nonetheless, it is also prudent to mentally run through all the possible causes of left shoulder weakness and try to localize the lesion to correlate with diagnosis even when it appears obvious. A meticulous clinical examination of the shoulder such as the finding of deltoid muscle atrophy however subtle can also assist in providing clues to the diagnosis of QSS.
The second point of interest is the investigation of the persistent shoulder weakness. Often, imaging studies such as X-ray and MRI are needed with aid from NCS to diagnose QSS. X-ray of the shoulder would be able to illustrate any joint or bony abnormalities such as fracture spikes or osteochondroma that can cause compression of the quadrilateral space. 4,5 In addition, MRI scan can evaluate the presence of soft tissue space occupying lesions such as paralabral cyst, aneurysm, neuroma, tumour or hypertrophied muscular boundaries. 1 –3,6 –9,11 Most importantly, by having the differential diagnosis of QSS in mind, the physician incharge can also specify to the radiologist to look out for pathologies at the quadrilateral space to improve sensitivity. Had it been just an ultrasound scan of the shoulder for rotator cuff pathology, the diagnosis of QSS may have been missed. Following that, NCS and EMG can help with identifying axillary neuropathy and ruling out C5 and/or C6 radiculopathy because axillary nerve arises from the C5 and C6 nerve roots. 2,11 Therefore, physicians should always be cognizant of QSS as a differential diagnosis.
Other differential diagnosis for QSS is broad and includes thoracic outlet syndrome, referred pain from cervical radiculopathy, brachial neuritis or plexopathy and suprascapular nerve injury on top of the usual shoulder differential diagnoses as mentioned above. 11 As described by McAdams and Dillingham in 2008, 12 their algorithm for assessment of patients with posterior shoulder pain includes thorough history taking and physical examination followed by physical therapy programme for common causes of posterior shoulder pain. If the pain does not abate in 6 months of physical therapy, MRI of the shoulder was obtained. A lidocaine block test was performed if the MRI did not show clear anatomical source of the pain. This QS lidocaine block test can be done with or without ultrasound guidance and if positive warrants further evaluation of the QSS with EMG and computerized tomography angiogram. We concur with the suggested assessment algorithm 12 with a few modifications as in the proposed diagnostic algorithm flow chart (Figure 5).

Diagnostic algorithm flow chart. Patients are first screened via history and clinical examination followed by treatment with physical therapy versus MRI scan of the shoulder. If MRI scan is not diagnostic, the investigation of choice would be NCS/EMG or CT angiogram. If results are not diagnostic or equivocal, a QS lidocaine block can be performed with or without ultrasound guidance. MRI: magnetic resonance imaging; NCS: nerve conduction study; EMG: electromyography; CT: computerized tomography; QS: quadrilateral space.
In summary, we describe a case of QSS masquerading initially as rotator cuff tendinopathy. We hope that this case report will remind clinicians to be vigilant of other differential diagnoses even when the cause seems apparent.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.