
Abstract
Background:
Orthopedic surgeons routinely obtain informed consent prior to surgery. Legally adequate informed consent necessitates a thorough discussion of treatment options and risks and proper documentation. However, the quality of informed consent in orthopedic trauma patients is an under-researched area.
Purpose:
To assess the quality of the informed consent process in trauma compared with elective orthopedic patients and to assess patients’ emotional state at the time of signing consent form.
Methods:
Sixty-two consecutive patients undergoing either elective total joint arthroplasty (N = 32) or orthopedic trauma surgery (N = 30) were included. The data were collected through personal interviews using a proposed informed consent score. The interviews were held after obtaining the informed consent and before the index procedure. Patients were asked to describe their diagnosis, the surgical procedure, its’ benefits, and risks as well as alternative treatments.
Results:
Mean age differed significantly between elective and trauma group patients (66.1 vs. 51.6, respectively, p < 0.01), while gender and education level were comparable (p = 0.075, p = 0.55, respectively). The quality of consent was significantly better for patients with post-high-school education compared to elementary education level (consent score: 16.9 ± 4.1 vs. 12.2 ± 5.5, p = 0.021). Patients in the elective group showed an overall higher quality of consent, as reflected by a mean score of 17.03 ± 4.2 versus a mean score of only 13.73 ± 4.7 in the trauma group (p = 0.005, 95% CI: 1.02–5.57). Specifically, trauma patients demonstrated a lower comprehension of the diagnosis, the benefits of surgical treatment, the possible complications, and the expected postoperative course.
Conclusion:
Patients undergoing trauma surgery are significantly more likely to have an inadequate understanding of the proposed treatment. These findings raise questions concerning the validity of consent from trauma patients.
Background
Informed decision-making is the process by which physicians foster the informed participation of patients in clinical decision-making. This process embodies the communication between surgeon and patient in which the patient learns of the risks and benefits of a proposed procedure and decides whether to proceed. 1 –3 Physicians are responsible to effectively communicate and encourage their patients to participate in decision-making, creating a two-way flow of information between patient and physician.4 While orthopedic surgeons obtain informed consent on a regular basis, there is very little data to guide them regarding effective methods of obtaining and documenting this essential communication. 5
There is little published evidence about patients’ experience of the consent process, and, in particular, there is little evidence that distinguishes between the experiences of patients who have undergone elective compared with trauma surgery. Given the increasing array of therapeutic interventions available in orthopedic trauma surgery and the increase in medicolegal activity relating to acute surgery, the process of informed consent in this setting assumes increasing importance.
In patients undergoing surgery for traumatic injury, the process of informed decision-making may be compromised by the fact that the individual is experiencing acute pain and psychological distress, or conversely is under the effect of analgesia or sedation. 6 Sometimes, there is also the need to intervene rapidly, leaving the patient without adequate time to deliberate. The nature of urgent surgery makes objective evaluation of the informed consent process difficult. 7 In contrast to trauma surgery, in elective arthroplasty surgery, the process starts with the referring practitioner, is developed through the first consultation with the surgical team, and continues until the surgical procedure begins. 8 In many departments, this process is also reinforced by consultation with supporting staff such as nurses and physical therapists, as part of the preparation process for surgery. The informed consent in these patients is, therefore, not a single event but a process leading to a fuller understanding of the intended procedure and its attendant benefits and risks. 9 It also seems logical that the physician–patient communication that occurs in the office, possibly with an already familiar surgeon, is more interactive and substantive than discussions that occur on the hospital floor, the emergency room, or in the preoperative holding area. 5 In a study comparing between emergent to elective gynecological procedures,10 patients undergoing emergent procedures were significantly less likely to remember signing a consent form and reported being in pain, drugged, desperate, tired, or unwell when asked to sign the consent form. These patients were significantly less likely to report satisfaction with the consent process than elective patients.
We designed a prospective cohort study based on personal interviews to assess the quality of the informed consent process in trauma compared with elective orthopedic patients as well as the patients’ emotional state at the time of signing consent form, focusing on competent adults. Our hypothesis was that elective patients have a fuller understanding of the intended procedure and its benefits and risks, leading to an informed consent process of higher quality when compared to trauma patients.
Materials and methods
Study design
This prospective observational study was conducted at Rabin Medical Center, Orthopedic Department over a 2-year period. Institutional review board approval was granted.
Patient population and setting
The subjects were of two distinct groups. The first included elective patients planned for a joint replacement surgery [primary THA (total hip arthroplasty) or primary TKA (total knee arthroplasty)]. The second group included patients who arrived at the emergency department and were diagnosed with a traumatic injury of the extremities, either a fracture or a tendon injury, and subsequently admitted for surgical treatment, to the same orthopedic department. Of note, informed consent for the surgery was obtained by the same group of department physicians, for both groups. For trauma patients, informed consent for surgery was obtained upon arrival to the hospital as soon as the diagnosis was made in the emergency department. For elective patients, consent was obtained in the pre-operative assessment clinic, held at a mean interval of 27.4 ± 4 days before the planned surgery. In both groups, the provider evaluating each patient discussed the proposed procedure and informed the patient on three main areas, that is, basic operative information, post-operative management, and possible complications. Patients provided informed consent at the end of the encounter after all questions were answered and signed consent forms.
The patients were recruited to the study at the department already after giving consent for surgical treatment. The interviewers (SS, RD, and ES) were physicians who did not have a previous discussion with the patient with regards to the surgery, were not the consent obtainers, and had no involvement in the delivery of care. The interviews were held in the time frame between giving the consent and the actual surgery and no longer than 7 days from signing the consent form. Patients’ capacity to consent for treatment and decision when to seek substituted consent was determined by the physician obtaining the consent. Patients were excluded if they were found to be incompetent to give consent or if they had one of the following: age younger than 18 years, sustained a concurrent head injury, involved in polytrauma requiring multiple procedures, Glasgow Coma Score of less than 15. The predetermined target sample size population was 60 patients, to give sufficient power to the study (power of 80% for detecting a difference of three points in the total consent score, at the 0.05 level). A total of 70 patients, able to give their own consent, were seen in the emergency room or the arthroplasty outpatient clinic during a 4 months period and then subsequently admitted for operation.
Of the 70 patients who met the inclusion criteria, 5 declined participation and 3 chose to be operated elsewhere. Thus, a total of 62 patients were finally enrolled in the study.
Structured interviews
Structured interviews were used to examine the completeness of informed decision-making as perceived by the patients. The initial survey was pilot tested on 15 consecutive patients to assess for completeness and comprehension. The interview included three segments: the first obtained basic demographics including the level of education, occupational status, living arrangements, and the level of independence.
The second and main part of the interview was designed to assess the patients’ understanding of their condition and possible treatments as well as the quality of informed consent fostered by the consent obtainer. Assessment of the informed decision-making process relied on the two key dimensions proposed by Braddock et al. 2 : providing information and fostering patient involvement. The questions were designed to explore most of the key elements in those two dimensions, as described by Braddock et al. in their informed-decision-making model. These included discussions of the nature of the decision, the patient’s role, alternatives, pros and cons, and uncertainties; the assessment of the patient’s understanding and his or her desire to receive input from others; and the exploration of the patient’s preferences and the impact on the patient’s daily life (Table 1). This comprised an 11-item list. A score of 0–2 was set for each item, based on the interviewer’s impression. If the required item for the relevant decision was thoroughly discussed and understood by the patient, it was determined satisfactory and received two points (the highest score). The item was labeled inadequate and received zero points if the element was not discussed or not understood by the patient. Partial understanding received one point.
ICS items.
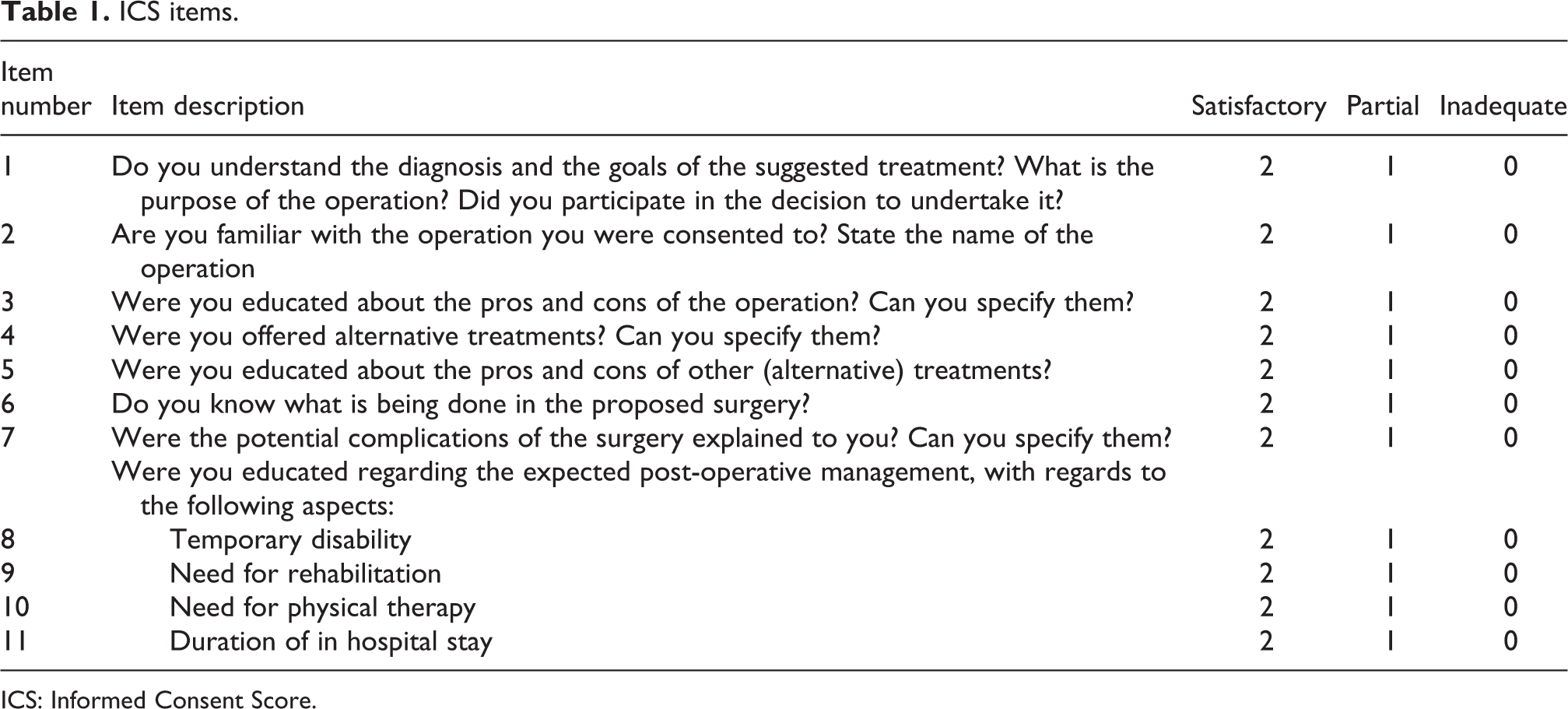
ICS: Informed Consent Score.
The third part included the Spielberger State-Trait Anxiety Inventory for Adults (STAI) questionnaire 11 to assess how the respondents feel about the upcoming surgery. The STAI questionnaire is a well-acknowledged instrument, measuring respectively transient and enduring levels of anxiety. The STAI questionnaire contains 20 items equally divided between positive and negative statements regarding anxiety. The range of possible scores varies from a minimum of 20 to a maximum of 80, the higher the score the higher the level of anxiety.
The interview was of approximately 20 min in duration and was conducted with the individual’s consent in all cases.
Statistical analysis
Descriptive analysis focused on the completeness of informed decision-making for each decision category. The score for each category was valued as 0 (inadequate), 1 (partial), or 2 (satisfactory). There were 11 items in total, thus the result was a score ranging from 0 to 22, with higher scores representing a more thorough understanding, and a better quality of consent conveyed to the participants. Validation of reliability of our 11-item score was assessed using Cronbach’s α, a measure of internal consistency. The overall reliability coefficient was found to be 0.828, which indicated a high level of internal consistency.
Quantitative data relating to demographics of patients in the trauma and elective surgery groups were compared by using Student’s t-test. Significance was accepted at the p < 0.05 level.
Categorical bivariate analysis was conducted using χ 2 and Fisher’s exact test, where appropriate. Continuous variables were analyzed using Student t-test or Mann–Whitney U test after testing for normality and equal variance. For variables with more than two subcategories, analysis of variance (ANOVA) was conducted to detect between groups differences. The Scheffe’s post hoc test was performed to test multiple differences of variables between groups. Multivariate analysis was carried out using three-way ANOVA.
Correlation of continuous variables was assessed using Pearson’s linear correlation. Values of p < 0.05 were regarded as significant. A multivariate linear regression model was constructed to establish the adjusted effect of the type of surgery (elective vs. trauma) on the informant consent scores.
Data were analyzed using the SPSS software V.20 (SPSS Inc, Chicago, Illinois, USA).
Results
Of the 62 patients enrolled in the study, 32 patients were included in the elective surgery group and 30 in the trauma surgery group.
The elective surgery group consisted of patients undergoing total knee arthroplasty (n = 13) and total hip arthroplasty (n = 19). The trauma surgery group was more diverse and consisted mostly of a variety of fractures (n = 27) requiring open reduction and internal fixation (1 pelvic ring, 6 femoral neck, 5 distal radius, 6 ankle, 2 tibial plateau, 1 patella, 3 distal humerus, and 2 phalangeal) and tendon injuries requiring surgical repair (n = 3). Overall, there were 57 surgeries that were considered major, whereas 5 were considered minor and consisted of the phalangeal fractures and tendon injuries.
Of the entire cohort, 56.5% of patients were females. The mean age was 59.1 ± 16.5 years. The elective group’s patients were significantly older (66.3 ± 11.5 years (range 45–93 years) versus 51.4 ± 17.5 years (range 22–81 years), p < 0.001). Education level was diverse: 11 patients (17.7%) had elementary education, 26 (41.6%) had high-school education, and 25 (40.3%) were college graduates or above. However, the level of education was not different between the two study groups. Of the entire cohort, 20 patients (32.3%) were salaried employees, 7 (11.3%) were self-employed, 25 (40.3%) retired, and 10 (16.1%) were unemployed. The elective group had a significantly higher proportion of retirees when compared to the trauma group (59.3% vs. 20%, p < 0.001). Living circumstances did not differ significantly between the two groups (Table 2).
Baseline characteristics and between group analysis.
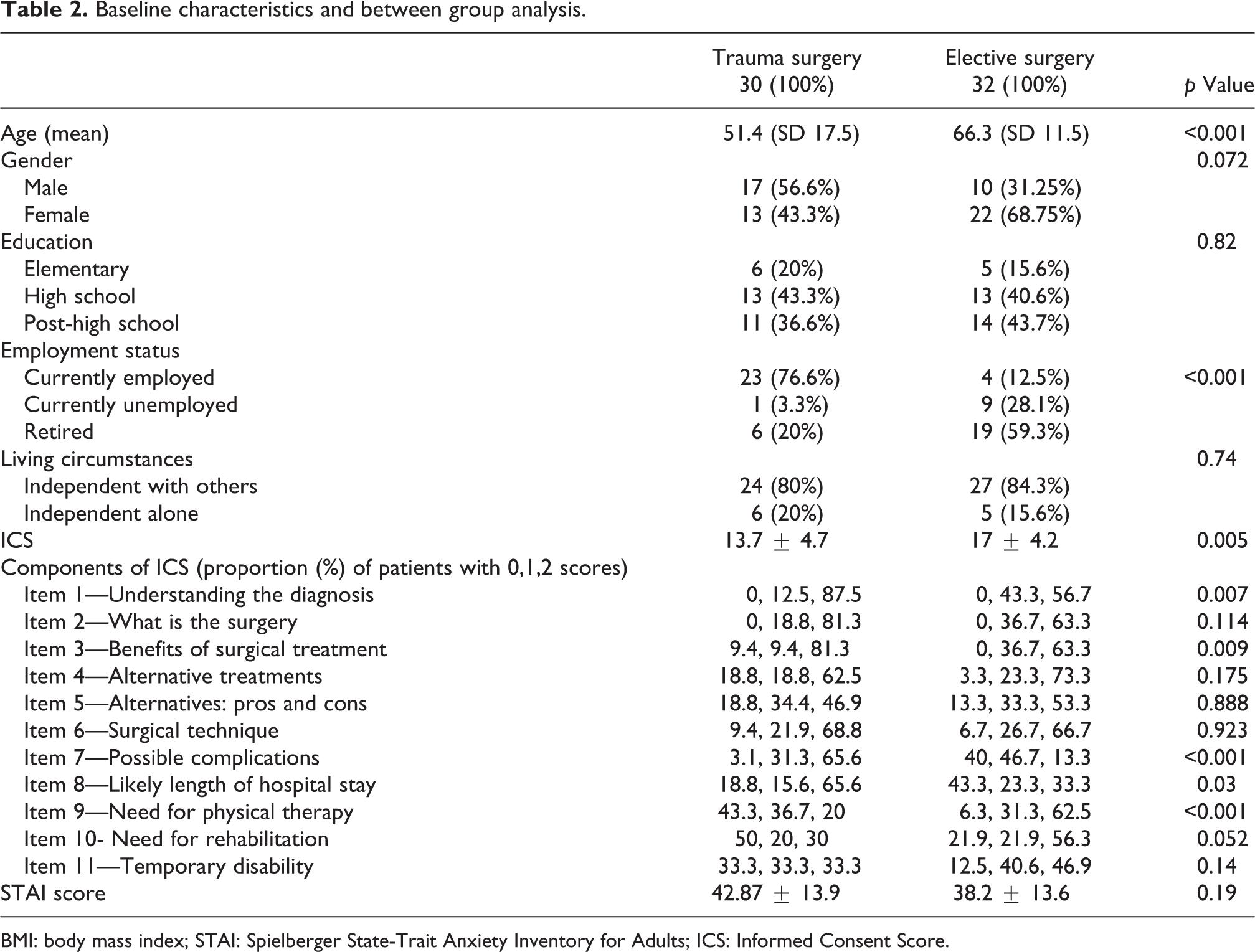
BMI: body mass index; STAI: Spielberger State-Trait Anxiety Inventory for Adults; ICS: Informed Consent Score.
Consent scores
Analysis of the consent score showed a significant difference between the two groups. Patients in the elective group showed an overall higher quality of consent, as reflected by a mean score of 17.03 ± 4.2 versus a mean score of only 13.73 ± 4.7 in the trauma group (p = 0.005, 95% CI: 1.02–5.57).
The difference in the mean consent scores remained significant after excluding the minor injuries from the trauma group (17.03 ± 4.2 in the elective group and 14 ± 4.9 in the trauma group (p = 0.016, 95% CI: 0.59–5.4)).
Several consent items were found to differ significantly between the two groups (Table 2). The trauma group patients demonstrated a significantly lower level of understanding, as reflected by the proportion of patients with a score of 2 in the following items: understanding the diagnosis, benefits of surgical treatment, possible complications, assumed length of hospital stay, and the need for physical therapy.
The scores differed significantly between the different subgroups of surgeries. While no significant difference was noted between patients undergoing TKA and THA (18.5 ± 2.7 vs. 16 ± 4.8, p = 0.97, 95% CI: −5.5 to 0.49), when all five subgroups were compared, the difference was statistically significant, as patients with minor trauma had lower scores (p = 0.02; Figure 1(a)). In the elective group, we did not find a correlation between age and consent score (Pearson r = −0.16, p = 0.37). On the other hand, in the trauma group, age was negatively correlated with the consent score (Pearson r = −0.53, p = 0.003; Figure 2).

Box plots demonstrating the different mean informed consent scores (a) and STAI scores (b) in the elective surgery subgroups compared with trauma subgroups. The boundaries are Tukey’s hinges. The median is identified by a line inside the box. The length of the box is the interquartile range and the whiskers represent the range. STAI: State-Trait Anxiety Inventory.
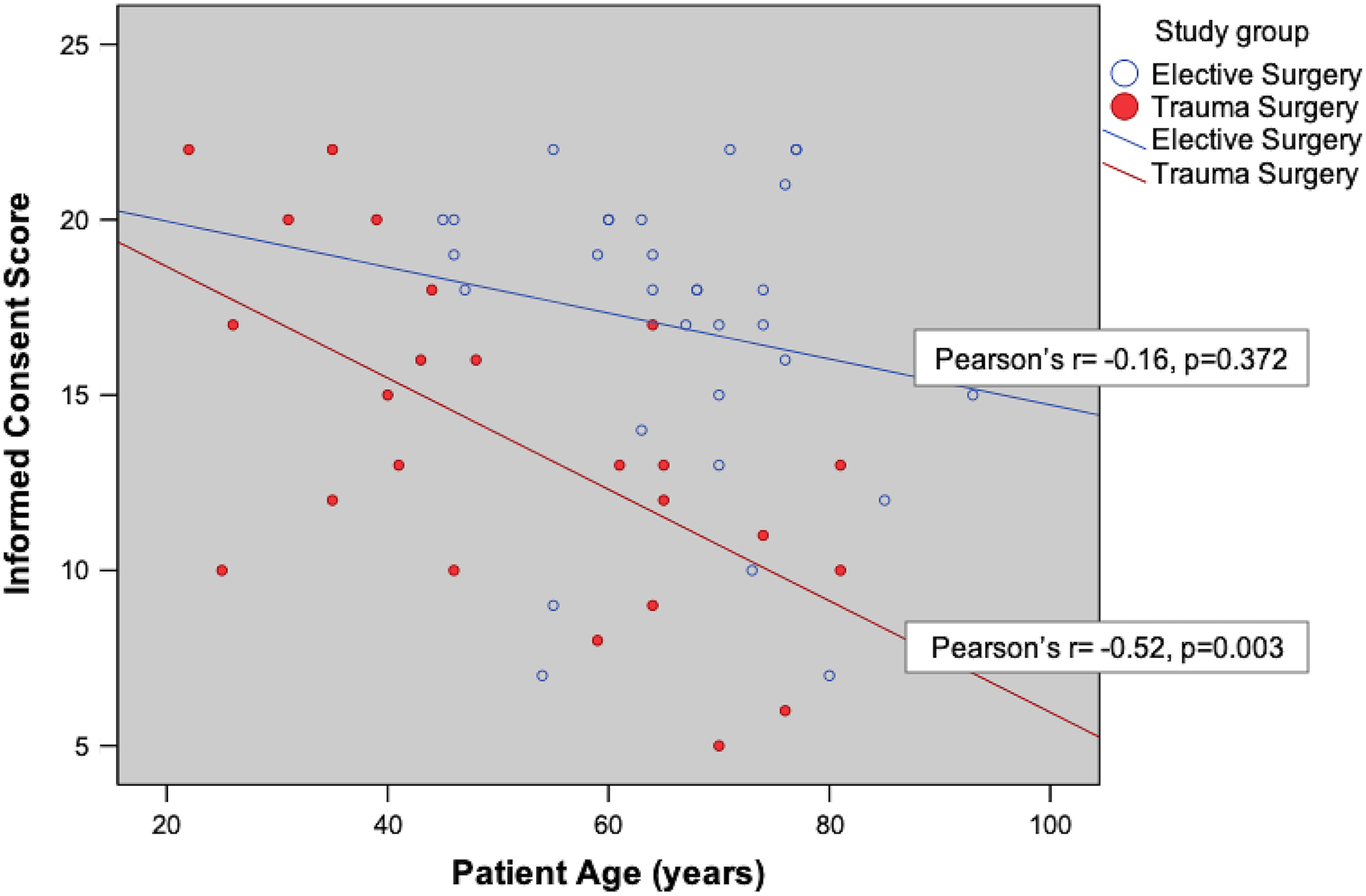
Graph depicting the correlation between patients’ age and informed consent scores, with the red dots and line representing trauma patients and blue representing elective patients. In the trauma group, there is a moderate negative correlation between age and consent score (Pearson correlation coefficient −0.53; p = 0.003).
Consent scores were significantly higher depending on the education level, when post-high-school education was compared to elementary education level (16.9 ± 4.1 vs. 12.2 ± 5.5, p = 0.021). Although scores differed significantly depending on employment status, these differences did not remain significant with post hoc analysis.
A three-way ANOVA was conducted to determine the effects of study group (elective vs. trauma), education level, and employment status. This showed that only the education level remained a statistically significant factor (p = 0.018), whereas belonging to a certain group and employment status were not significant (p = 0.16 and p = 0.18, respectively). Education remained the only significant factor also when only major cases were included (p = 0.008).
A multivariate linear regression model controlling for the following independent variables: age, gender, employment status, education level, the magnitude of surgery (major vs. minor), and the studied variable, type of surgery (elective vs. trauma) could significantly predict the informed consent score (F (6, 55) = 5.62, p < 0.0001, R 2 = 38%). The mean adjusted effect of surgery due to trauma was associated with a mean decrease of 3.48 points in the total consent score (p = 0.008).
STAI scores
Mean STAI score was not statistically different between the two groups. Although the elective group’s score was lower than that of trauma group, this was not statistically significant (38.28 vs. 42.87, respectively, p = 0.19, 95% CI: −11.6 to 2.4). After the exclusion of minor surgeries, there was still no significant difference between the elective and trauma groups (38.28 ± 13.6 vs. 45.2 ± 13; p = 0.06; 95% CI: −14 to 2.4). STAI did not differ significantly between different education levels (p = 0.873).
Analysis of differences between subgroups (Figure 1(b)) revealed that the highest scores were among patients undergoing femur/pelvic trauma surgeries (50.1 ± 11) and other major trauma surgeries (43.3 ± 13.5), while the lowest scores were obtained from patients undergoing minor operations (31.2 ± 13.7). Comparison of all five subgroups did not reveal a statistically significant difference in STAI score (p = 0.07).
We examined a possible correlation between overall consent score and STAI score. We found no correlation, whether the entire cohort was tested (r = −0.46, p = 0.72) (graph x) or each group separately.
Discussion
Informed consent is the process by which a patient agrees to undergo a medical procedure after careful consideration. The considerations include indications for treatment, alternatives, complications, and side effects. The quality of the informed consent process has ethical, medical, and legal ramifications. While there is established data in the literature regarding the patients’ level of understanding before elective surgery, 2,3,9,12 –14 the literature describing informed consent in patients facing urgent surgery for traumatic injuries is scarce.
The aim of the present study was to test the null hypothesis that there is no difference in the quality of the informed consent process consent obtained from orthopedic trauma patients versus elective patients.
For this comparison, we used, based on previous studies and guidelines for consent, a gradual score scoping all stages, or levels, of the informed consent process.
Our main outcome was a significant difference in the score between the trauma and elective groups, with a lower mean score in trauma patients. This finding is in line with previous studies that showed a lower level of understanding of patients undergoing urgent surgeries, not only in orthopedics.10 We demonstrated a higher anxiety level in the trauma group, as reflected by the STAI score, although this was not found to be statistically significant.
We also showed a correlation between the consent and the level of education, with a significantly better quality of consent in patients with post-high-school education, a finding in line with previous studies.15
In an attempt to improve patients’ understanding before a suggested procedure, several authors have advocated the use of supplementary materials such as written information sheets, 6,9 education classes, 16 and video education. 17 Smith et al. have demonstrated a significantly better recall of risks in trauma patients, when supplementary written information was given before giving consent. 6
We consider the ideal informed consent process to be a layered structure, with each item leaning on the previous one. The patient will not be able to fully comprehend the surgery offered to him without understanding the diagnosis and cannot understand the complications without first understanding what is being done in the surgery. For that reason, we have arranged the items by logical order of comprehension. First, the diagnosis is explained, with its ramifications and prognosis, then a treatment program is laid out, followed by alternatives, and so forth. When looking at the graph depicting the percentage of patients who received a full score for each item; for each group, there is a decline in the item score as the informed consent process unravels (Figure 3). The patients generally better understand the “basic” elements than the more “advanced” items. A complete consent process is time consuming. It is possible that the patient loses attention during the physician’s explanation and therefore disregards the more “advanced” items.

Graph depicting the percentage of patients in each item category that received a two-point score for that item. The items in the structured interview are arranged by a logical order of comprehension from left to right. The red line represents the trauma group whereas the blue line represents the elective group. The graph demonstrates a decline in the item score as the informed consent process unravels, which is steeper in the trauma group.
When analyzing the different score items of the informed consent process, several observations were made. The informed consent scoring remains relatively comparable during discussion of the diagnosis and surgery itself but falls rapidly when discussing complications and the postoperative management. This observation of declining understanding is more accentuated in the trauma group. It is also possible that the consenting physician, due to time limitations, goes through the last parts of the explanations with relative brevity or speed. Another possible explanation is that patients who have already made up their minds to move ahead with the proposed surgery are less likely to pay attention to the complications and aftercare parts of the discussion and therefore are able to recall them in less detail. Possibly it is too much to process and comprehend at this point, especially given the relatively short time between the trauma and the actual surgery. Elective group patients, on the other hand, have enough time to prepare for their procedure, sometimes several months, and are therefore more mentally prepared to grasp the further “advanced” aspects of their surgery. Another observation is that although the trauma group is comparable to the elective group in the understanding of the surgery and what the surgical procedure entails, they show less understanding of the diagnosis itself. This might be related to the relatively short time span between their injury, the time of diagnosis, and the treatment itself, in contrary to THA or TKA patients having months to years to “digest” their diagnosis. We also observed that both groups have a relatively lower understanding of the alternative treatments and even more the pros and cons of the alternatives. This can be explained both by physician’s bias, choosing to discuss this issue in lesser detail or emphasis, and the patient’s bias, “preferring” not to recall this now irrelevant option, after already making up their minds to proceed with surgery.
We acknowledge the several limitations of this study. Firstly, our two groups of patients are small and differ significantly in mean age and occupational status. Secondly, the trauma group consists of multiple and diverse procedures, thus making it more difficult to make a standard, uniform assessment. The magnitude and relevance of operative risks vary with different procedures. Thirdly, we captured the end product of the consent process, that is, the patient’s final comprehension, and did not record the actual process itself for analysis. Fourthly, we did not control or analyze the different time spans between obtaining the consent and performing the structured interview, and it is possible that the recall and understanding decayed steadily with time. Lastly, pain, sedative medications and psychological distress resulting from the injury can all affect the patient’s ability to understand and retain information. Although we were not able to control the impact of pain on our results, we did the STAI questionnaires to evaluate the patients’ anxiety levels.
Conclusions
The process of informed consent in the acutely injured orthopedic patient is challenging. We hypothesized that the informed consent obtained from patients undergoing elective surgery would be of higher quality when compared to trauma patients.
We found major differences in the quality of informed consent between trauma and elective patients, with the most vulnerable population being elderly patients who sustained traumatic injuries, as well as less educated patients.
Future research should concentrate on improving the quality of the entire decision-making process in this patient population, before the informed consent is finally obtained, with emphasis placed on improving the delivery methods used in the process.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.