
Abstract
A simple bone cyst is a tumor-like lesion that is not a true neoplasm. It usually presents as a solitary lesion within the proximal humerus and proximal femur. The etiology of simple bone cysts is still to be elucidated. We describe our experience in the successful surgical management of a rare case of two, large-sized, simple bone cysts involving the entire left humerus and right femoral head, respectively, in a 34-year-old male patient with Wilson’s disease and concomitant hepatic cirrhosis. We theorized that Wilson’s disease could be the cause of the delay or blockage of the natural healing process of the simple long-bone cysts, leading to their abnormal growth and development. To our knowledge, such a combined occurrence of multiple, simple long-bone cysts and Wilson’s disease has not been reported in the literature to date.
Introduction
A simple bone cyst is a tumor-like lesion that is not a true neoplasm. It usually presents as a solitary lesion, developing most frequently in the proximal humerus and the proximal femur.
The etiology of a solitary simple bone cyst is still unknown. We describe our experience in managing a rare case of multiple simple bone cysts involving the entire left humerus and the right femoral head in a 34-year-old male patient with Wilson’s disease. Wilson’s disease is a genetic disorder that leads to an accumulation of copper in the body, which adversely affects the liver and brain. This is the first such reported case of multiple simple bone cysts of the long bones associated with Wilson’s disease.
Case report
A 34-year-old male patient visited our outpatient clinic with the chief complaint of lateral left shoulder pain, following some trivial trauma. The patient had presented 1 month back with a history of intermittent pain involving the posterior aspect of the left shoulder. His past medical history revealed liver cirrhosis secondary to Wilson’s disease (which had been diagnosed 20 years back). The patient was being treated with
We performed radiography of the left shoulder joint to evaluate the cause of pain at the site. The anteroposterior (AP) and lateral plain radiographs of the left humerus revealed the presence of a well-defined, expansile osteolytic lesion with a fine sclerotic border and with associated cortical thinning. The mass was seen to occupy the complete humeral shaft including the humeral metadiaphyseal region (Figure 1(a) and (b)).

(a) and (b) The anteroposterior and lateral plain radiographs of the left humerus reveal a well-delimited, expansile osteolytic lesion with a fine sclerotic border, associated with cortical thinning. The mass is observed to occupy the whole humeral shaft including the metadiaphysis.
The T1-weighted coronal magnetic resonance image (MRI) of the humerus showed a multi-septate mass with low signal intensity, extending through the entire shaft (Figure 2(a)). The fat suppressing T1-weighted image of the mass revealed non-enhancing fluid content with a low signal, surrounded by a peripheral rim and septal enhancement (Figure 2(b)). Conversely, the fat-suppressing coronal T2-weighted MRI showed a high signal intensity mass with low signal rim and internal septations (Figure 2(c)). A technetium-99m anterior whole body bone scan revealed photopenia along the whole of the left humerus, indicating an increased and inhomogeneous uptake (Figure 3).
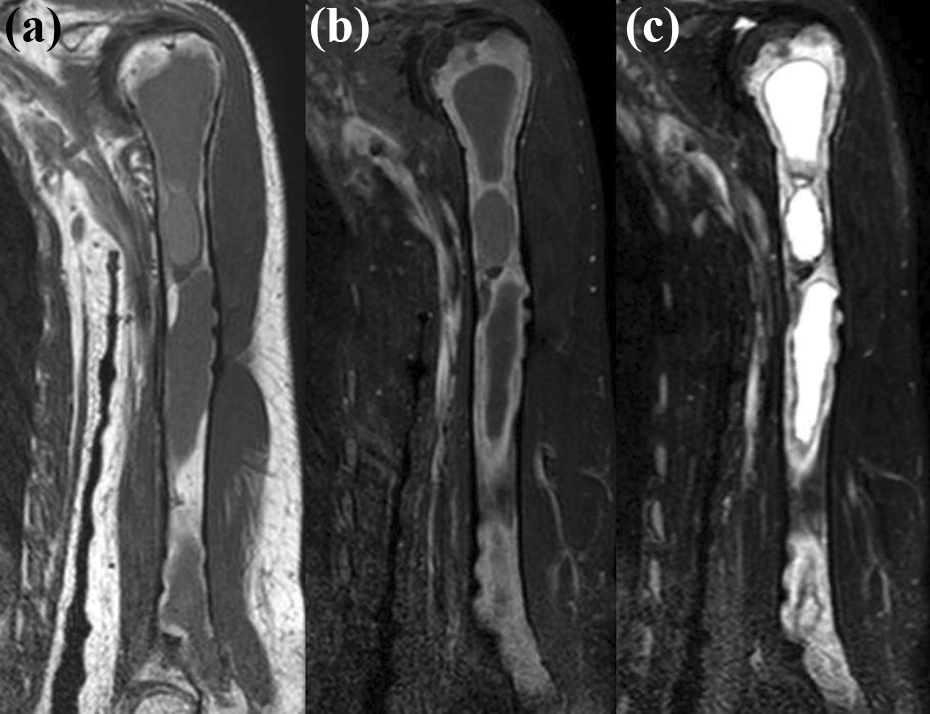
Preoperative magnetic resonance images of the left humerus. (a) A coronal T1-weighted image shows a multi-septate, low signal intensity mass occupying the whole humerus. (b) The fat suppressing T1-weighted image of the cystic mass reveals its non-enhancing, low signal fluid content with a peripheral rim and septal enhancement. (c) The fat suppressing T2-weighted coronal image shows a high signal intensity mass with low signal intensities indicating the rim and internal septations.

A technetium-99m anterior whole body bone scan shows photopenia (indicating an inhomogeneous increased uptake) along the entire left humerus.
An AP radiograph of both hips taken 5 years back showed a well-defined, radiolucent lesion with a thin peripheral sclerotic margin surrounding it (arrow) in the subtrochanteric region of the right proximal femur. The screw fixation performed for the left proximal hip fracture fixation was also evident in the image (Figure 4).

The anteroposterior radiograph of both hips reveals a well-defined, radiolucent lesion with a thin sclerotic margin surrounding its periphery (arrow) in the proximal subtrochanteric portion of the right femur; the screw fixation performed for the left proximal hip fracture is also evident.
Since the simple bone cyst involved the entire length of the humerus with an associated thinning of the proximal cortex, there was a high probability of the patient suffering additional pathological fractures. We therefore opted for surgical management of the cysts.
Discussion
A simple bone cyst was first described by Virchow 3 and has since been referred to using various terms such as solitary, hemorrhagic, traumatic, and primary bone cysts. Simple bone cysts normally occur in the second and third decades of life (91%), though they have been reported in patients from the ages of 1 to 53 years 4 and twice as prevalent in males. 2,5 The cysts arise in the proximal metaphyses of the humerus and femur and have the potential to spread toward the diaphysis along with bony growth in adults. They have also been reported at other sites such as the ileum, proximal tibia, distal radius, calcaneus, mandible, and small bones of the hand and foot. 2,6 Most patients are asymptomatic, with many lesions detected incidentally on radiographs. 7
The etiology and pathogenesis of these cysts is yet unclear. Cohen 8 suggested that the principal etiological factor is blockage of interstitial fluid drainage from an area of cancellous bone that undergoes rapid growth and remodeling. Investigations have revealed that the cystic fluid contains various inflammatory mediators, all of which may contribute to bony resorption. 9,10
The resultant small, asymptomatic lesions in the upper extremities can be managed expectantly with regular follow-up examinations using serial plain radiographs. The pathological fractures of the upper extremity in children that occur secondary to a simple bone cyst can be treated conservatively, because the fracture itself may initiate cyst “healing.” However, symptomatic or large-sized lesions at a risk of pathological fractures can be treated using several methods such as aspiration, curettage, injection of methylprednisolone, and bone grafting. The percutaneous injection of a steroid directly into the affected bone has been shown to be an effective and inexpensive treatment alternative, with less morbidity. The poor prognostic indicators for a successful outcome of this approach include age <10 years, the presence of multiloculated, large-sized, and radiographically active cysts, and long bone. 11
In our case, the humeral lesion was multiloculated and involved the entire shaft. Moreover, our patient suffered from recurrent hepatic comas, increasing the possibility of pathologic fractures following accidental falls. Therefore, we adopted a surgical approach with curettage and bone grafting to reduce the risk of these fractures in the future.
Mindelzun et al. 12 investigated the incidence and type of bone lesions in their patients with Wilson’s disease. They found one patient with multilocular cysts in the right femoral distal metaphysis and nine patients with subarticular cysts located in bones of the hands, wrists, feet, and ankles.
The relatively well-known musculoskeletal manifestations of Wilson’s disease include synovitis, early osteoarthritis, osteoporosis, rickets, and osteomalacia. The lesser known pathologies include spontaneous fracture, heterotopic ossification, scoliosis, epiphyseal dysplasia, genu varum, avascular necrosis of femoral head, and osteochondritis dissecans. 13
Aksoy et al. evaluated patients with Wilson’s disease to study and describe the characteristic bone changes encountered in this metabolic disorder. 14 While chronic hepatic dysfunction is known to be associated with osteoporosis and pseudocysts in some patients with cirrhosis, 15 the skeletal changes associated with Wilson’s disease typically included demineralization of maxillary or mandibular bones 16 and formation of osseous lacunae. 17
While the pathophysiology of the formation of these cysts is unknown, in our patient, the metabolic abnormalities due to liver cirrhosis secondary to Wilson’s disease could be responsible for a delayed healing of the initial lesions and may have led to the progression and development of huge simple bone cysts involving the humerus and the femoral head. Though cystic changes in small bones, associated with Wilson’s disease, have been reported, this is the first case report of a patient with Wilson’s disease diagnosed with multiple and large-sized simple bone cysts involving the long bones.
Conclusions
We present our successful experience in the surgical management of multiple and large-sized simple bone cysts of the humerus and femoral head in a patient with liver cirrhosis secondary to Wilson’s disease. We surmise that metabolic disturbances associated with Wilson’s disease might have interfered with the natural healing process of the simple bone cysts, leading to their abnormal growth and development. However, further in-depth studies of such cases are needed to validate this theory.
Research ethics and patient consent
This case report was approved by the institutional review board of Daejeon St Mary Hospital, College of Medicine, The Catholic University of Korea (IRB no. DC10EESE34). Informed consent was confirmed by the IRB0.
Surgical findings
The proximal metaphysis and diaphysis of the left humerus were exposed via the deltopectoral approach using a 20-cm long incision. A cortical window of 1 × 2 cm2 was created in order to access and examine the lesion at the proximal end of the humerus. Since the cortex at this site was very thin, we made holes at the four corners of a demarcated rectangular area with a Kirschner wire and used an osteotome to create the window. We aspirated 30 cm3 of serosanguinous fluid and found soft tissue contents within the cystic lesion. Simple curettage was therefore performed, and several cystic membranes were found and removed (Figure 5). We then performed chemical cauterization of the resultant cavity with 99% alcohol, following which the wound was thoroughly washed with saline, and a 30-cm3-sized chip was inserted as a bone allograft. Thereafter, the brachialis muscle was split at the humeral mid-level and the diaphysis was exposed. Another window of 1 × 2 cm2 was created at this site using the same technique. Simple curettage of the lesion was performed through this opening as well and the defect was also subsequently filled by inserting a 30-cm3 chip bone allograft. On plain radiographs and MRIs, the lesion at the distal humerus was observed to be very narrow, and the passage of a curette was deemed impossible. As it was difficult to perform curettage at this site, only chemical cauterization using alcohol was performed. 1,2

(a) and (b) Intraoperative images show the bony window and its contents at the proximal end and at the mid-shaft position of the humerus. (c) A photograph of the extracted cystic membranes following humeral curettage.
Despite the thinness of the cortical bone, the proximal humerus showed no pathological fractures. During bone curettage, we detected retention of blood-tinged fluid within the cyst, which was aspirated with a syringe and subjected to a subsequent cytological analysis. After 6 weeks of immobilization using an ultra-arm sling, the patient was able to resume his routine daily activities, and he returned to his job (of moving lightweight objects) after a further 3 months. During the 2-year follow-up, plain radiographs showed healed bony lesions within the proximal metaphysis and the diaphysis of the operated humerus (Figure 6). The patient also had a left-sided compression hip screw in situ due to the left subtrochanteric fracture 5 years back. As we performed a follow-up X-ray of the hip joint 6 years later, the radiological findings indicated a simple bone cyst of the right femoral head. The cyst was aspirated and 200 mg of methylprednisolone (Depo-Medrol) was injected into the cavity. The aspirate was found to be a yellowish serous fluid and cytological examination findings corresponded to that of a simple bone cyst. Four months after the treatment of the simple bone cyst of the right femur, the patient died of hepatic failure.

(a) and (b) The postoperative, 2-year follow-up anteroposterior and lateral plain radiographs of the humerus show healing with sclerotic densities in the whole shaft of the humerus and thickening of the cortex.
Pathological examination findings
The cytology of the cystic fluid aspirated from the humeral cyst showed few lymphocytes and several macrophages against a bloody background. Grossly, the extracted tissue specimen consisted of multiple fragments of grayish to dark brown, thin, and membranous soft tissue interspersed with some bony tissue, measuring up to 3.5 × 2.1 × 0.2 cm3. The microscopic examination of the tissue revealed multiple cysts lined by well-vascularized connective tissue with some hyalinization and myxoid changes observed adjacent to the trabecular bone. The lining cells of the cysts could not be identified. In addition, tissue microscopy revealed foreign body giant cells with cholesterol clefts and fibrinoid deposits along with a focal chronic inflammatory infiltrate containing lymphocytes, plasma cells, and multiple foci of hemorrhage (Figure 7). No copper deposits were detected in the humeral biopsy specimen. These findings corroborated the diagnosis of a simple bone cyst. In the cytological examination of the aspirate from the right hip, some lymphocytes and neutrophils were found against a bloody background. No deposits of copper were detected in this specimen either.
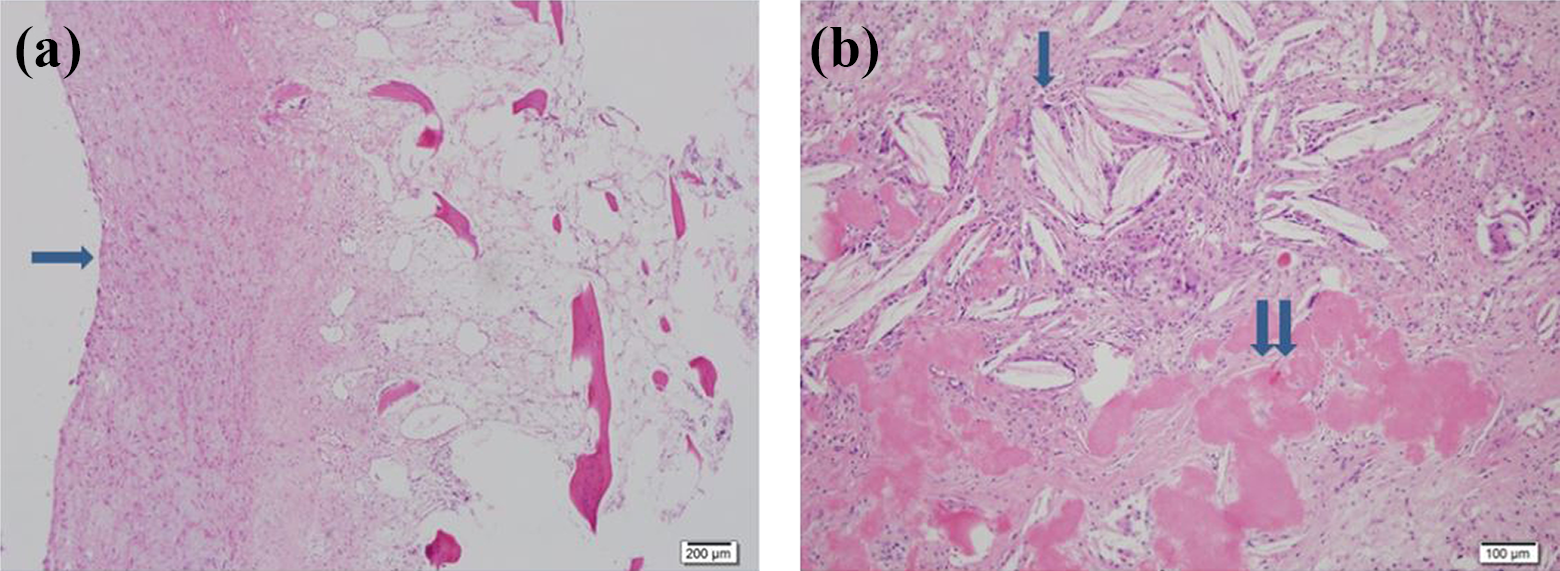
(a) A microscopic examination of the curetted cystic contents reveals well-vascularized connective tissue (arrow). (b) Cholesterol clefts with multinucleated giant cells (arrow) and fibrinoid deposits (paired arrows) are observed throughout the specimen (hematoxylin and eosin stain, (a) ×12.5 and (b) ×100).
A written informed consent for patient information and images to be published was provided by the patient before his death.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.