
Abstract
Purpose:
The distal tibiofibular syndesmosis is an important structure for ankle stability. The objective of this study was to evaluate the motion of the syndesmosis under different loading patterns and determine the characteristics of the syndesmotic motion.
Methods:
Six fresh cadaveric lower extremity specimens with the knee reserved were tested in this study. The skin and muscles were removed with all ligaments around the syndesmosis and knee and ankle joint intact. An axial load of 600 N was applied to the specimens with the ankle joint in 10° dorsiflexion, neutral position, and 15° plantar flexion using a universal material testing machine. Then, with the ankle joint positioned neutrally, a combination of 600-N axial and 5-Nm torsional external rotation loading was applied to the specimens. The medial–lateral and anterior–posterior displacement and rotation of the distal fibula relative to the distal tibia were measured.
Results:
Under the axial loading, the distal fibula tended to move medially and anteriorly and rotate internally with the ankle positioned from the neutral position to 15° plantar flexion. Meanwhile, when the ankle was positioned from the neutral position to 10° dorsiflexion, the distal fibula tended to move laterally and posteriorly and rotate externally. Under the combined loading, with respect to the isolated axial loading, the distal fibula tended to move medially and posteriorly, and rotate externally relative to the distal tibia.
Conclusion:
Micro motion existed in the syndesmosis. The relative motion of the syndesmosis was correlated to the ankle position and loading patterns.
Introduction
The distal tibiofibular syndesmosis is an important functional structure to maintain ankle stability during weight-bearing and walking. The distal fibula and tibia and syndesmotic ligaments form a stable articulation. The syndesmosis provides a strong lateral buttress for the ankle mortise joint and resists the axial, rotational, and translational forces that attempt to separate these two bones. 1,2 Previous studies showed that the fibula takes 6.4% to 17% of the axial load during weight-bearing. 3,4 Movement of the distal fibula relative to the tibia can make the fibula bear part of the load timely to maintain the mechanical stability of the ankle joint.
Syndesmotic injury accounts for 1% to 10% of all ankle sprains, and this injury is more common in ankle fractures, accounting for about 10% of ankle fractures and 25% of ankle fractures that require surgery. 1,5 Syndesmotic injuries are most frequently caused by external rotation or dorsiflexion forces. Brosky et al. 6 reported that either foot dorsiflexion or plantar flexion may result in syndesmotic injury when maximal tension is achieved with external rotation.
For the treatment of syndesmotic instability, the AO/ASIF group recommends the use of syndesmotic screw fixation, which might disturb the normal motion and result in chronic pain or hardware failure if the screws were not removed after healing of the syndesmosis. A more recent development is a flexible fixation using the suture-button fixation devices, which have the potential advantage of preserving the physiological motion of the syndesmosis and obviate the need for a second surgery for routine hardware removal. 5,7
Recently, motion of the syndesmosis has drawn much attention. However, there are few research studies on the physiological motion of the syndesmosis, especially those which simulate the normal gait or injury mechanism. The purpose of this study was to analyze the motion of the syndesmosis under different loading patterns and explore the biomechanical characteristics of the syndesmosis.
Methods
Specimen preparation
A total of six fresh frozen cadaveric lower extremity specimens were used. Ethical approval was obtained from the Human Research Ethics Committee of Tongji Hospital, Tongji University School of Medicine (KYSB-2015-56). The average donor age was 36 years (range, 28–54 years). The specimens were amputated 10–15 cm above the knee, stored at −20°C, and thawed at a room temperature for 12 h before use. Evident preexisting foot abnormalities were excluded by visual inspection and review of the medical history. X-rays were performed to rule out osteoarthritis, previous fractures, tumors, osteonecrosis, and foot deformities.
The skin, muscles, and other soft tissues of the legs were removed until the tibia and fibula were exposed. The patella and ligaments around the knee joint were kept intact. The soft tissue structure around the proximal tibiofibular joint was not disturbed. Additionally, the skin and soft tissue of the foot, interosseous membrane, and capsule and ligaments of the ankle joint, including the syndesmotic ligaments, were kept intact. Two 6.5-mm cancellous screws were used to fix the distal femur and proximal tibia to lock the knee in the neutral position. Moreover, two 3.5-mm cortical screws were used to fix the subtalar joint in the neutral position. The custom-made black-beaded pins were inserted into the distal tibia and fibula, which constitute the syndesmotic joint, as identification points. The exact locations of the points were at the anterolateral Tillaux tubercle and posterolateral Volkmann tubercle on the distal tibia surface and at the Wagstaffe tubercle, the insertion point of the posterior inferior tibiofibular ligament, and the lateral point on the distal fibular surface.
Biomechanical testing
The specimen was placed on a loading platform, keeping the tibia perpendicular to the horizontal plane. The femoral stump was fixed on top of the loading machine (DDL20, Changchun Research Institute for Mechanical Science Co. Ltd, Changchun, China). A specially designed fixation system was used to fix the foot, which maintained the ankle joint in 10° dorsiflexion, neutral, and 15° plantar flexion position (Figure 1). In the normal gait, ankle dorsiflexion is about 10°, and plantar flexion is approximately 10–15°. 8,9 Therefore, this study was designed to keep the ankle in 10° dorsiflexion, neutral, and 15° plantar flexion position. The fibula was not fixed so that movements of both the proximal and distal tibiofibular joint were not affected. Three digital cameras, positioned laterally, posteriorly, and in front of the specimen, perpendicular to each other, were used to capture the motion of the specimen.

Different ankle positions produced by a specially designed fixation system: 10° dorsiflexion (a), neutral position (b), and 15° plantar flexion (c).
The DDL20 electronic universal testing machine was used to apply a load to the specimens. The specimens were preloaded for 10 cycles with an axial load of 600 N and torsional external rotation load of 5 Nm to allow for muscle tensioning and mechanical equilibrium. The 600-N axial load was equivalent to the body weight of a 60-kg individual, which was a common load in most biomechanical testing reported in the literature. 10,11 The 5-Nm torsional external rotation load was applied to simulate the syndesmotic injury mechanism, which was usually used for nondestructive biomechanical testing of the syndesmosis. 12,13 In the formal experiment, the 600-N axial load was applied at a rate of 10 mm min−1. The 5-Nm torsional external-rotation load was applied at a rate of 0.5° s−1, with the axial load maintained at 600 N. When the loading process was complete, the load was maintained for 30 s to allow for data recording. The experimental scene is presented in Figure 2.

The experimental scene.
The testing procedures were as follows: (1) The ankle was in 10° dorsiflexion, neutral, and 15° plantar flexion position. A 600-N axial load was applied on the specimen. (2) The ankle was in a neutral position. A combined load was applied on the specimen (600-N axial load and 5-Nm torsional external rotation load). Measurement of the medial–lateral and anterior–posterior displacement and rotation of the distal fibula relative to the distal tibia were performed. The digital image correlation method was used to calculate the data. 14 The calculating program was provided by the Department of Mechanics, Shanghai University, China.
Statistical analysis
All data were expressed as mean ± standard deviation. Statistical analysis was performed using SPSS version 20.0 for Windows (SPSS Inc., Chicago, USA). A normality test was performed first. If the data set was normally distributed, a paired t test was used for two-group comparison, and a one-way analysis of variance was used for multi-group comparison. When differences existed between groups, the Tukey’s post hoc test was used to make multiple comparisons. The level of significance was set at p < 0.05. If the data set was not normally distributed or inequality of variances existed, the Kruskal–Wallis H test was used. Post hoc multiple comparisons were done with a non-parametric Mann–Whitney U rank sum test when a Kruskal–Wallis H test was significant. A Bonferroni corrected value of p < 0.05/[n × (n − 1)/2] was considered statistically significant, and n was the number of comparison groups.
Results
Axial loading with different ankle positions
Under an axial load of 600 N, data on the relative motion of the syndesmosis with the different ankle positions are presented in Table 1.
Relative motion of the distal fibula under an axial load of 600 N.

MLD: medial–lateral displacement; APD: anterior–posterior displacement; NP: neutral position; PF: plantar flexion; DF: dorsiflexion.
aNegative value means medial displacement.
bNegative value means anterior displacement.
cKruskal–Wallis H test.
dNegative value means internal rotation.
When the ankle position was changed from the neutral position or 10° dorsiflexion to 15° plantar flexion, the distal fibula moved medially and anteriorly and rotated internally relative to the tibia. Meanwhile, when the ankle position was changed from the neutral position or 15° plantar flexion to 10° dorsiflexion, the fibula moved laterally and posteriorly and rotated externally relative to the tibia (Table 2).
Motion change of the distal fibula under an axial load of 600 N.
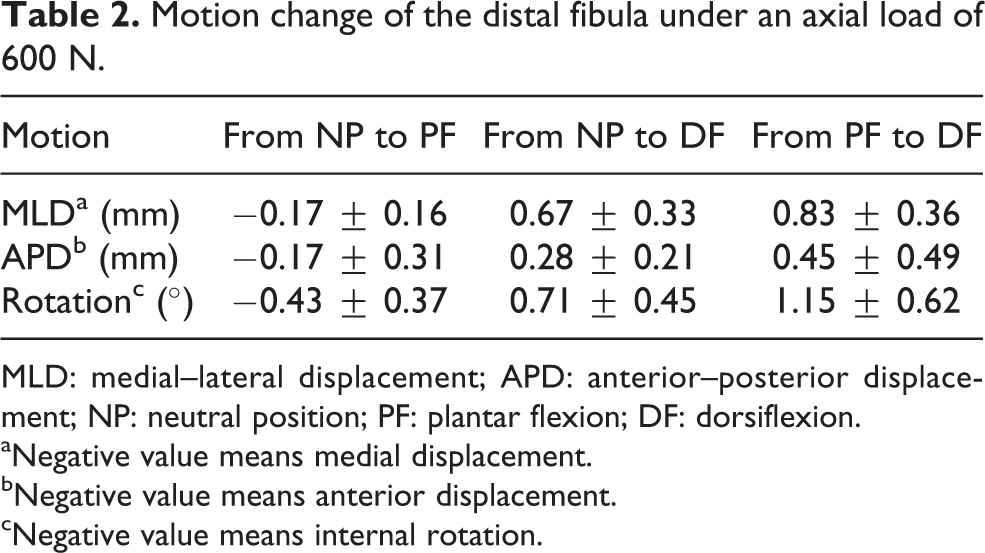
MLD: medial–lateral displacement; APD: anterior–posterior displacement; NP: neutral position; PF: plantar flexion; DF: dorsiflexion.
aNegative value means medial displacement.
bNegative value means anterior displacement.
cNegative value means internal rotation.
For the specific displacement or rotation, the ankle position exerted different effects on the distal fibular motion. No significant difference was noted on the medial–lateral displacement in the neutral position compared with that in plantar flexion (p > 0.05). Nevertheless, a significant difference was observed on the medial–lateral displacement in the neutral position and plantar flexion compared with that in dorsiflexion (p < 0.05). With respect to the anterior–posterior displacement, compared with the neutral position, no significant difference was noted during dorsiflexion and plantar flexion (p > 0.0167). In contrast, there was a significant difference between dorsiflexion and plantar flexion (p < 0.0167). No significant difference was observed in the rotation of the distal fibula between the neutral position and plantar flexion (p > 0.05). However, a significant difference was noted on the rotation of the distal fibula in the neutral position and plantar flexion compared with that in dorsiflexion (p < 0.05, Table 3).
p Value for comparison of the motion of the distal fibula in different ankle positions.
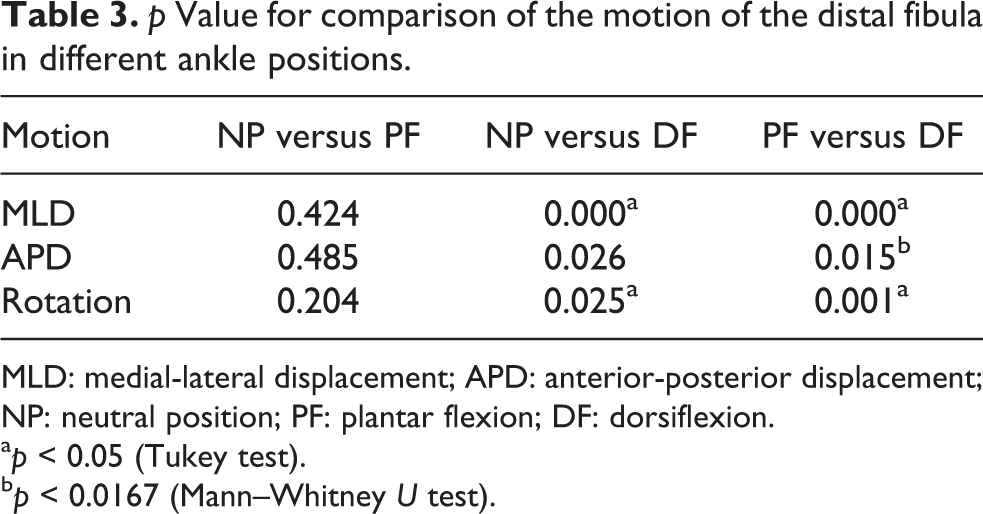
MLD: medial-lateral displacement; APD: anterior-posterior displacement; NP: neutral position; PF: plantar flexion; DF: dorsiflexion.
a p < 0.05 (Tukey test).
b p < 0.0167 (Mann–Whitney U test).
Combined loading with the ankle in neutral position
Under the combined loading, the medial and posterior displacement and external rotation of the distal fibula relative to the distal tibia were 0.25 ± 1.01 mm, 1.65 ± 0.56 mm, and 1.59 ± 0.67°, respectively. Compared with isolated axial loading, the distal fibula moved medially and posteriorly and rotated externally under a combined loading. With the axial loading maintained, the medial and posterior displacement and external rotation of the distal fibula were 0.33 ± 1.04 mm, 1.67 ± 0.50 mm, and 1.50 ± 0.73°, respectively, after adding the torsional external rotation loading. No significant difference was noted in the medial–lateral displacement between both loading patterns (p > 0.05). However, there were significant differences in the anterior–posterior displacement and rotation of the distal fibula (p < 0.05, Table 4).
Comparison of the motion of the distal fibula under different loading patterns.

MLD: medial–lateral displacement; APD: anterior–posterior displacement.
aNegative value means medial displacement.
bNegative value means anterior displacement.
c p < 0.05.
dNegative value means internal rotation.
Discussion
The distal tibiofibular syndesmosis is between the rough medial convex surface of the distal fibula and the triangular fibular notch of the lateral surface of the distal tibia. 2,15 The two osseous parts of the syndesmosis are linked by four ligaments, that is, the syndesmotic ligaments, including the anterior inferior tibiofibular ligament, interosseous ligament, posterior inferior tibiofibular ligament, and inferior transverse ligament. The anterior inferior tibiofibular ligament extends obliquely from the anterolateral Tillaux-Chaput tubercle of the distal tibia to the anteromedial Wagstaffe-Le Fort tubercle of the distal fibula. The interosseous tibiofibular ligament is continuous with the interosseous membrane at its most distal aspect, representing the thickened distal portion of the interosseous membrane. The posterior inferior tibiofibular ligament originates from the posterolateral Volkmann tubercle of the distal tibia and inserts at the posterior edge of the lateral malleolus. The inferior transverse ligament originates from the lateral malleolar fossa just below the posterior tibiofibular ligament, covers the superior part of the talus, and is often considered as the deep part of the posterior inferior tibiofibular ligament. 2,15 –17
The syndesmosis is usually regarded as a fibrous joint. 2,18 There is a small area at the base of the syndesmosis where the tibia and fibula are in direct contact. This area is called the tibiofibular contact zone. The contact facets of the bones are covered with a thin articular cartilage about 0.5–1.0 mm thick. The rim of the cartilage is continuous with the articular facet of the tibial plafond and fibular malleolus. 18 The size of the contact facets is rather small, sometimes they are mere ridges. Bartonícek 19 dissected the tibiofibular syndesmosis in 30 cadaveric specimens. In seven cases, the direct contact areas were absent, the tibia and fibula were separated by the synovial plica, and the fibular cartilaginous facet was also absent. But on the tibia, it was missing only in one of these seven cases. In the other 23 cases, cartilaginous facets were found on both bones. He thought that the distal tibiofibular articulation was not a syndesmosis but rather a synovial joint. To some extent, we believe that micro motion exists between the distal tibia and distal fibula because of the existence of the cartilaginous facet.
The results in the current study showed that the distal tibiofibular syndesmosis was a slightly movable joint. Some literature studies reported that micro motion existed in the syndesmosis, which can be classified as in vitro and in vivo.
In vitro cadaveric studies were chosen by some investigators. Peter et al. 20 performed a biomechanical testing using eight cadaveric specimens. They found that lateral translation and external rotation of the lateral malleolus occurred while the ankle was moved from plantar flexion to dorsiflexion under a constant axial loading of 700 N. Displacements of up to 1.25 mm and rotations of up to 2° were recorded. Markolf et al. 1 investigated 27 specimens and found that the distal fibula was always displaced posteriorly with respect to the tibia, with no measurable medial–lateral displacement during forced ankle dorsiflexion and external foot torque tests. Huber et al. 21 measured the motion of the fibula relative to the tibia in eight embalmed cadaveric specimens using a 3-D motion system. Without any loading, the relative motion was measured from 50° plantar flexion to 30° dorsiflexion. The results were 1.7 ± 0.41 mm in medial–lateral displacement, 1.3 ± 0.33 mm in anterior–posterior displacement, and 2.7 ± 1.08° in internal–external rotation.
Regarding the in vivo studies, Beumer et al. 22 investigated the normal kinematics of the distal tibiofibular syndesmosis in 11 healthy volunteers using the radiostereometric analysis. No recognizable patterns of fibular movement were found in relation to the tibia during weight-bearing in the neutral position. Application of an isolated 7.5-Nm external rotation moment on the foot caused external rotation of the fibula between 2° and 5°, medial translation between 0 mm and 2.5 mm, and posterior displacement between 1.0 mm and 3.1 mm. Wang et al. 23 studied 16 healthy syndesmoses of 16 individuals during the stance phase of the normal gait using a 3-D to 2-D registration technique. They reported that the distal tibiofibular joint exhibited 2.98 ± 1.10° of dorsal–plantar flexion, 5.94 ± 1.52° of inversion–eversion, and 5.99 ± 2.00° of internal–external rotation and 2.63 ± 1.05 mm on medial–lateral, 3.86 ± 1.65 mm on anterior–posterior, and 4.12 ± 1.53 mm on superior–inferior translation during the stance phase.
In our study, the specimens were loaded in different ankle positions to simulate the normal gait, an axial load of 600 N was used to simulate the body weight, and a 5-Nm torsional external rotation load, which was nondestructive to the syndesmosis, was used to simulate the syndesmotic injury mechanism. 12,13 The results showed that motion of the distal fibula relative to the distal tibia was different when the ankle position was changed. Under the combined loading, the distal fibula tended to move posteriorly and rotate externally. We speculate that rupture of the syndesmosis might be caused by excessive moving of the distal fibula posteriorly and rotating externally under a sudden external rotation force, rather than moving laterally.
Based on the results of our study and other related literature, micro motion exists in the distal tibiofibular syndesmosis. As a result, when treating syndesmotic injuries in clinical practice, the surgeons should pay much attention to this biomechanical characteristic. At present, screw fixation is still the gold standard for the treatment of syndesmotic injury. However, the rigid fixation would hinder the motion of the syndesmosis and often led to screw breakage. Although tricortical fixation may theoretically lessen the rate of screw breakage, studies have shown 10–29% screw breakage for tricortical syndesmotic screws during full weight-bearing. 24 Therefore, removal of syndesmotic screws prior to weight-bearing is advocated. 25 Manjoo et al. 26 retrospectively reviewed 106 patients with syndesmotic fixation and summarized that an intact syndesmosis screw was associated with a worse functional outcome compared with loose, fractured, or removed screws. However, there were no differences in the functional outcomes between loose or fractured screws and removed screws. Screw removal will unlikely benefit patients with loose or fractured screws, but may be indicated in patients with intact syndesmosis screws. In recent years, flexible fixation has begun to appear and gradually become popular. A recent meta-analysis showed that the suture-button fixation had significantly better functional score, ankle motion, and time to full weight-bearing and lesser complications based on the short- and intermediate-term follow-up data. 27 Consequently, choosing a reasonable treatment for syndesmotic injury based on the motion characteristics of the syndesmosis is recommended. We suggest flexible fixation or early removal of the syndesmotic screw prior to full weight-bearing.
There were some limitations to this study. First, the cadaveric study could only reflect the acute change of the parameters, which might not always be consistent with those in the living body. Second, the number of the specimens was too small, causing limited results. To some extent, the significance of the results could not be conclusive. Third, dynamic loading to simulate the whole normal walking gait could not be performed. Furthermore, not all motions in every plane were analyzed.
Conclusion
The distal tibiofibular syndesmosis is a joint with micro motion. The motion of the distal fibula relative to the distal tibia was correlated to the ankle position and loading patterns. The physiological motion of the syndesmosis should be taken into accounts in the clinical treatment of syndesmotic injuries.
Footnotes
Acknowledgment
We thank Professor Dong-sheng Zhang and his research team of the Department of Mechanics in Shanghai University for their excellent technical support.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study is sponsored by National Natural Science Foundation of China (grant no. 81501884).