
Abstract
The objective of study was to evaluate a case series of patients in whom polyetheretherketone (PEEK) cages were used for anterior column reconstruction in vertebral osteomyelitis. Fifteen patients underwent clinical and radiological evaluation with average follow-up of 26 months. Parameters assessed were time of surgery, blood loss, segmental kyphosis or lordosis angle, time to solid bony fusion, ambulatory status, and functional outcome. Mean time of surgery was 150 min with mean blood loss of 530 ml. One patient died in early postoperative period. All patients without preoperative neurologic deficit were walking unaided first day postoperatively. Solid bony fusion was demonstrated in 14 patients, on average 7.1 months postoperatively. Functional outcome at the latest follow-up was excellent, good, or fair in 86%. Two failures with recurrent infection were treated with PEEK cage removal and reinstrumentation. High success rate could be expected when PEEK cages are used for anterior column support in pyogenic vertebral osteomyelitis.
Brief introduction
Treatment of pyogenic vertebral osteomyelitis is mostly conservative with antimicrobial therapy according to causative microorganism and external bracing. 1 There is a subset of patients, however, who will need operative treatment either because of progressive neurologic deficit, mechanical instability, progressive deformity, presence of epidural abscess, failure of conservative treatment, or intractable mechanical pain. 1,2
There are many techniques and approaches for the treatment of septic spine conditions. The mainstay of treatment is radical debridement of anterior column, which necessitates appropriate reconstruction, traditionally with autologous bone and in recent years using titanium cages. 1,3
Polyetheretherketone (PEEK) cages gained wide acceptance in degenerative spine conditions. 4 Compared to titanium, their modulus of elasticity is closer to cortical bone and their radiolucency enables better assessment of bony fusion. 5 Recently, few reports emerged of favorable results using PEEK cages in septic spine conditions. 6 –8
The aim of the present article was to present a case series of patients operatively treated with PEEK cages for anterior column support in pyogenic vertebral osteomyelitis.
Patients and methods
Between May 2009 and May 2014, 15 patients with one level pyogenic vertebral osteomyelitis were operated using PEEK cages for anterior column reconstruction. Two cases involved cervical spine (Figure 1), four cases thoracic spine, and nine cases lumbar spine. There were 5 female and 10 male patients with an average age of 59 (range 40–82) years at the time of surgery. In seven cases, infection was hematogenous, and in seven cases, infection occurred after herniated lumbar disc surgery and once after lumbosacral transaxial fixation. Causative organisms were identified by intraoperative tissue samples, using standard culturing systems. Additionally, samples were sent to PCR (Polymerase chain reaction) analysis for the presence of Mycobacterium tuberculosis DNA. Causative bacteria were identified in all cases. All demographics and baseline characteristics are presented in Table 1.

A 55-year-old female (patient no. 9) with osteomyelitis of C6–C7. T1-weighted MRI image preoperatively showed C6–C7 affection with spinal canal narrowing and epidural abscess (a). Postoperative lateral X-ray showed solid bony fusion at the latest follow-up (b).
Preoperative data.

aAmbulatory status is measured as ability to walk unaided.
Significant medical comorbidities were seen in six patients. Three suffered from a long-term diabetes mellitus, one having septic arthritis of a shoulder, one patient had a history of cerebellar vascular insult, one had chronic kidney failure and used dialysis, one had chronic obstructive pulmonary disease, and one had pulmonary fibrosis.
In cases of thoracic and lumbar osteomyelitis, surgery was performed through midline dorsal approach over the affected segments. Pedicle screws were inserted (Xia, Stryker Spine, Allendale, NJ, USA; Quantum, Pioneer Surgical Technology, Marquette, MI, USA) and secured with rods. Two neighboring segments were instrumented (Figure 2) with an exception of two patients in whom three and four segments were instrumented (Figure 3).

A 63-year-old male (patient no. 5) with osteomyelitis of L4–L5. T1-weighted MRI image showed spinal canal narrowing (a). Postoperative lateral X-ray showed intervertebral bone formation 4 months after surgery (b).
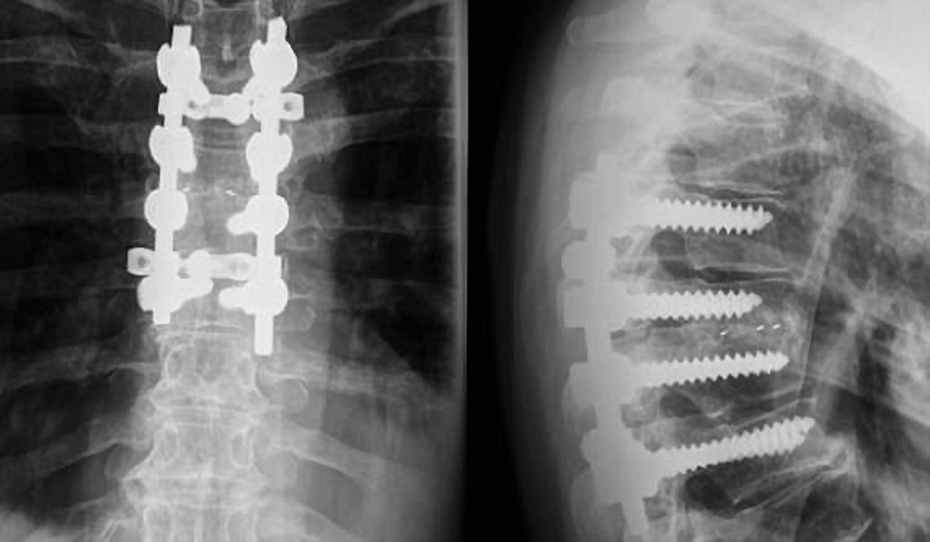
A 62-year-old female (patient no. 4) with Th5–Th6 osteomyelitis. X-Rays 8 months postoperatively showed solid interbody fusion at the affected level.
With the affected segment stabilized, posterior decompression was performed, followed by anterior decompression consisting of evacuation of the affected intervertebral disc (IVD) and debridement of terminal endplates. In thoracic cases, costotransversectomy was performed to provide more lateral access to the disc. Special care was taken while dissecting soft tissues from dural sac. Affected segments were approached from more affected side. Anterior column support was secured using PEEK cage (Boomerang, Medtronic, Minneapolis, MN, USA; T-Plus, Pioneer Surgical Technology, Marquette, MI, USA). Bone obtained from posterior elements was put into the cage and at anterior third of IVD. During cage placement, care was taken not to damage any adjacent nerve structures. Cage of maximal possible height was placed as anteriorly as possible followed by posterior compression to maintain lordosis in lumbar cases.
In a case of cervical osteomyelitis, surgery was performed through the left anterolateral approach. IVD was evacuated and terminal endplates debrided. After opening the posterior longitudinal ligament, decompression of anterior epidural space was performed. Anterior column instrumentation was obtained with PEEK cage (Cervical I/F Cage, DePuy Spine, Raynham, MA, USA) and plating (Slim-Loc, DePuy Spine, Raynham, MA, USA). The cage was not filled with bone or any other material.
Deep drain was retained until drainage was reduced to less than 50 ml/day on two consecutive days, but for no less than 3 days. Antibiotic therapy was administered according to sensitivity testing and given intravenously for at least 6 weeks. Thereafter, antibiotics were continued orally for 4 weeks or in cases of elevated CRP and sedimentation rate until their values returned to normal.
In a case of infection after lumbosacral axial fixation (patient no. 11), the retroperitoneal approach was employed to explant overtly loosened axial screw followed by pedicle fixation and anterior column reconstruction performed via dorsal approach in the same session.
Clinical data were recorded, including time of surgery, blood loss, and ambulatory status. Patients were followed at monthly intervals until solid bony fusion was demonstrated. Latest follow-up was on average 26 months postoperatively. Every assessment consisted of neurologic work-up and standard plain X-rays. In inconclusive cases, computed tomography was performed to assess bony fusion. Angle of segmental kyphosis for thoracic spine and angle of segmental lordosis for lumbar and cervical spine were obtained preoperatively, postoperatively, and at the latest follow-up. Functional outcome using Kirkaldy-Willis criteria was determined at the final follow-up.
All procedures performed were in accordance with the ethical standards and with the 1964 Helsinki Declaration. Written informed consent for patient information and images to be published were provided by all participants included in the study.
Results
Surgery was commenced eight times as emergency procedure: three times due to paraplegia and twice due to paraparesis all lasting for less than 48 h, twice due to acute radiculopathy with paresis of a lower limb (foot dorsiflexion, knee extension) and once because of acute radiculopathy with paresis of an upper limb (shoulder abduction and elbow flexion).
Mean time of surgery was 150 min with mean blood loss of 530 ml. Solid bony fusion was achieved in 14 of 15 patients on average 7.1 months postoperatively. One patient (no. 15) died 11 days after surgery because of respiratory failure. Surgical procedure resulted in an average increase of segmental lordosis of 5.1°, decrease of thoracic segmental kyphosis of 4.7°, and decrease of cervical segmental lordosis of 0.5°. Loss of corrective changes was observed at final follow-up with an average decrease of lumbar lordosis of 4.9°, increase of thoracic kyphosis of 5.3°, and decrease of cervical lordosis of 0.5° (Table 2). Patients without preoperative neurologic deficit took 1 day to walk unaided. Four of the five patients with upper motor neuron dysfunction made partial recovery. Two patients with lumbar radiculopathy recovered completely and a patient with cervical radiculopathy recovered partially.
Perioperative and follow-up data.

aNegative values represent angulation in lordosis.
Patient self-assessed functional outcome based on the Kirkaldy-Willis criteria showed excellent result in three patients, good in six patients, and fair in three patients. Two patients had symptoms of recurrence with poor outcome and are presented in detail.
Patient no. 6 was admitted from a local hospital due to severe mechanical back pain and elevated CRP (30). MRI showed L2-L3 osteomyelitis with epidural and psoas abscesses. She had diabetes mellitus type II and sideropenic anemia and developed septic shoulder arthritis 18 days prior to first presentation in our institution. The patient underwent posterior instrumentation with pedicle screws and anterior column reconstruction using PEEK cage. Based on sensitivity testing, antibiotics were administered parenterally for 50 days. At the end of antibiotic treatment, patient was discharged symptom free with normal CRP. Seven months after surgery patient presented again with back and right leg pain. CRP was elevated (93) and MRI showed psoas abscesses with osteomyelitis of L4 vertebral body. Another surgery was undertaken with the removal of PEEK cage and L3 pedicle screws. Screws in L2 vertebral body were not loose and were left in situ. Additional pedicle fixation of L1 and L4 resulted in stable construct. L2–L3 interbody space was packed with tricortical graft and cancellous bone obtained from iliac crest. The patient was prescribed intravenous antibiotics for 45 days. Thereafter, she remained symptom-free and without signs of infection.
Patient no. 8, treated for diabetes mellitus type II, presented 10 days after L4–L5 discectomy with deep wound infection. MRI showed disc space infection with highly elevated CRP (296). Patient was treated with decompression and debridement. Based on sensitivity testing, antibiotics were administered parenterally for 60 days resulting in gradual resolution of infection. Five days after discharge, the patient was admitted again due to severe back pain and elevated CRP (55). MRI showed disc space infection with paravertebral abscesses (Figure 4(a)). Pedicle fixation and anterior column reconstruction with PEEK cage were performed (Figure 4(b)). After surgery, antibiotics were administered parenterally for another 6 weeks. During antibiotic treatment, the patient complained of persisting back pain. Six weeks after instrumented fusion, X-rays and CT disclosed screw loosening in L4 and L5 with anterolisthesis of L4 (Figure 4(c) and (d)) and MRI showed multiple abscesses at L4 and L5 with CRP being elevated again (70). The patient underwent another surgery: PEEK cage was removed together with overtly loosened L4 and L5 pedicle screws. L4 and L5 interbody space was packed with autologous bone; segments from L2 to ileum were instrumented (Figure 4(e)). Again antibiotics were administered for 6 weeks resulting in definitive remission of infection.

A 51-year-old female (patient no. 8) with post-discectomy osteomyelitis of L4–L5. T1-weighted MRI image showed paravertebral abscesses (a). X-Rays 1 day postoperatively showed good alignment of L4–L5 vertebral bodies (b). Six weeks postoperatively anterior slip of L4 was seen (c) and CT showed endplate erosions (d). Anteroposterior and lateral X-rays after revision surgery consisting of debridement, PEEK cage removal and L2-ilium instrumentation (e). Intervertebral space of L4-L5 was packed with autologous bone obtained from iliac crest. L4 pedicles were partially resected in order to decompress L4 nerve roots (f).
Discussion
Surgical treatment of spinal osteomyelitis, according to most authors, consists of intervertebral space debridement followed either by anterior column reconstruction with posterior instrumentation or anterior column instrumentation. 1,3,9 –12 The material used for anterior column support has been traditionally autologous structural bone graft 1,3 and more recently titanium cages. 10 –12 In recent years, however, few case series reported usage of PEEK cages in septic spine conditions with altogether less than 50 successfully treated patients. 6 –8,13 Present case series comprises further 15 cases of spinal osteomyelitis with instrumented interbody fusion using PEEK cages. The fusion success rate in present series was 93%, which is in concordance with reports using autologous bone or titanium cages. 10,14,15 Contrary to the previous reports on PEEK cages where positive outcome was noted in all patients, 6 –8,13 our series implies that not every patient could be expected to have favorable result with resolution of infection. Two patients with unfavorable outcome had infection with methicillin-sensitive Staphylococcus aureus and long-standing type II diabetes mellitus treated with insulin. Caution is therefore suggested when treating spinal osteomyelitis with PEEK material in diabetic patients and possibly in other comorbidities, which result in immunologic compromise.
There is ongoing debate about which approach to use in septic spine conditions. Some authors advocate posterior only approach, 16,17 others anterior approach, 18 while some prefer to approach spine from both routes in single 19,20 or two-staged procedure. 12,21 Consensus is also lacking about how many segments to instrument. In present series, single posterior approach was employed with instrumentation of only affected segments, the exception being one thoracic case with four and one lumbar case with three instrumented segments. All patients, who were neurologically intact prior to surgery, were able to walk unaided on first postoperative day and continued rehabilitation without wearing external support. Ability of early rehabilitation with mobilization speaks in favor of single posterior approach addressing as few segments as possible.
The average time to fusion was 7.1 months, which is slightly less than reported in previous studies where time to solid bony fusion ensued from 7.5 months to 8.6 months. 22 –24 Operatively segmental lumbar lordosis could be increased by 5.1° and thoracic kyphosis decreased by 4.7° on average. However, in the course of follow-up, these values regressed to similar amount as preoperatively. Loss of correction, mostly in thoracic and thoracolumbar cases, was also described in other studies due to end plate remodeling. 10,14 In our study, 7 of 9 lumbar cases were post-discectomy infections with inherently different clinical course and natural history from hematogenous spondylodiscitis. This is in accordance with the literature, where previous spine surgery in tertiary centers accounts for 31–39% of pyogenic spondylodiscitis cases. 25,26
There are drawbacks and limits to the present study. The cohort is diverse concerning the location, route of infection, causative microorganism, and sensitivity of pathogens. Furthermore, the study is retrospective in its basis and includes no control group, which enabled only descriptive analysis.
Conclusion
Treatment of pyogenic vertebral osteomyelitis using PEEK cages for anterior column reconstruction presents viable alternative to autologous bone and titanium. Contrary to previous reports, where only good experience was noted with PEEK cages, two failures in our series call for caution when using PEEK cages in pyogenic vertebral osteomyelitis for patients with serious comorbidities.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.