
Abstract
Introduction:
Ankle fractures involving posterior malleolus are disabling injuries if not managed properly. Clinical and functional outcome of ankle fractures involving posterior tibial plafond is significantly worse. Although the surgical approach and techniques to reduce and fix this fracture are well described in the literature, there still seems to be divided consensus among orthopedic surgeons regarding the same.
Methods:
In this case series of eight patients with trimalleolar fractures, a posterolateral approach was used for fixation of posterior malleolus in all the cases. A preoperative computed tomography scan formed an integral part of management of such injuries. The Olerud and Molendar scoring system was employed at 12 months of follow-up to assess the functional outcome. Weight-bearing X-rays were taken to assess for any ankle arthritis.
Results:
The average age of patients was 48.8 years. The most common mode of sustaining injury was twisting of the ankle joint (n = 5). The average time to union and full weight-bearing was 12.8 weeks (range 10–16 weeks). An excellent functional outcome in four patients and a good outcome in the rest of the four patients were obtained at the end of 12 months of follow-up. No significant ankle arthritis or complications were encountered.
Conclusion:
Appropriate preoperative imaging evaluation is an integral part of planning for these complex injuries. The posterolateral approach provides good exposure for appropriate visualization. Stable fixation of posterior malleolus in trimalleolar fractures plays a vital role in obtaining a positive clinical and functional outcome.
Introduction
Ankle fractures constitute a major proportion of injuries received at orthopedic emergencies all over the world. 1 Although the incidence of trimalleolar ankle fractures is comparatively less, nevertheless, these are disabling injuries if not managed appropriately. It is well described in the literature that ankle fractures involving posterior malleolar component tend to do clinically and functionally worse as compared to other ankle fractures. 2
There still seems to be no consensus in the literature on how to evaluate and manage these injuries in a streamlined protocol. Traditionally, it has been the size of the posterior malleolar fragment, which has been the guiding factor to fix these fractures. Recently, studies have stated that anatomical reduction and fixation of the posterior malleolus should be carried out in all cases of trimalleolar fracture irrespective of its size and type to obtain a good clinical and functional outcome. 3
In our study, we conducted a preoperative computed tomography (CT) scan in all our cases to better understand the fracture configuration and plan our fixation. In a recent study, CT scan formed an integral part of pre- and postoperative imaging workup. According to it, the calculation of the fragment size is better on a sagittal CT of the ankle joint rather than only on a plain lateral ankle radiograph. 3
Various techniques and approaches have been described to fix the posterior malleolar component of a trimalleolar fracture. After anatomical reduction and fixation of the lateral malleolus, the posterior malleolus usually reduces by itself in the majority of the acute cases due to ligamentotaxis by the posterior inferior tibiofibular ligament (PITFL). Surgeons taking the fragment size into consideration then fix it in an anteroposterior (AP) direction by percutaneous screws. Various studies have elucidated the disadvantages associated with the AP screw fixation method. 4 –6
Open reduction and fixation of posterior malleolus from a posterior to anterior direction thus making perfect sense to effectively manage these injuries. To achieve the same, the posterolateral approach has been well described in the literature but still does not seem to be very popular among orthopedic surgeons. 7,8 Studies utilizing this approach to fix such fractures are few in number. 6,7,9 –11 Our case series attempts to bridge the knowledge gap in managing these injuries using this approach.
Methods
In this case series, eight adult patients with closed trimalleolar fractures received and managed at our institute from January 2015 to March 2016 were included. Only follow-up compliant patients were included in the study. Patients with open fractures or other associated fractures in the body elsewhere were excluded. Patients with severe preexisting arthritis in the affected ankle joint, limp, or assisted walk due to some previous or ongoing pathology in the hip or knee joint either in ipsilateral or in contralateral limb were excluded from the study.
Initial management was done in the orthopedic emergency area, which included getting standard AP and lateral radiographs of the ankle joint. Distal neurovascular status and clinical signs to exclude compartment syndrome were assessed and documented. Patients with gross ankle dislocation were attempted to be reduced in the emergency itself under sedation after prior consent from the patient and relatives. A below-knee plaster slab was applied to immobilize the joint and analgesics were instituted. The limb was kept elevated to prevent excessive swelling. After routine blood investigations and preanesthesia clearance, patients were posted for surgery. An ankle CT scan was conducted in all cases as part of the preoperative planning. Intravenous 1 g cefazolin was administered 30 min prior to skin incision in the operating room after prior antibiotic sensitivity testing.
Surgical technique
After the induction of appropriate anesthesia, the patient was first made to lie in a prone position on a radiolucent operating table. All bony prominences were well padded. The knees were slightly flexed by positioning a bolster underneath the ankles to obtain good ankle dorsiflexion for fracture reduction. A posterolateral approach was used by making an incision midway between the medial border of the fibula and the lateral border of tendoachilles (Figure 1). The use of a pneumatic tourniquet in the initial part of our surgery was done to identify and isolate the sural nerve and lesser saphenous vein away from the surgical field. The sural nerve courses from medial to lateral part, and at a point 7 cm proximal to the tip of the lateral malleolus, the nerve is on an average 26 mm posterior to the edge of the fibula. 12 Careful soft tissue dissection and protection of the sural nerve is a must to prevent the formation of painful neuromas. The peroneal tendons were retracted further laterally and anteriorly to expose the fibula. The fibular fixation was carried out first. We provisionally fixed the fracture with K-wires and applied a 3.5-mm reconstruction plate or one-third tubular plate in an antiglide fashion over the posterior surface of the fibula. Anatomical reduction of the lateral malleolus usually made the ankle stable and posterior malleolus reduced by itself due to ligamentotaxis by PITFL. The ankle stability was checked intraoperatively by performing a posterior drawer or posterior loading test of the foot with one hand and by stabilizing the distal leg with the other hand. In inadequate reductions or stabilization of the posterior malleolus, a talar subluxation under the distal articular surface was appreciated.

Skin marking showing the incision for the posterolateral approach in between the tendon of tendoachilles and the posterior border of the fibula.
Fixation of posterior malleolus was carried out next. A deep interval between the peroneal tendons laterally and flexor hallucis longus medially (Figure 2) was made, and soft tissue and periosteum were incised from a medial to lateral fashion to avoid injuring the PITFL. Also, care was taken not to injure posterior malleolar vessels, thereby preventing devascularization of the posterior malleolar fragments. The soft tissue, soft callus, and hematoma interposing in the fractured surfaces of the posterior malleolus were cleared with curette and saline irrigation. This was possible by a slight book opening technique in a craniocaudal direction of the posterior malleolus. This is achieved prior to fixation of the lateral malleolus since once stabilized by PITFL in its place the posterior malleolus is comparatively difficult to maneuver. The posterior malleolus was buttressed with a 3.5-mm recon plate, distal radius T-pate, or one-third tubular plate. The fibular translation test was then performed to check for the stability of the syndesmosis and, in none of the cases, we found syndesmosis to be unstable. No syndesmotic fixation was carried out in any of our cases. The posterolateral wound was irrigated, adequate hemostasis was achieved, and closure was performed.
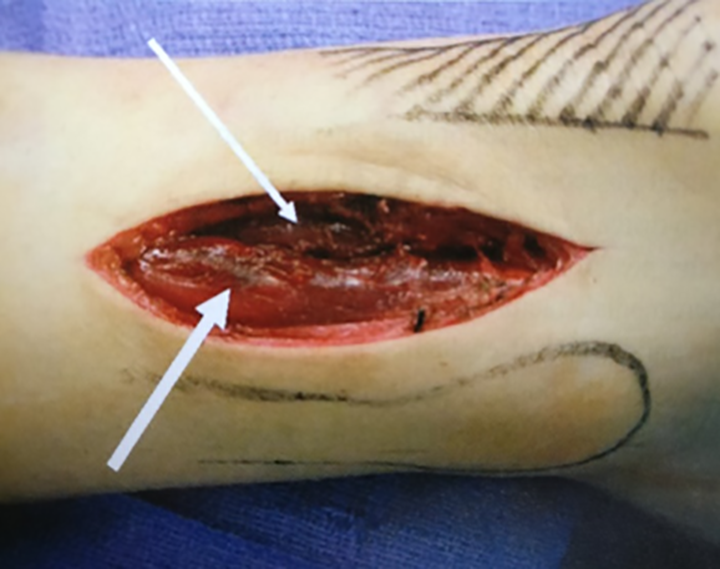
Deep soft tissue interval for posterior malleolus exposure in between peroneus muscles laterally (broad white arrow) and the flexor hallucis longus (narrow white arrow).
The second part of the surgery included fixation of the medial malleolus in the supine position. The part was repainted and redraped. An anteromedial approach was used to expose the medial malleolus, carefully protecting the great saphenous vein. The interposing periosteum was excised and fixation achieved with two 4-mm partially threaded cannulated screws.
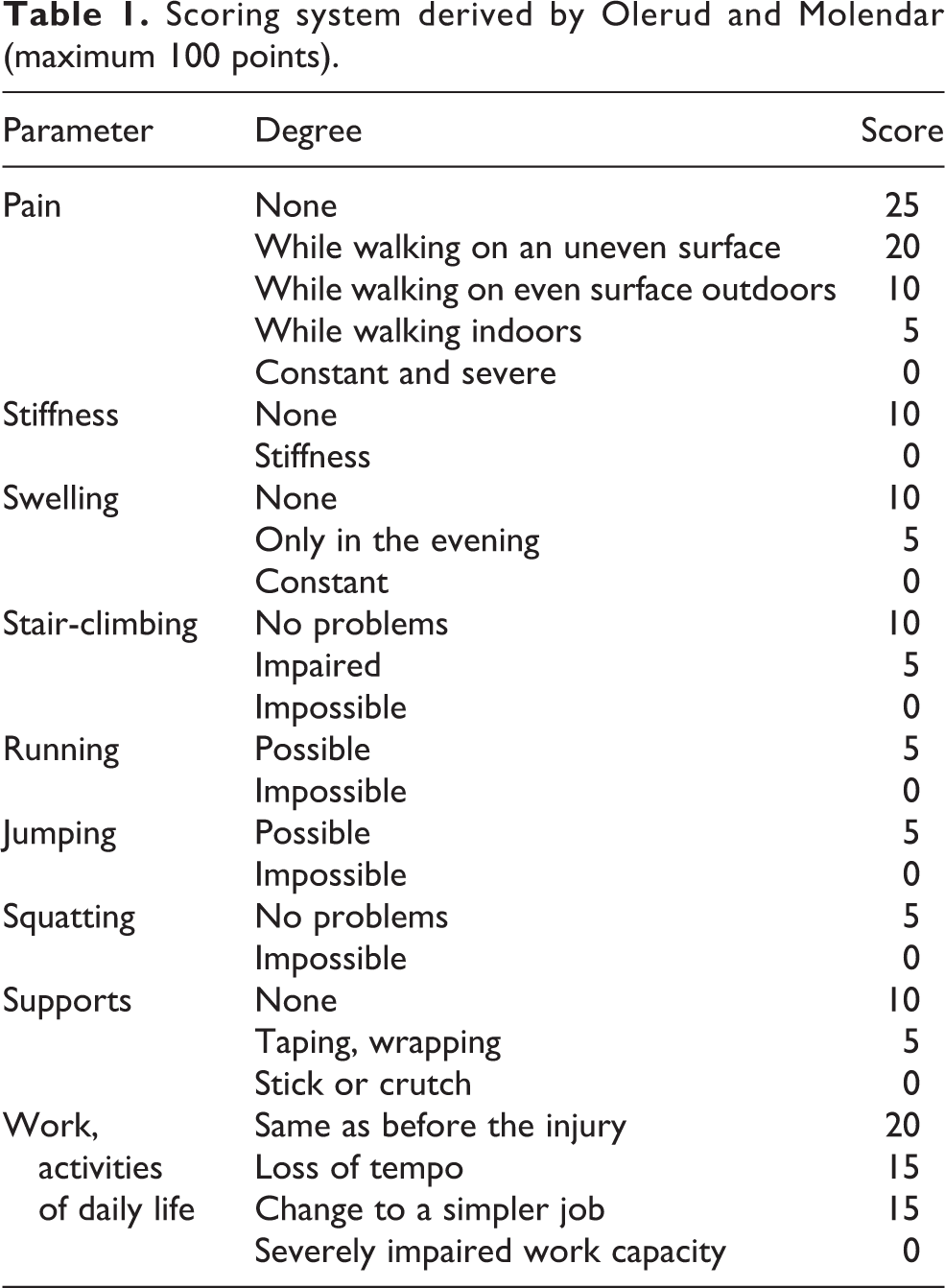
The patient was subsequently discharged after a dressing change at 48 h postsurgery. A below-knee plaster was maintained until 2 weeks postoperatively. Stitch removal and application of a removable boot cast was done at 2 weeks. A strict nonweight-bearing and ankle range of motion (ROM) exercises protocol was maintained until 6 weeks postsurgery. Follow-up at 6 weeks was done when radiographs of the ankle joint were repeated and partial weight-bearing with the help of walking aids was initiated. Regular monthly follow-ups were conducted. Full weight-bearing was started once the clinical and radiological union was achieved. Ankle score, according to Olerud and Molander (Table 1), and ankle arthritis with weight-bearing X-rays at 12 months of follow-up were documented in all cases. 13,14
Scoring system derived by Olerud and Molendar (maximum 100 points).
Results
Eight adult patients with an average age of 48.8 years (range 30–62) were followed up prospectively in our case series, of which five were females and three males. The most common mode of sustaining injury was twisting of the ankle joint (n = 5). The size of the posterior malleolar fragment was divided into three categories with the majority (n = 4) classified as having a medium size (25–33%). Two patients each fell into the small (<25%) and large fragment (>33%) variety. Since we performed the surgery in two positions, the average duration of surgery was 102 min. The average blood loss recorded intraoperatively was 103.75 ml. The average time to union and full weight-bearing was 12.8 weeks (range 10–16 weeks). The average percentage of the restoration of ROM as compared to the contralateral ankle at the time of union was 90.8% of dorsiflexion, 95% of plantar flexion, 86% of inversion, and 87.3% of eversion. An excellent outcome in four patients and a good outcome in the rest of the four patients at the end of 12 months follow-up were concluded according to the Olerud and Molendar scoring system (Table 1). Bargon criteria for grading post-traumatic arthritis of the ankle joint at the end of 12 months with the help of weight-bearing ankle X-rays were assessed. 14 Only one patient had grade 2 arthritis, three patients had grade 1, while the rest (n = 4) had grade 0 arthritis. No complications related to soft tissue healing, pain, or hardware impingement or breakage were encountered.
Discussion
Ankle fractures involving the posterior malleolus are usually the result of a supination-exorotation or a pronation-exorotation form of injury. In majority of our cases, it was a typical Weber B or Lauge-Hansen supination-exorotation form. According to the mechanics of such an injury, the posterior malleolus fragment is an avulsion fracture due to rupture of the PITFL. It constitutes stage 3 of the injury pattern to the ankle ring after involving the rupture of the anterior tibiofibular ligament (stage 1) and an oblique fracture of the distal fibula (stage 2). The rupture of the medial collateral ligament causing medial malleolus avulsion is stage 4, with the fracture line being transverse and in majority below the superior tibiotalar joint line. Since the syndesmosis of the ankle ring is stabilized mainly by the PITFL and the apex of the fibular fracture is mainly posterior or posterolateral in such injuries, stabilization from the posterior side becomes paramount.
Traditionally, small posterior malleolus fractures have been treated conservatively. 15 Fixation, if involvement is more than one-third of the distal articular surface (33%), has been the norm for long. 16 There have been studies which put this figure at 25% and one study which puts 10% as the cutoff limit. 17,18 Cadaveric and biomechanical studies too have been inconclusive to find the posterior malleolar fragment size requiring fixation or whether to leave it untouched. 19,20 We, in our study, followed a protocol to anatomically reduce and fix the posterior malleolus fragment in all our cases. This method is well supported in the recent literature too. 3,21 In all our cases, after fixation of the lateral malleolus, we performed a posterior loading test intraoperatively to see for the stability of the ankle joint. In one case where the size of the posterior malleolus was small (<25%), some posterior subluxation of the talus under the distal articular surface could be appreciated. While in certain cases where the fragment size was larger (>25%), no residual instability was present after lateral malleolus fixation. The quality of lateral malleolus reduction and fixation was judged to be satisfactory in all cases before performing this test. This reiterates the fact that good posterior malleolus reduction and fixation should be obtained in trimalleolar fractures irrespective of its size and type.
Preoperative imaging and evaluation of trimalleolar fracture demand equal attention as would any articular fracture. For long, only AP view (Figure 3) and lateral view ankle X-rays (Figure 4) had been the workhorse to diagnose and subsequently follow-up these cases. An ankle CT scan formed an essential component of our preoperative assessment. Fracture anatomy, configuration, articular step-offs, osteochondral fragments (Figure 5), and fracture apexes were all studied. The sagittal, coronal, and axial cuts helped us in a better understanding of the same. The Volkmann’s fragment and any comminution of the posterior malleolus (Figure 6) were delineated. 22,23

AP radiograph of the ankle joint showing a fracture of the medial and lateral malleoli with increased medial clear space of the tibiotalar joint. AP: anteroposterior.

Lateral radiograph of the same ankle showing ankle subluxation with fracture of the posterior malleolus, thus constituting a trimalleolar fracture dislocation.

Sagittal CT image showing an osteochondral fragment (blue arrow). CT: computed tomography.

Axial CT image showing posterior malleolus size and comminution. CT: computed tomography.
The posterolateral surgical approach was used to fix the lateral malleolus followed by the posterior malleolus component. It is well described in the literature but does not seem to be much favored among the trauma surgeons. 7,8 The possible reasons for this could be (a) prone or lateral positioning for this approach making medial malleolus fixation difficult, (b) possible danger of injuring the sural nerve leading to painful neuromas, (c) time-consuming, since many surgeons are of the opinion that the entire fixation could be performed in the easier supine position, and (d) not many orthopedic surgeons being conversant with this technique.
We agree with the argument of time consumption (average duration of surgery = 102 min), since we performed the surgery in two positions, first, fixation of the lateral and posterior malleoli was done in the prone position and then in the supine position, we fixed the medial malleolus. In certain studies, all fixations have been performed in prone position itself but a certain amount of difficulty in fixing medial malleolus, with improper fixations and sometimes failing to recognize the fragment itself, has also been reported. 4 The use of tourniquet in the initial part of the surgery and careful soft tissue dissection to identify and isolate the sural nerve helped us in obtaining good results.
Good clinical and functional outcome was reported in all our eight cases with fixation of the lateral malleolus by the application of plate on the posterior surface. Many biomechanical studies have also recognized the advantages of posterior plating of fibula as compared to plating the fibula over the lateral surface. 24 However, one study has found no significant difference. 25 We observed that the apex of the fibular fracture was posterior or posterolateral in the majority of such injuries (Figure 7), and we believe that the application of the plate over the fracture apex is biomechanically much superior.

A 3-D reconstruction CT image of the ankle joint showing a trimalleolar fracture with the apex of the fibular fracture located posteriorly. CT: computed tomography.
We believe that posterior malleolus fixation by buttress plates and interfragmentary screws from posterior to anterior direction played a significant role in obtaining good outcomes (Figures 8 and 9). Recognizing these fractures having a vertical shear nature, providing strong fixation with the help of a buttress plate, becomes pivotal. Ankle joint being a weight-bearing axially loaded joint demands rigid fixation for early weight-bearing.

Six-week follow-up X-rays ((a) AP and (b) lateral view) of a trimalleolar ankle fracture with all fragments fixed. AP: anteroposterior.

Fourteen weeks fof ollow-up ankle X-rays ((a) AP and (b) lateral view) showing the fracture well united. Full weight-bearing walk was initiated by this time. AP: anteroposterior.
Fixing by AP percutaneous screws has its own set of disadvantages, which is well supported in the literature. Firstly, it is difficult to fix smaller fragments of posterior malleolus by this technique. Secondly, achieving reduction and monitoring direction of the screws under fluoroscopy is relatively difficult to judge. Thirdly, the nature of the injury has a vertical shear component, which is not biomechanically tackled by screws alone. 5,7,9
Stable fixation of posterior malleolus by plates also has the advantage of making the syndesmosis extremely stable. Fibular translation test was negative in all our cases after fixation of the lateral and posterior malleolus. Additional syndesmotic screw application, thus, becomes unnecessary. 26,27 Thus, problems of syndesmotic screw breakage on early weight-bearing, screw removal, or unstable syndesmosis requiring resurgery for syndesmosis reduction and fixation are circumvented. A study compares patients with trimalleolar ankle fractures in whom the posterior malleolus was fixed with posterolateral buttress plating and had superior clinical outcomes at follow-up compared with those treated with AP screws. 6 There is a proposed multicentre randomised clinical trial comparing the outcome after anatomical reduction and fixation of the posterior fragment via the posterolateral approach or no fixation of the posterior fragment. This trial may help in developing guidelines for the management of such injuries. 28 Only one patient in our case series of eight patients developed grade 2 ankle arthritis at the end of follow-up.
Conclusion
Adequate preoperative imaging, a thorough understanding of the fracture anatomy and biomechanics, and adequate visualization via a proper exposure and stable fixation of all the three components of a trimalleolar fracture play a key role for good clinical and functional outcome in such injuries.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.