
Abstract
Purpose:
This study is aimed to determine the abnormal radiological hallux interphalangeus angle (HIA) range, which can assist surgeons in determining the required bone resection in an Akin osteotomy of the proximal phalanx of the great toe.
Methods:
Radiographs of 141 feet were analyzed. The mean HIA and range were calculated.
Results:
The prevalence of hallux valgus interphalangeus (HVI) deformity was 78% (110/141). The mean HIA was 13.5° ± 4.5° (1.4–24.4). Fifty percent had abnormal HIA values of 10–15°, 40% had values of 15–20°, and 10% had greater than 20°. A large proportion of patients with HVI deformities may need greater than the standard 2–3-mm bone wedge removal during Akin osteotomy.
Conclusion:
The high prevalence and wide range of HVI deformities should alert surgeons to the possibility that greater than 3-mm bone wedge resections may be required.
Keywords
Introduction
Hallux valgus interphalangeus (HVI) is the lateral deviation of the distal phalanx in the great toe. It is measured by the hallux interphalangeus angle (HIA), which is formed from the longitudinal bisections of the proximal and distal phalanges. An angle of up to 10° is considered normal. 1 –3 It is a common finding in the human population and can be seen at birth. 4 In their radiographic review of patients with normal and hallux valgus feet, Strydom et al. 3 found a HVI prevalence of 62.1%, and a study by Kim et al. 5 found a prevalence of 82% in normal feet.
A HVI deformity can put pressure on the second toe, which can lead to further pain and deformity of that toe. Clinically symptomatic HVI can be corrected by a medially based closing wedge proximal phalangeal osteotomy of the big toe, as originally described by Akin in 1925. 6 An Akin osteotomy can be used to treat an isolated HVI deformity, or more commonly, as one component of hallux valgus surgery, particularly in moderate to severe cases or in recurrent deformity. 2,7,8 It is often performed in minimally invasive hallux valgus surgery, and the size of the osteotomy is determined intraoperatively with fluoroscopy or intraoperative imaging. 9 –11 Unlike in arthroplasty, templating in hallux valgus surgery is not routinely used. It is preferable for the amount of bone required for wedge resection to be determined by the surgeon preoperatively using radiographic measurements.
Previous studies have determined mean values of the HIA, but none has defined the abnormal range. 4,5,12,13 The purpose of our study was to define the range of abnormal HIAs in normal feet and to determine the percentage of patients who would require more than a 3-mm wedge resection in a proximal phalangeal osteotomy. By doing so, we aim to help the surgeon become aware of the likelihood of requiring more than the standard 3-mm wedge resection.
Materials and methods
Radiographs
Foot radiographs performed at a single institution from January 2016 to September 2017 were collected. Inclusion criteria consisted of weight-bearing X-rays and age 18 years or older. Exclusion criteria included previous surgery, any injury or fracture, hallux valgus angle (HVA) greater than 15°, any radiographic signs of osteoarthritis in the great toe, or any other visible pathology.
Based on a priori power analysis, 141 radiographs from the same number of patients were included in the study. Each patient was given a numerical identifier to protect confidentiality. The mean age of the patients was 51.7 ± 15.8 (range, 19–87) years, with 53.9% (n = 76) male and 46.1% (n = 65) female. The percentage of left foot X-rays was 47.5% (n = 67), while 52.5% (n = 74) for the right foot.
Measurement of angles
All anteroposterior weight-bearing X-rays were taken with the beam 1 meter from the cassette and angled 15° from vertical and centered on the midfoot. The X-rays were exported to imaging software (Intelerad Medical Systems, Montreal, Quebec, Canada) for analysis.
Two independent observers completed the measurements. The HIA was measured for each X-ray. The mid-diaphyseal axis for the proximal phalanx was measured according to the standardized technique as described by the American Orthopaedic Foot & Ankle Society. 14 A similar technique was used to determine the mid-diaphyseal axis for the distal phalanx (Figure 1).

HIA measurement. Mid-diaphyseal reference points were measured 5 mm from the basal articular surface of the distal phalanx and 5 mm from the tip of the phalanx. These points were used to mark the long axis of the distal phalanx. Mid-diaphyseal reference points 5 mm from the articular surfaces were also used for the proximal phalanx. The angle between the long axes of the distal phalanx and proximal phalanx is the HIA. HIA: hallux interphalangeus angle.
Statistical analysis
Based on previous literature, we assumed that a sample standard deviation of 6° was a conservative upper estimate. 3,5,15 We used this standard deviation of s = 6 to calculate a large enough sample size that guaranteed that we could estimate the population mean with a 95% confidence interval of length ±1°, using the formula mean ± t × s/sqrt(N), where t is the 97.5% quantile of a t-distribution with N − 1 degrees of freedom. This resulted in a necessary sample size of N = 141.
To describe patient demographics, we report the sample mean, the sample standard deviation, 95% confidence intervals for the mean and the range of measured HIAs. To calculate the distribution of the HIA measurements (Figures 2 and 3), we used the default kernel density estimation method in the statistics software R version 3.4.2. To assess the interobserver reliability, we used the icc function in the irr (version 0.85) package in the statistics software R to calculate the intraclass correlation coefficient and corresponding 95% confidence interval as described by Shrout and Fleiss, modelling both the raters and the patients as random effects to estimate the agreement of the raters. 16 To test the mean differences between HIAs of male and female patients, we used a two-sample t-test and to test the mean difference between the two observers we used a paired t-test.

Distribution of all HIAs. HIA: hallux interphalangeus angle; HVI: hallux valgus interphalangeus.
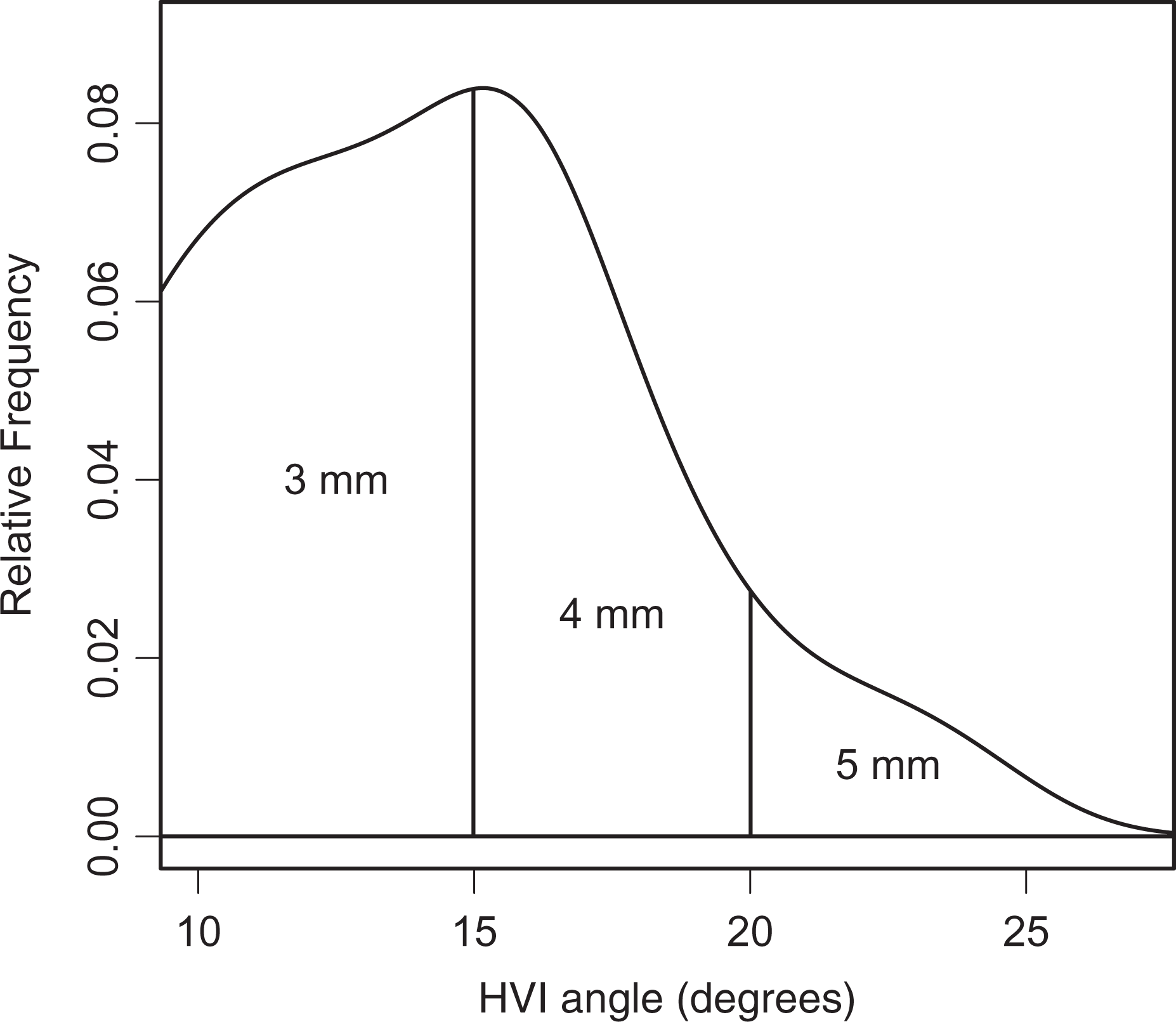
Distribution of abnormal HIAs and corresponding osteotomy size required for correction. HIA: hallux interphalangeus angle; HVI: hallux valgus interphalangeus.
Results
The prevalence of HVI deformity was 78.0%; 110 of 141 radiographs. The mean HIA for all patients was 13.5° ± 4.5° with a range from 1.4° to 24.4°.
The mean HIA for males was 14.0° ± 4.3° (range, 3.2–24.4). The mean HIA for females was 13.0° ± 4.8° (range, 1.4–24.0; Table 1). Though the HIA was larger for males than it was for females, this difference was not statistically significant (p = 0.223).
Hallux valgus interphalangeus angle mean values and range.

CI: confidence interval; SD: standard deviation.
Of the patients who had an abnormal HIA, 50% had a HIA of 10–15°. Forty percent of these patients had a HIA of 15–20°, and 10% had a HIA of greater than 20° (Table 2).
Patients with abnormal HIAs and size of wedge resection required in an Akin osteotomy.

HIA: hallux interphalangeus angle; HVI: hallux valgus interphalangeus.
The intraclass correlation coefficient between the two observers was 0.85 with a 95% CI [0.780, 0.896]. This corresponds with a good correlation. The mean difference between the two observers was 0.82°, which was significant (p = 0.0001), though it was less than 1°.
Discussion
This is the first study to describe the range of abnormal HIAs in normal feet. Previous studies have stated mean values, but none has reported the range. Our prevalence of 78.0% for a HVI deformity in normal feet was higher than that found by Strydom et al. 3 but was similar to Kim et al.’s 5 finding of 82%. Our mean HIA of 13.5° ± 4.5° for all patients was similar to other studies. 4,5,12,13
With a range of 1.4–24.4°, the HIA can be highly variable; but it does form a normal distribution curve (Figure 2).
A HIA of up to 10° is considered normal. Our study indicates that 50% of patients with an abnormal HIA have a HIA between 10° and 15°. We found that there is still a significant number (40%) who have a HIA between 15° and 20°. One in 10 (10%) patients has a HIA of greater than 20°.
Akin osteotomy is performed frequently and is indicated to correct HVI deformities, but it is more commonly done as part of total hallux valgus surgical correction, particularly in moderate to severe or recurrent deformities. In these cases, lateral deviation of the hallux can create pressure on the second toe, so a medial proximal phalangeal closing osteotomy will angulate the hallux away from the second toe. 2 Barouk et al. 7 stated that they perform a proximal phalangeal osteotomy in 90% of cases of hallux valgus correction to treat residual valgus, axial rotation, or excess length of the hallux. We agree with Park et al. 8 in that performing an Akin osteotomy can improve patient satisfaction, as it helps to improve overall cosmesis of the first ray. This is particularly evident in minimally invasive hallux valgus surgery, in which the Akin osteotomy is a vital part of the procedure to achieve greater corrections especially when performing the Chevron osteotomy for severe deformities. 17,18 Shannak et al. 19 stated that an Akin osteotomy can be used to add 10° of correction after a first metatarsal osteotomy, but that corrections greater than 20° could lead to hallux varus and should not be performed. However, based on our findings, larger corrections are to be expected since 10% of those with abnormal HIAs had angles greater than 20°.
Frey et al. 15 derived a trigonometric calculation to determine the amount of angular correction that can be expected from a certain size osteotomy wedge. Shannak et al. 19 expanded upon this idea and used a similar calculation considering the different average widths of the proximal phalanx for males versus females, since the width of the proximal phalanx will change the size of the osteotomy base. Using their calculations as a reference, we can provide a guide as to how much bone to remove during an Akin osteotomy. Though they reported recommended osteotomy sizes for men and women separately, we mainly focused on the female values since hallux valgus and hallux interphalangeus correction surgeries are mainly done in women. Also, we rounded off to the nearest whole number the value of the osteotomy for easier reference. The distribution of abnormal HIAs and the size of the osteotomy base required for correction are shown in Figure 3. The frequency of each osteotomy size that is expected based on our data is shown in Table 2. Based on Shannak et al.’s 19 guidelines and the abnormal HIA range values we obtained, we derived that 50% of patients with a HVI deformity may require a 3-mm osteotomy wedge resection while 40% may need a 4-mm wedge resection. Remarkably, 10% of these patients may require up to a 5-mm osteotomy wedge resection. These findings are important because half of patients with HVI deformity will likely require a 4- or 5-mm wedge resection instead of the usual 2- to 3-mm standard. Knowing the range and distribution of abnormal HIA values in the general population and preoperative measurement of the HIA, the surgeon will be alerted to the possibility of an osteotomy wedge resection greater than 3 mm.
Both under-correction and overcorrection are potential complications of an Akin osteotomy. Recurrence or progression of the deformity is the most common complication and usually occurs if the Akin was performed in the presence of first MTP subluxation or incongruity, as an Akin will not decrease the 1–2 intermetatarsal angle. 2 Additionally, as demonstrated by the Frey et al. 15 and Shannak et al. 19 studies, a small change in the osteotomy base can greatly affect the angular correction. Performing an Akin osteotomy shortens the length of the great toe, as would any closing wedge osteotomy. Therefore, only the minimum amount of bone required for correction ought to be removed, as under- or overcorrection is undesirable and may lead to complications. In open Akin osteotomies, typically a 0.4-mm saw blade is used. Since the saw blade is used twice to make the cuts, this width must be taken into account when considering the total amount of bone removed. In minimally invasive surgery (MIS) for hallux valgus, either a 2 × 12 mm burr or a 3.1 × 13 mm burr is used to complete the Akin osteotomy, and this also must be accounted for. 9,10,17,18 Additionally, since MIS is done under radiographic guidance, these small differences in the size of the osteotomy base could be more difficult to detect. MIS for hallux valgus is known to have a steep learning curve, and this aspect of it may also make it more challenging initially. 20,21 A recent study by Hujazi et al. 22 showed that angular measurements of HIA have an excellent intra- and interobserver reliability for both pre- and post-hallux valgus surgery. Therefore, measuring the HIA preoperatively is highly encouraged and would be essential as it will help the surgeon to anticipate the amount of total correction during hallux valgus surgery.
Conclusion
The findings in this study described the range of HIAs in a normal population and showed that it follows a normal distribution. We also indicated how frequently a 3-mm wedge resection versus a 4- or 5-mm wedge resection is required in Akin osteotomies. It is important to note that our values serve as general guidelines and may need to be adjusted for a proximal phalanx that is narrower or wider than the average. The surgeon ought to measure the HIA preoperatively to be aware of the possibility that larger bone wedge removals might be necessary to achieve adequate correction during an Akin osteotomy procedure. Ultimately, the amount of wedge resection is determined intraoperatively.
Limitation of the study
A limitation to this study is that our data are not entirely representative of all HIAs because we only measured the HIA of patients who had foot X-rays probably due to pain or for other unknown reasons. We did not necessarily include normal, asymptomatic feet in our study. Therefore, our results may not be readily generalizable to the population. However, ours is the first study to report the range of abnormal HIAs. Moreover, pronation of the hallux was not considered in the radiographical measurement of the HIA since feet with HVA of greater than 15° were excluded in the study. Significant pronation of the hallux is usually expected with HVA of 35° or more. 23
Footnotes
Authors’ note
All authors were fully involved in this study and the preparation of the manuscript and the material has not been submitted for publication other than this journal.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.