
Abstract
Purpose:
To compare the long term outcomes of transtibial nonanatomic single-bundle (SB) and double-bundle (DB) anterior cruciate ligament (ACL) reconstruction.
Methods:
Between January 2008 and September 2010, we retrospectively evaluated 377 patients who underwent primary ACL reconstruction and who were available at 8 years of follow-up. Patients who received transtibial nonanatomic SB ACL reconstruction (n = 263) were assigned to group SB and DB ACL reconstruction (n = 114) to group DB. The patients were assessed with the International Knee Documentation Committee (IKDC), the Lysholm scores, Tegner activity score, knee joint stability tests, and patellofemoral osteoarthritis (OA) findings using the Kellgren–Lawrence (K-L) classification. Contralateral ACL (CACL) injury was also evaluated.
Results:
Thirteen patients underwent revision ACL surgery during the follow-up. Ultimately, 256 patients in group SB and 108 patients in group DB were available at the 8-year follow-up. At final follow-up, the IKDC subjective score (p = 0.04) and Lysholm score (p = 0.02) showed significantly superior results in group DB compared to group SB. However, there was no significant difference of Tegner activity score (p = 0.30), range of motion (p = 0.81), and knee joint stability tests. There was significant progression of patellofemoral OA between preoperative and final follow-up in ipsilateral knee of both groups but not significant progression in contralateral knee. However, there was no significant difference between the two groups at the follow-up. There were 2.7% ipsilateral ACL graft failure in group SB, compared with 5.2% in group DB (p = 0.12) and 6.4% CACL tear in group SB, compared with 5.2% in group DB (p = 0.65). The mean survivorship of ACL graft was 9.47 ± 0.05 years (95% confidence interval (CI), 9.36–9.58) in group SB and 9.87 ± 0.16 years (95% CI, 9.54–10.20) in group DB, and there was no significant difference (p = 0.25).
Conclusion:
DB ACL reconstruction resulted in significantly better clinical IKDC subjective scores and Lysholm scores. However, most of the differences in clinical scores were small, and the clinical relevance of this difference is unknown. In addition, there was no significant difference in Tegner activity score, knee joint stability tests, patellofemoral OA, and survivor rate of the ACL graft and CACL after reconstruction after a minimum of 8-year follow-up.
Keywords
Introduction
There have been many changes in the method of anterior cruciate ligament (ACL) reconstruction for decades. While the basic concept of ACL reconstruction method has been changed from isometric to anatomic, efforts to restore the ACL to its original shape and original position as much as possible continue. 1 –5 The anatomy of the ACL has proven to be a controversial subject. 6 The ACL structures reported in most cadaveric studies 7,8 consist of two major functional bundles, the anteromedial bundle and the posterolateral bundle, and many biomechanical and cadaveric studies have shown that anatomic ACL double-bundle (DB) reconstruction restores knee stability more close to normal when compared to the conventional single-bundle (SB) ACL reconstruction. 9 –11 Based on this, many surgeons used the DB technique to restore the original ACL. Many comparative clinical studies 9,11,12 also reported similar or superior clinical outcomes in DB ACL reconstruction, but there is still a question as to what the clinical differences in the various studies may have on the patient. Most of the studies reported are short-term comparative studies of SB and DB techniques with short-term follow-up within 1–5 years, and there have been only three trials 3,10,13 of mid- to long-term follow-up (8–10 years) research, thus a long-term follow-up study is relatively scarce. Furthermore, compared cases in most published clinical studies used different surgical techniques for SB and DB ACL reconstructions, which makes it difficult to compare those methods fairly. A recent long-term study by Jarvela et al. 3 also compared the anatomic DB technique with the conventional SB technique, but it was difficult to have an exact comparison dependent on the bundle type.
Thus the purpose of this study was to compare the clinical outcomes of transtibial nonanatomic SB ACL reconstruction and DB ACL reconstruction with long-term follow-up of a large single-surgeon series, and to evaluate the survival rate and the progression of osteoarthritis (OA) of the ipsilateral knee and that of the contralateral knee by a long-term follow-up study. Our hypothesis was that DB ACL reconstruction would result in better clinical outcomes, less patellofemoral OA, less graft failure rate, and a higher survivor rate of the ACL graft and contralateral ACL (CACL) after reconstruction than the SB ACL reconstruction.
Material and methods
After institutional review board approval, we evaluated 453 consecutive patients who underwent primary ACL reconstruction between January 2008 and September 2010. Patients who were included in the study had received primary ACL reconstruction due to an isolated ACL tear. The diagnosis of an ACL tear was confirmed by physical examination and magnetic resonance imaging (MRI). Exclusion criteria included patients who had multiple ligamentous injuries (n = 15), contralateral knee surgery before the index surgery (n = 11), and growth plate involvement (n = 20). Therefore, 407 patients were enrolled in the study. Of 407 patients, 377 patients were able to follow up for more than 8 years. All the surgical procedures were performed by a single surgeon.
Of 377 patients, 263 who underwent SB ACL reconstruction were assigned randomly to group SB and 114 who underwent DB ACL reconstruction were assigned to group DB. Thirteen patients (7 in the SB group, 6 in the DB group) had a graft failure during the follow-up and underwent revision ACL surgery. Ultimately, 256 patients in group SB and 108 patients in group DB were available at the 8-year follow-up.
There were no significant differences between the two groups with regard to age at surgery, sex, time since injury, associated meniscal injury, and follow-up time (Table 1).
Demographics and baseline data for the ACL reconstruction cohort (n = 377).

ACL: anterior cruciate ligament; SB: single-bundle; DB: double-bundle; SD: standard deviation.
Surgical technique
The surgical technique of the double-bundle method has been described earlier in detail by Yoon. 2 In all cases, autologous hamstring tendon was used, and it was harvested on the ipsilateral side of the knee joint using a stripper. For SB reconstruction, the semitendinosus and gracilis tendons were harvested. Autohamstring graft diameter used was only 8 or 9 mm. For a DB reconstruction, only the semitendinosus tendon was harvested and it was used for the posterolateral (PL) bundle reconstruction. Semitendinosus autograft diameter was 6 mm, anterior tibialis allograft diameter was 6 mm. Besides, the anterior tibialis tendon allograft was used for the AM bundle reconstruction. Each graft was trimmed to the appropriate diameter. The ACL tibial guide (Mitek, Norderstedt, Germany), with the angle set at 45°, was used to pass a guide pin. In all the surgical procedures, a transtibial technique was used and bony notchplasty was not performed.
In SB ACL reconstruction, the tibial tunnel was located the center of the ACL tibial footprint. The femoral tunnel was located between 10:00 and 11:00 direction for a right knee joint (between 01:00 and 02:00 direction for a left knee joint). Graft tendon was fixed on the femoral side with a bioabsorbable pin (Rigidfix cross-pin system; DePuy Mitek, Raynham, Massachusetts, USA). The grafted tendon was fixed at 30° of flexion using cancellous screws and spiked washers or staples and was double fixed with bioabsorbable interference screws suitable for the diameter of the tunnel.
In DB ACL reconstruction, the two locations of tibial tunnel were located the insertion sites of the ACL tibial footprint. The femoral tunnel was located 11:00 direction of the intercondylar clock, 6 mm anterior to the posterior bony edge of the lateral wall with arthroscopic observation from the anteromedial portal for right knee joint (01:00 direction for a left knee joint) in an AM bundle, and 10:00 direction of the intercondylar clock, 6 mm anterior to the posterior bony edge of the lateral wall with arthroscopic observation from the anteromedial portal for a right knee joint (02:00 direction for a left knee joint) in a PL bundle. The AM bundle was fixed with a biodegradable pin (Rigidfix cross-pin system) and the PL bundle was fixed to the lateral femoral cortical bone with EndoButton CL (Smith & Nephew, Andover, Massachusetts, USA) on the femoral side. On the tibial side, with the knee joint at 30° of flexion, both bundles were fixed with a staple. This was followed by a double fixation using a biodegradable interference screw fitted to the diameter of the tunnel.
Postoperative rehabilitation
The rehabilitation protocol was the same for all patients except those who required meniscus repair. From day 1 postoperatively, the early-stage joint movement was initiated using a continuous passive motion machine. Until 3 weeks postoperatively, the patients were restricted to partial weight-bearing. From 6 weeks postoperatively, the patients were allowed to perform a gait without a brace. From 3 months postoperatively, the patients began to jog or swim. From 9 months postoperatively, the patients were allowed to participate completely in sporting activities. In patients who required a meniscus repair, the rehabilitation was modified to exclude weight-bearing activities and 90° knee flexing for the first 6 weeks.
Clinical and stability evaluations
Knee function was assessed by patient’s functional scores, range of motion (ROM) of the knee joint, and knee joint stability evaluation. Functional scores included the International Knee Documentation Committee (IKDC) subjective scores, Lysholm scores, Tegner activity scores and physical examinations performed preoperatively and at final follow-up. The knee joint’s ROM was measured by goniometer. To evaluate knee joint stability, physical examinations which included the anterior drawer test, Lachman test, and pivot shift test were performed and recorded by one senior author who was also blinded to the group allocations. In addition, joint laxity was measured using side-to-side difference in anterior tibial translation on Telos® stress radiographs (Telos, Weiterstadt, Germany).
Radiographic evaluation
Radiographic evaluation was performed preoperatively and at final follow-up with axial patella projection. Patellofemoral OA findings were evaluated using the Kellgren–Lawrence (K-L) classification. 14 OA was defined as a K-L grade of at least 2. A blinded musculoskeletal radiologist conducted the radiological evaluation.
Graft failure
Failure was defined as the need for revision ACL reconstruction (1) for complete tear of ACL graft, specifically including complete tear of ACL graft seen on MRI, and (2) for instability with pivot shift test grade 2 or 3 results compatible with the failure of graft.
Statistical methods
All statistical analyses were performed with SPSS version 17.0 (SPSS). Quantitative variables were presented as mean and standard deviation or median and interquartile range. The χ 2 test and Fisher’s exact test were used to compare qualitative variables, and quantitative variables were compared using the independent t test for normally distributed continuous variables, or Mann–Whitney U test; the distribution of our quantitative variables was not normal. For preoperative and postoperative comparisons of dependent variables, the paired-samples t test was utilized for normally distributed data, and the Wilcoxon signed-rank test was utilized for nonnormally distributed data. Differences with p values <0.05 were considered statistically significant, and the results were expressed with a 95% confidence interval (CI). A power analysis was performed to determine the sample size for the current study. Survival analysis was performed by the Kaplan–Meier method. The log-rank test (Mantel–Cox, 95% CI) was applied to determine if there was a statistical difference between the two curves. A p value <0.05 was considered as statistically significant.
Results
Clinical scores
In both groups, the mean IKDC subjective scores, Lysholm scores, and Tegner activity scores were significantly improved postoperatively compared to pre-operation. In preoperative clinical scores, there were no significant differences regarding the IKDC subjective score, Lysholm score, and Tegner activity score between the two groups (Table 2). Also, there was no significant differences regarding Tegner activity score at final follow-up. However, at final follow-up the IKDC subjective score and Lysholm score showed significantly superior results in group DB compared to group SB. However, these differences were small and may not be clinical relevant.
Comparison of preoperative and the latest follow-up clinical scores (n = 364).

SB: single-bundle; DB: double-bundle.
aInternational Knee Documentation Committee.
Range of motion
The mean ROM was 130.7° ± 26.1° in SB group and 132.4° ± 19.7° in DB group preoperatively. After ACL-R, it was 144.1° ± 9.6° and 142.7° ± 7.4°, respectively. There was no significant difference in the mean angle of joint movement (p = 0.81). There was no case of limitation of ROM at final follow-up.
Knee joint stability
In both groups, the anterior drawer test, Lachman test, pivot shift test, and side-to-side difference in anterior tibial translation on Telos stress radiographs significantly improved postoperatively (Table 3). However, comparing the two groups, a significant difference was not observed preoperatively or when these evaluations were repeated at final follow-up.
Preoperative and the latest follow-up in knee joint stability.

SB: single-bundle; DB: double-bundle.
aSignificance was determined with use of Student’s t-test.
bSignificance was determined with use of paired t-test.
cThe values are given as the mean and the standard deviation.
The preoperative and postoperative clinical data at final follow-up are summarized in Table 3.
Patellofemoral OA
None of the patients had patellofemoral OA (K-L grade of at least 2) either in the operated knee or in the contralateral knee preoperatively. In the operated knee, at final follow-up, OA (K-L grade of at least 2) in the patellofemoral compartment was identified in 13.6% in group SB and 12.9% in group DB. There was significant progression of patellofemoral OA between preoperative and final follow-up outcome in both groups; however, there was no significant difference between the two groups (Table 4). In the contralateral knee, at final follow-up, OA in the patellofemoral compartment was identified in 1.8% in group SB and 0.9% in group DB. There was no significant progression of patellofemoral OA between preoperative and final follow-up outcome in both groups (Table 4). No significant group difference was found at final follow-up, and also no significant difference between preoperative and postoperative patellofemoral OA changes in both SB and DB.
Comparison of patellofemoral osteoarthritis (K-L grade).
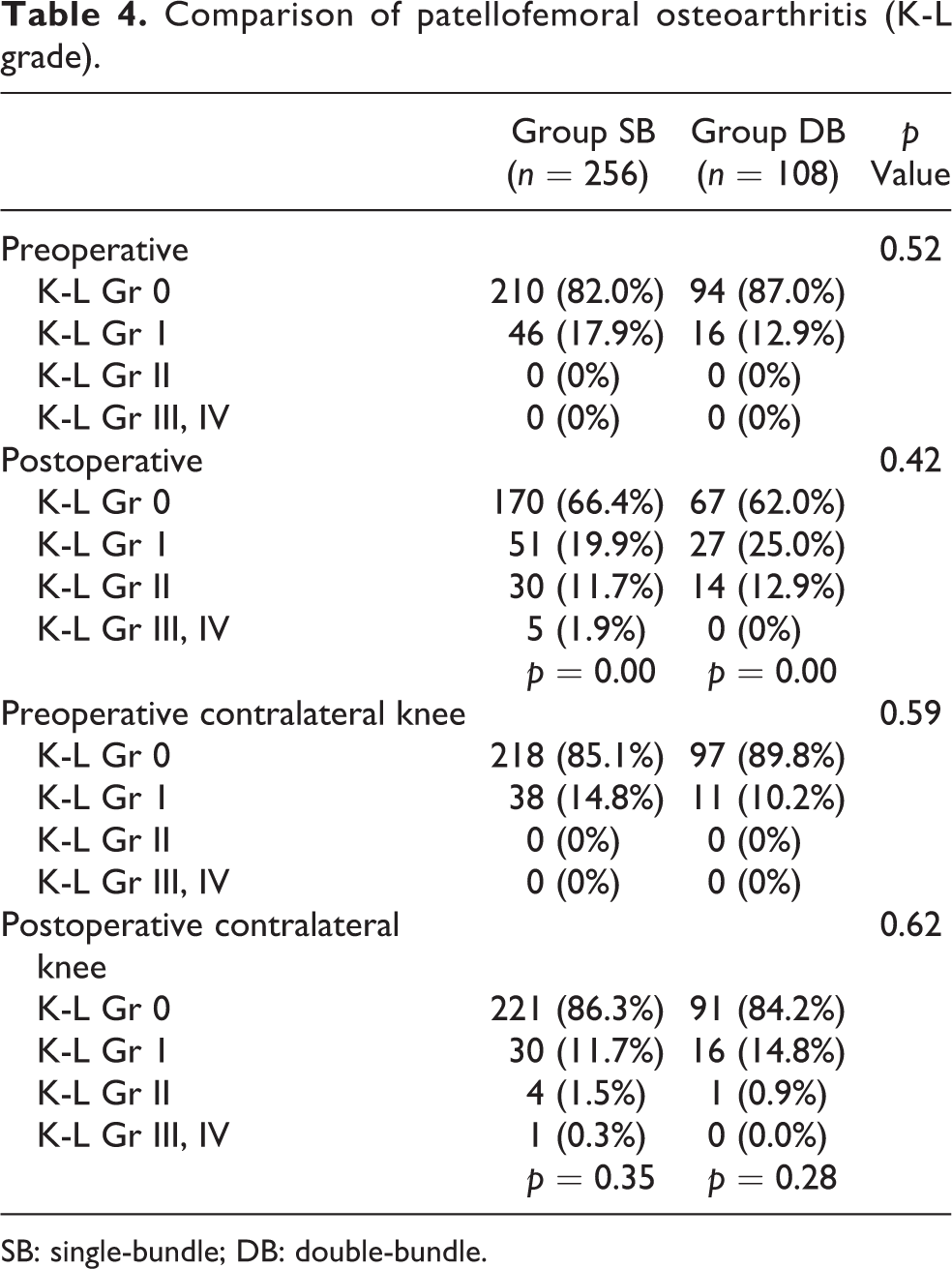
SB: single-bundle; DB: double-bundle.
Failure
We had seven failures in group SB (2.7%) and six failures in group DB (5.2%). Characteristics of failed ACL reconstruction are summarized in Table 5. However, there was no significant difference in the graft failure rate between groups (p = 0.12). The mean time to failure for group SB was 48.3 ± 10.5 months compared to 28.6 ± 4.7 months for group DB. More than 5 years after surgery, there was no more failure in DB group.
Characteristics of failed anterior cruciate ligament reconstruction.

SB: single-bundle; DB: double-bundle; ACL: anterior cruciate ligament.
aSignificance was determined with use of paired t-test.
bSignificance was determined with use of Student t-test.
Survivorship
Kaplan–Meier survival curves were calculated for failure as the end points (Figures 1 and 2). In groups SB and DB, survival rates of ACL reconstruction surgery were 99.6% and 99.1% at 1 year, 99.2% and 98.2% at 2 years, 98.9% and 94.7% at 5 years, 96.6% and 94.7% at 9 years, respectively. The log-rank test demonstrated no significant difference between the two Kaplan–Meier survival curves (p = 0.25). The mean value with standard deviation for survivor time was 9.47 ± 0.05 years (95% CI, 9.36–9.58) in group SB and 9.87 ± 0.16 years (95% CI, 9.54–10.20) in group DB. The most common time for ACL graft failure in DB group was between 2 and 3 years. After 5 years of ACL reconstruction surgery, there was no incidence of ACL failure in group SB.

Kaplan–Meier survival estimates, with failure of anterior cruciate ligament reconstruction as the end point, demonstrating a projected 96.6% and 94.7% survival overall at 9.47 and 9.87 years in patients with groups SB and DB, respectively. The log-rank test (Mantel–Cox, 95% CI) showed that there was no statistically significant difference between them (p = 0.25). CI: confidence interval; SB: single-bundle; DB: double-bundle.

Kaplan–Meier survival estimates, with contralateral ACL survival as the end point, demonstrating a projected 93.5% and 94.7% survival overall at 9.24 and 9.78 years in patients with groups SB and DB, respectively. The log-rank test (Mantel–Cox, 95% CI) showed that there was no statistically significant difference between them (p = 0.69). CI: confidence interval; SB: single-bundle; DB: double-bundle; ACL: anterior cruciate ligament.
CACL injury
CACL tear was confirmed at the time of CACL reconstruction. There are 17 CACL tears in group SB (6.4%) and 6 in group DB (5.2%) by trauma. The mean time to CACL tear was 50.0 ± 26.6 months in group SB and 19.2 ± 8.4 months in group DB. In the CACL injury, CACL survival rates were 99.6% and 95.6% at 1 year, 98.5% and 95.6% at 2 years, 96.2% and 94.7% at 5 years, 93.5% and 94.7% at 9 years in group SB and group DB, respectively (Figure 2). The mean value with standard deviation for CACL survivor time was 9.24 ± 0.09 years (95% CI, 9.07–9.42) in group SB and 9.78 ± 0.20 years (95% CI, 9.39–10.18) in group DB. The most common time for CACL injury in DB group was within 1 year.
Discussion
After long-term follow-up, the main finding of our study was that ACL reconstruction using either SB or DB had satisfactory clinical outcomes and cumulative failure rates. In addition, no statistically significant differences were found in the outcomes between SB and DB ACL reconstruction. Our hypothesis was partially validated because two subjective findings were significantly better in group DB than group SB. Conversely, there were no significant differences in the knee joint stability, patellofemoral OA, and survivorship of the ACL graft and CACL after reconstruction.
Regarding clinical scores, significantly higher IKDC subjective scores and Lysholm scores were found in group DB but no significant difference in Tegner activity scores was found between SB and DB ACL reconstruction. Moreover, there was no significant difference in ROM and knee joint stability tests between SB and DB ACL reconstruction. Most of the differences in clinical scores were small, and the clinical relevance of this difference is unknown.
In our study, which had a minimum of 8-year follow-up, OA in patellofemoral joint of the operated knee was present in 13.8% of all patients and was not significantly different between the two groups.
However, Gong et al. 15 showed that the DB technique resulted in significantly fewer cartilage lesions on femoral groove at second-look arthroscopic surgery 18 months after the primary ACL reconstruction than the SB technique. Moreover, Tajima et al. 16 previously reported this in a cadaveric study. However, we evaluated the long-term progression of patellofemoral joint OA after ACL reconstruction. Patellofemoral joint OA after ACL reconstruction has been mostly unrecognized. 17,18 In recent studies, Yoon et al. 19 and Jarvela et al. 3 showed that the reconstruction technique has only a small effect on OA progression, so our finding is in line with the previous finding. We also found that ACL reconstruction has little effect on contralateral patellofemoral joint OA progression. When mild OA change is found in the contralateral knee, there is a possibility that progression of patellofemoral and cartilage degeneration might be attributed to normal age-dependent joint degeneration.
In our study, we also found lower rates of graft failure for SB compared with DB ACL reconstruction. The reasons for this are unclear and are contrary to some previous studies. 3,9 Table 5 shows that revision ACL reconstruction due to complete tear of ACL graft was higher in group DB than in group SB, while revision ACL reconstruction due to instability was higher in group SB than in group DB. This is in accordance with many recent papers 3,20 –22 that the patients who undergo DB ACL reconstruction may have some advantages in knee kinematics. Because the two grafts cross each other inside the joint, acting separately at different knee angles, they mimic the normal ACL anatomy more closely than a single graft. 3 Nevertheless, our long-term study showed no significant differences in failure rate and overall survival between the groups.
To our knowledge, this is the first mid- to long-term survival study on CACL injury and DB ACL reconstruction. Our study showed no significant differences in CACL tear rate, time to index surgery, and overall survival (Table 5). Specifically, 5 of 6 CACL tears (83.3%) were within 2 years in group DB, while in group SB, only 1 of 17 CACL tears (5.8%) was within 1 year and 6 of 17 (35.2%) were within 2 years from index surgery. We found 58.8% of CACL tears to be between 1 and 5 years after surgery in group SB. The exploration for this phenomenon is unclear.
Many previous studies 3,9,20 have shown results similar to ours. There was no significant difference in clinical outcome between the DB and SB ACL reconstruction, and there were no significant differences in many aspects including failure rate, survivorship, and occurrence of OA in our long-term follow-up study. In fact, recently published studies on the shape of the ACL fiber describe the ACL fiber as a single flat bundle that extends like a ribbon as reported by Smigielski et al. 4 rather than a DB. Some authors have reported that the ACL fans out toward the femoral and tibial insertions, with the cross-sectional areas of the insertions being larger than that of the midsubstance. 5,23,24 This assertion implies it is more important to restore the origin and insertion of the original position than to focus on the number of bundles in the native anatomic morphology of the ACL fiber during ACL reconstruction, which is based on older research results.
This study had several limitations. The major limitation is that it is a retrospective study. However, unlike other retrospective studies, 3,11,24 our approach was limited to the bundle type (conventional SB technique and nonanatomic DB technique), which put the focus on the effect of bundle type on surgical outcome. Potentially important patient-related factors that can affect the outcome of the surgery were compared in demographics, and, because no significant difference was observed between the two large groups, it was possible to conduct this comparative study. To our knowledge, our study is the first to compare the long-term outcome of large-sample size groups operated at a single center by a single surgeon using the same surgical method. A second limitation is that we used allograft with autograft in the DB group, but we used autograft alone in group SB. This could be a potential confounder. In Asian people, the graft diameter of the hamstring tendon autograft is usually less than 8 mm2, therefore we decided to use autograft with allograft in DB group. Third, we evaluated OA progression only in patellofemoral joint. However, the aim of our study was to compare SB and DB techniques and there are more clearly identified factors responsible for OA in the medial and lateral compartments than the number of graft bundles. Most patients had combined meniscus and cartilage lesions, which is commonly observed in ACL injuries. The status of a meniscal tear or meniscectomy might affect the progression of medial and lateral compartment OA of knee. Therefore, we focused on the patellofemoral joint change.
Conclusion
In conclusion, after long-term follow-up, DB ACL reconstruction resulted in significantly better clinical IKDC subjective scores and Lysholm scores. However, most of the differences in clinical scores were small, and the clinical relevance of this difference is unknown.
In addition, there was no significant difference in Tegner activity score, knee joint stability tests, patellofemoral OA, and survivor rate of the ACL graft and CACL after reconstruction after a minimum of 8-year follow-up. The number of ACL bundle fibers does not appear to be a critical factor for success in ACL reconstruction.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.