
Abstract
Purpose:
Soft tissue sarcomas (STSs) of the thigh’s adductor compartment frequently attain a large size before clinical presentation and displace the major neurovascular and lymph structures. We aimed to elucidate the clinical outcome in patients with STS of the thigh’s adductor compartment.
Patients and Methods:
From March 1999 to June 2016, we treated 24 adult patients with primary STS of the thigh’s adductor compartment.
Results:
The mean age at diagnosis was 60 years. There were 13 men and 11 women. The mean follow-up period after the date of the initial treatment was 84 months. The mean tumor size at diagnosis was 13.6 cm. The disease-specific survival was 75.3% at 5 years. Local recurrence was detected in seven patients. The 5-year local recurrence-free rate was 69.9%. The patients with proximal STS had significantly poorer local control, compared to the remaining patients. Twelve (50%) patients developed 14 surgical wound complications. Complications included wound dehiscence (n = 7), infections (n = 6), lymphorrhea (n = 1), wound dehiscence and infection (n = 1), and infection and lymphorrhea (n = 1). Six patients underwent additional surgical treatment. Intraoperative blood loss and operative time were related to the incidence of wound complications. Intraoperative blood loss and operative time in patients with proximal adductor STS were significantly larger than those in the remaining patients.
Conclusion:
We should take care of patients with STS of the thigh’s adductor compartment, especially for proximal adductor STS, because they have a greater risk of local recurrence and wound complications.
Introduction
Patients with large deep soft tissue sarcomas (STSs) have a greater risk of tumor-associated events and mortality. 1,2 STSs of the thigh’s adductor compartment frequently attain a large size before clinical presentation and displace the major neurovascular and lymph structures. When STSs extend to the proximal part of the adductor compartment, the pubic rami or the obturator membrane may be involved, increasing the bleeding risk and enlarging the dead space after tumor resection. 3 Therefore, patients appear to be at greater risk of intra- and postoperative complications. Moore et al. suggested that the anatomic tumor site was an important factor for major wound complications, and that the adductor compartment was the most predisposed site for major wound complications. 4 However, very few reports have looked at STS of the thigh’s adductor compartment. 3 –6 The purpose of this study was to elucidate the clinical outcome in patients with STS of the thigh’s adductor compartment.
Patients and methods
From March 1999 to June 2016, we treated 24 adult patients with primary STS of the thigh’s adductor compartment. Patients presenting with local recurrence at diagnosis were excluded from this study. The pretreatment workup included lung, abdomen, and pelvis computed tomography scans with and without contrast enhancement. The histopathological diagnosis and tumor grade were determined using the French Federation of Cancer Centers Sarcoma Group (FNCLCC) system for all patients and were reviewed and confirmed by independent pathologists. The surgical margin was microscopically evaluated in all patients. Defining a wound complication posed difficulties as a single standard was difficult to apply. A complication requiring further surgical treatment was defined as a major complication in many reports, and this definition was adopted in this study. A moderate wound complication was one associated with purulent discharge, or with wound dehiscence of greater than 2 cm. 5,7,8 Therefore, erythema, seromas without additional complications, and hematomas requiring no treatment were not included in the present study. The study protocol was approved by the institutional review board. The need for an informed consent was waived because of the retrospective nature of this study.
Statistical analysis
The statistical associations of the clinicopathological factors were evaluated using the Mann–Whitney U test for quantitative data, and the χ 2 or Fisher’s exact test for qualitative data. The duration of disease-specific or event-free survival was defined as the interval between the date of initial treatment for the primary tumor and that of death, local recurrence, or metastasis. The survival curves were constructed using the Kaplan–Meier method. The log-rank test was used to compare the survival and event rates. Age and tumor size were investigated as continuous variable with univariate Cox hazard model analysis. A value of p < 0.05 was considered to be significant in all statistical analyses.
Results
Patient’s backgrounds’, tumor, and treatment characteristics
The mean age at diagnosis was 60 years (range, 23–81). There were 13 men and 11 women. Diabetes mellitus was complicated in five patients. The mean follow-up period after the date of the initial treatment was 84 months (range, 15–211). The mean tumor size at diagnosis was 13.6 cm (range, 6–25). Eleven patients had grade 3 sarcomas according to the FNCLCC system and 4 patients had grade 2. We also included nine patients with atypical lipomatous tumor (ALT). The 24 patients were histologically classified as follows: ALT (n = 9), dedifferentiated liposarcoma (n = 4), undifferentiated pleomorphic sarcoma (n = 3), leiomyosarcoma (n = 2), myxofibrosarcoma (n = 2), synovial sarcoma (n = 2), myxoid liposarcoma (n = 1), and extraskeletal osteosarcoma (n = 1). Two patients (leiomyosarcoma and synovial sarcoma) were found to have metastasis at initial presentation. All the 24 patients underwent limb salvage surgery for the primary sarcoma. Wide, marginal, and intralesional resection was acquired in 13, 10, and 1 patient, respectively. In nine patients with ALT, marginal resection was performed in eight patients and wide resection in remaining one patient, whose diagnosis before surgery was dedifferentiated liposarcoma.
Reconstruction after tumor resection was required in two patients. A prosthesis, including a part of the femur, was required after tumor resection in one patient with dedifferentiated liposarcoma because of suspected bone invasion based on the pretreatment examination. Skin graft was required in the remaining one patient. Three of the 24 patients received neoadjuvant and/or adjuvant chemotherapy. Four patients underwent brachytherapy and two received postoperative radiotherapy.
Of the 24 patients, 18 were alive and disease free in December 2016 (last review), 1 was alive with disease, and 5 had died of their disease. The disease-specific survival was 75.3% at 5 years (Figure 1). The disease-specific survival in patients with high-grade STSs was 57.5% at 5 years. Local recurrence was detected in seven patients. The 5-year local recurrence-free rate was 69.9% (Figure 2). When tumor resection was required for proximal muscle attachment, we defined the tumor as proximal adductor STS. On univariate analysis, the patients with proximal STS had significantly poorer local control (n = 10, 5-year local recurrence-free rate: 28.1%), compared to the remaining patients (n = 14, 5-year local recurrence-free rate: 100%). Five of 10 patients with proximal adductor STS developed local recurrence, while 2 of 14 patients with mid-distal adductor STS developed local recurrence (Table 1).

Kaplan–Meier curve showing overall survival in all patients.
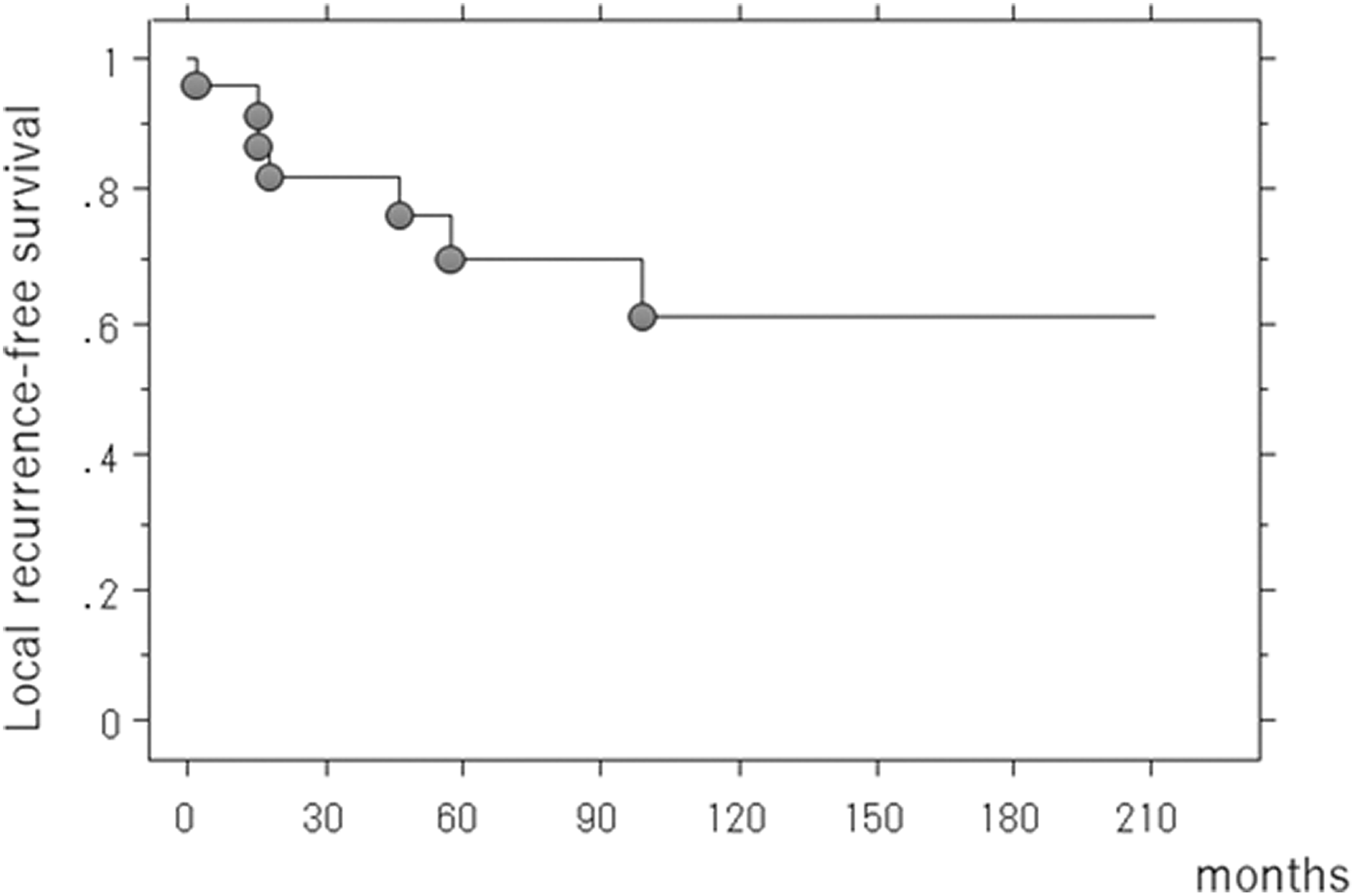
Kaplan–Meier curve showing local recurrence-free rate in all patients.
The prognostic factor for local control.

LRFR: local recurrence-free rate; Rx: radiotherapy; BRT: brachytherapy; CI: confidence interval; STS: soft tissue sarcoma; HR: hazard ratio.
Twelve (50%) patients developed 14 surgical wound complications. The patient’s age, gender, tumor grade, tumor size, duration of drainage, and drainage volume were not related to the incidence of wound complications (Table 2). Intraoperative blood loss (p = 0.03) and operative time (p = 0.02) were related to the incidence of wound complications. Complications included wound dehiscence (n = 7), infections (n = 6), lymphorrhea (n = 1), wound dehiscence and infection (n = 1), and infection and lymphorrhea (n = 1). Six patients underwent additional surgical treatment (Table 3). The cause of additional treatment was wound dehiscence (n = 3), infection (n = 2), and infection and lymphorrhea (n = 1). Five patients recovered by surgical debridement, although one patient underwent hip disarticulation due to infection (Table 3, case 2). Intraoperative blood loss and operative time in the 10 patients with proximal adductor STS were significantly larger than those in the remaining 14 patients.
Analysis of risk factors for wound complications.

DM: diabetes mellitus; Rx: radiotherapy; BRT: brachytherapy.
Characteristics of patients requiring additional surgery.
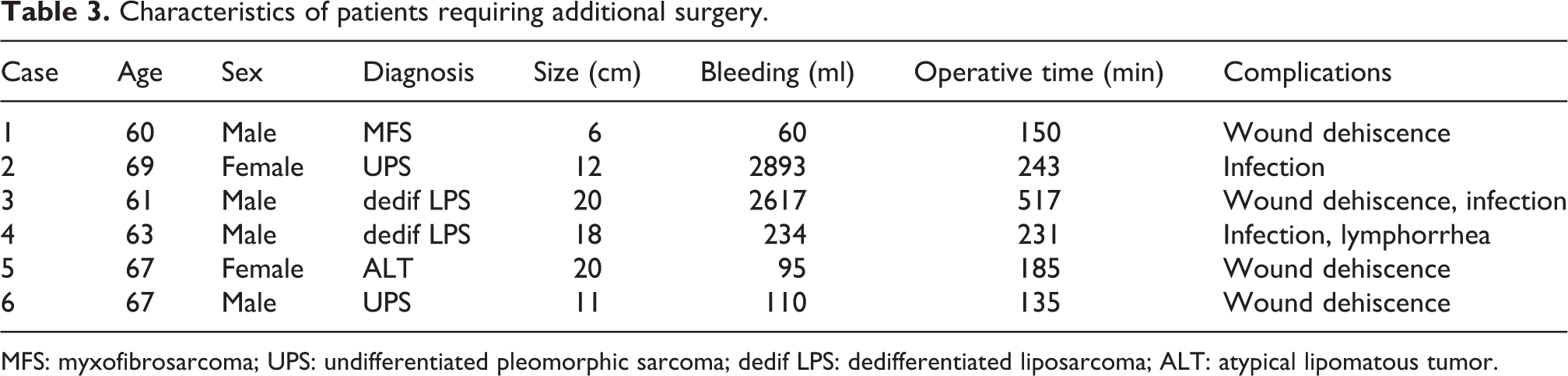
MFS: myxofibrosarcoma; UPS: undifferentiated pleomorphic sarcoma; dedif LPS: dedifferentiated liposarcoma; ALT: atypical lipomatous tumor.
The mean score of Musculoskeletal Tumor Society was 28 (range, 18–30). Walking with T-cane was required in three patients. One received prosthetic replacement after resection of tumor including femur. Another patient received tumor resection including sciatic nerve. The remaining one patient received total knee arthroplasty before tumor resection.
Discussion
Patients with STS of the thigh’s adductor compartment are particularly prone to wound healing complications. Grainger et al. reported that 42.9% of 49 patients developed complications which matched our criteria. 5 The rate of major complications, necessitating surgical treatment, was reported to be between 24.5% and 43% in patients with STS of the thigh’s adductor compartment. 3,5,6 In the present study, 12 (50%) of 24 patients developed wound complications and 6 (25%) required further surgical treatment. Therefore, STS of the thigh’s adductor compartment by itself is a high risk for wound complications. We tried to hypothesize why the adductor compartment of the thigh is at risk of wound complications. First, STSs of the thigh’s adductor compartment are frequently large at clinical presentation. Patients with larger tumors were at higher risk of wound complications because there was a positive correlation between tumor size and major wound complication rate. 4,9,10 In the present study, the mean tumor size was 13.6 cm, and 20 (83%) of the 24 patients had tumors of greater than 10 cm. Second, the lymphatics found in the adductor compartment are particularly vulnerable during surgical dissection, leading to seromas with subsequent infections. 4,11 Finally, STSs of the adductor compartment have specific anatomical characteristics, which displace the major neurovascular bundle. When STSs extend to the proximal part of the adductor compartment, the pubic rami or the obturator membrane may be involved. 3 The obturator artery’s branch and the femoral artery are present in the operative field around the attachment of adductor muscle to the pubis. Therefore, the management of STSs of the adductor compartment, especially when involving the proximal part of the adductor compartment, remains a challenge owing to the high risk of bleeding and the longer operative time. In the present study, intraoperative blood loss and operative time in 10 patients with proximal adductor STS were significantly larger than those in the remaining 14 patients. Duration of wound drainage and total volume drained were not associated with the development of wound complication, in contrast to what was shown previously. To reduce the blood loss intraoperatively, the usage of electronic vessel sealing device was reported in the field of general surgery. 12,13 Recently, electronic vessel sealing device was approved in Japan when we treat STS. We expect the prevention of bleeding using that device. Future study should be necessary to validate it. The introduction of vascularized tissue into the wound has been associated with better wound healing, although this incurs potential donor site morbidity and longer operative time may be an additional risk of surgical complication. 4,5 The low frequency of administration of chemotherapy and radiotherapy did not allow us to analyze this as a risk factor accurately. Our results are consistent with previous finding, 4 demonstrating age was not related to increasing wound complication rates. This may be because our cohort was relatively younger patients (mean 60 years), compared to the population of other cancers.
Concerning functional outcome, most patients had regained full physical function without any support except for three patients. Although Pradhan reported that the functional outcome was significantly worse in patients with wound complications after surgery at adductor STS, additional cases should be necessary to validate it in our cohort. 6
Local recurrence was detected in seven patients. The 5-year local recurrence-free rate was 69.9%. Interestingly, we found that proximal adductor STS had higher risk of local recurrence, although the present study included small sample size. There were no reports which analyzed the relationship between tumor site at adductor compartment and local tumor control, and future study should be necessary on this topic.
Conclusion
Patients with STSs of the thigh’s adductor compartment have a greater risk of tumor-associated events and mortality. Further strategies are necessary to improve the outcome (e.g. chemotherapy, radiotherapy). The limitations of this study include the small sample size and retrospective nature. However, we suggest that we should take care of patients with STS of the thigh’s adductor compartment, especially for proximal adductor STS, because they have a greater risk of tumor-associated events and wound complications.
Footnotes
Author contribution
Koichi Nakamura contributed equally to this study.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.