
Abstract
Purpose:
We aimed to evaluate the clinical results using the pins and rubbers traction system (PRTS) as described by Suzuki et al. for unstable intra-articular fractures of the proximal interphalangeal (PIP) joint and to assess the efficacy and the indication of the technique of the PRTS.
Methods:
Thirty-nine fingers in 39 patients (mean age 46.0 years) with unstable fractures of the PIP joint were treated by the PRTS. The mean interval between injury and surgery was 30.8 days. Active and passive exercise of range of motion of all fingers was started immediately after surgery. Radiographic and clinical results were evaluated at the final examination.
Results:
The mean period the PRTS was applied was 6.4 weeks. The mean follow-up period was 8.9 months. Anatomical union was obtained in all patients. No joint instability, no malunion, nor osteomyelitis was observed. At the final examination, the average active range of motion of the PIP joint was 74.6°. The average Visual Analogue Scale for pain and Quick Disability of Arm, Shoulder, and Hand score were 1.2 and 3.2, respectively.
Conclusions:
The current study demonstrated good results of the PRTS for unstable intra-articular fractures of the PIP joint. Furthermore, satisfactory results were obtained in cases of an incomplete amputation at the PIP joint, a pathological fracture due to bone tumor, and an osteochondral defect due to comminuted fracture of the proximal phalangeal head, where costal osteochondral bone was transplanted. From this study, the PRTS is recommended as a useful treatment because it is widely effective for various unstable fractures of the PIP joint.
Introduction
Comminuted intra-articular fractures of the proximal interphalangeal (PIP) joint and the unstable fracture-dislocations of the PIP joint can often be difficult to treat appropriately and frequently lead to long-term pain, joint stiffness, post-traumatic arthritis, and functional deficit. 1 –14 The ideal goal for treating these comminuted intra-articular fractures of the PIP joint is to achieve anatomical reduction and stable fixation of the fracture fragments combined with traction followed by early mobilization to prevent joint stiffness. 1 –6,8 –10,13 –15 Dynamic external traction systems are considered to be optimal devices to allow both reduction of fracture fragments by capsuloligamentotaxis and early mobilization. 1 –6,8 –10,13 –15
In recent years, various dynamic external traction systems have been reported in the literature to treat these intra-articular fractures of the PIP joint. 14,16,17 The pins and rubbers traction system (PRTS) described by Suzuki et al. in 1994 is one such dynamic external traction system that provides a number of advantages. 14 Suzuki et al. reported good results with adaptation of the PRTS to the intra-articular fracture of the PIP joint and the fracture-dislocations of the PIP joint. 14 Most authors have reported good results and satisfactory functional outcomes after the PRTS use, in many small series, but only for unstable intra-articular fracture of the PIP joint. 1 –6,8 –10,14,15
In the present study, we have used the PRTS not only for these unstable intra-articular fractures of the PIP joint but also for a case of an incomplete amputation at the PIP joint, a pathologic fracture due to bone tumor, and a condylar osteochondral bone defect due to an open proximal phalangeal fracture.
The purpose of this study was to evaluate the clinical results of using the PRTS for various unstable intra-articular fractures of the PIP joint and to reassess the efficacy and the indications of the technique of the PRTS. We consider that the PRTS can be useful and effective for various fractures of the PIP joint, not only to achieve anatomical reduction and stable fixation of the fracture fragments but also to allow for early mobilization to prevent joint stiffness.
Materials and methods
We treated 39 patients with unstable intra-articular fractures of the PIP joint of the finger using the PRTS as described by Suzuki et al. There were 32 men and 7 women, mean age 46.0 (range, 18–77) years at the time of injury. The affected hands were the right in 19 hands and the left in 20 hands. There were 6 fractures in the index finger, 9 in the long finger, 16 in the ring finger, and 8 fractures in the little finger. The etiologies of the injuries were 17 fractures during sports, 11 from falling, 7 crush injuries, and 4 due to traffic accident. We defined cases where the period from injury to surgery was more than 3 weeks as old fractures. There were 24 fresh fractures and 15 old fractures. There were 2 open and 37 closed injuries. Bony mallet fingers were combined in eight cases. The mean interval between injury and surgery was 30.8 days (range, 0–183 days).
We used the Seno classification 18 for the fractures of the base of the middle phalanx and the London classification 19 for the fractures of the condyle of the middle phalanx. There were 13 cases of type 1a (avulsion), 4 cases of type 1b (split), 14 cases of type 1c (split-compression), 1 case of type 2b, 5 cases of type 3 (pilon type) in the Seno classification, and 2 cases of type III in the London classification.
Surgical technique
The technique using the PRTS was almost the same as that described by Suzuki et al. in their original paper (Figure 1). First, a 1.2-mm-diameter Kirschner wire (axial traction pin) was inserted into the center of motion in the head of the proximal phalanx, and a second 1.0-mm-diameter Kirschner wire (hook pin) was inserted into the center of motion in the head of the middle phalanx while under fluoroscopic control. The two wires were bent 90° on both sides of the finger in the direction of the fingertip, very close to the skin. Each end of the first wire was long enough to reach about 3 cm distal to the fingertip. All of the four ends of the wires were bent as a hook. A rubber band, on each side of the finger, connected the axial traction pin with the hook pin, creating a traction force over the PIP joint. We think that rubber bands in size #12 (O’band, Kyowa Ltd, Japan) are very suitable for this technique. In all cases, a single rubber band on each side of the finger was wrapped around the wires twice. In all cases, the third 1.0-mm-diameter Kirschner wire (reduction pin) was transversally inserted through the base of the middle phalanx distal to the fracture to retain correction of a subluxation or dislocation of the PIP joint. According to the direction of dislocation, either dorsal or volar, the reduction pin was placed opposite, either volar or dorsal to the axial traction pin, to counteract the dislocation. The ends of this wire were bent 90°. All the wires must be parallel to the axis of the finger. The distraction at the joint space, the reduction of the small fragments, and the congruency of the PIP joint through a full range of motion were confirmed intraoperatively using fluoroscopy.

Surgical procedure of the PRTS. (a) Insertion of axial traction pin into the center of motion in the head of the proximal phalanx. (b) Insertion of hook pin into the center of motion in the head of the middle phalanx. (c) Insertion of reduction pin through the base of the middle phalanx distal to the fracture. (d) A rubber band, on each side of the finger, connected the axial traction pin with the hook pin. PRTS: pins and rubbers traction system.
Open reduction and internal fixation are necessary if the fragments cannot be kept reduced or if impacted articular fragments remain displaced by longitudinal traction with the PRTS. All old fractures required the open reduction and internal fixation in addition to the PRTS.
In addition to having used the PRTS for these unstable intra-articular fractures of the PIP joint, we also have used it for a case of an incomplete amputation at the PIP joint, a pathologic fracture due to bone tumor, and a condylar osteochondral bone defect due to an open proximal phalangeal fracture.
In the case of the intra-articular comminuted pathologic fracture of the PIP joint due to enchondroma, after curettage of the bone tumor and grafting of artificial bone, the PRTS was fixed without inserting a wire into the bone tumor (Figure 2). In the case of the condylar osteochondral bone defect due to an open intra-articular comminuted fracture-dislocation of the PIP joint, after reconstructing the proximal phalangeal head with a costal osteochondral graft, the PRTS was fixed without inserting a wire into the grafted bone. In both of these cases, the active exercise of range of motion was able to start immediately after surgery (Figure 3).
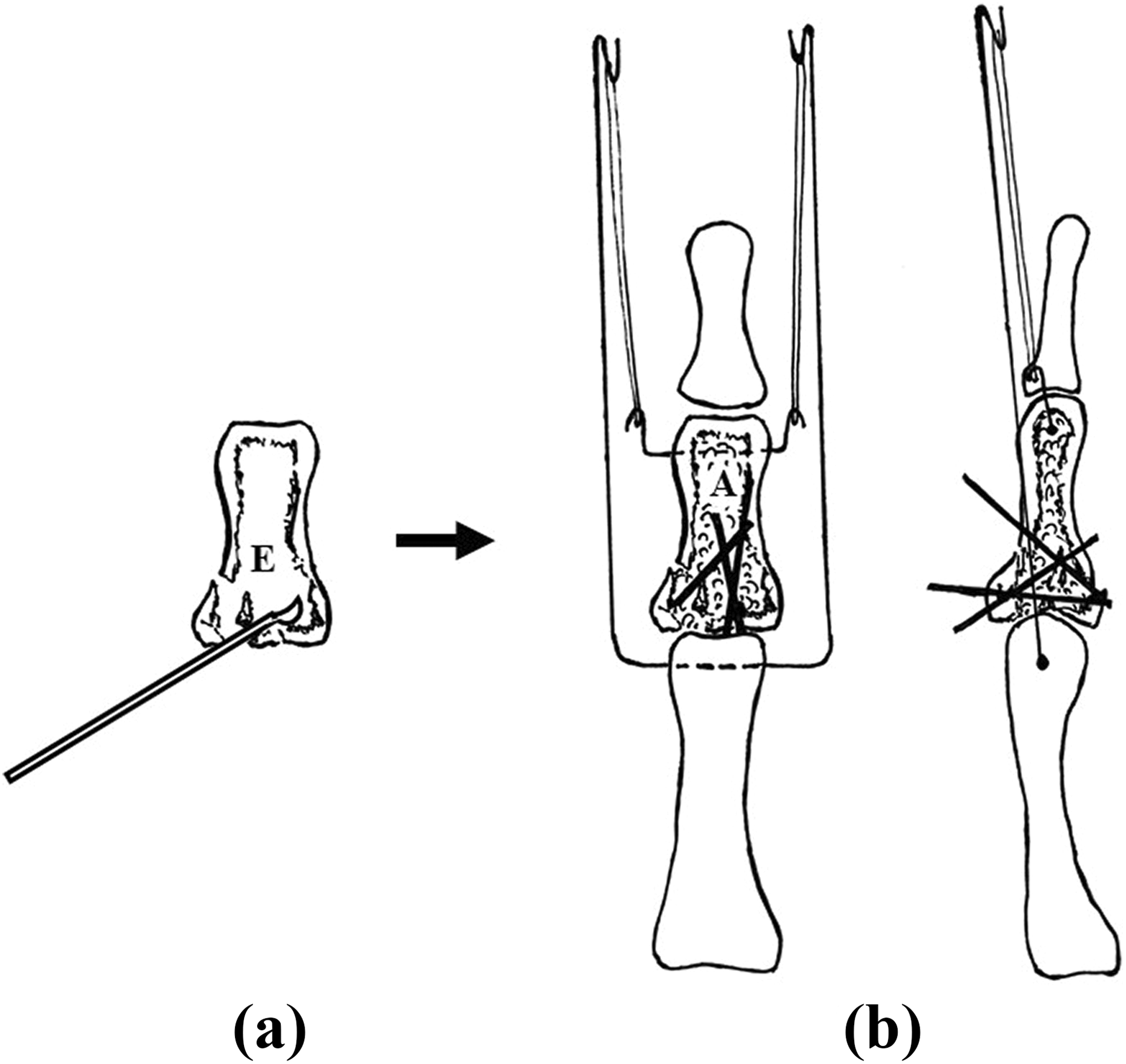
Surgical procedure of the PRTS for the intra-articular comminuted pathologic fracture of the PIP joint due to enchondroma. (a) Curettage of the enchondroma. (b) The PRTS was fixed and internal fixation of the base of the middle phalanx was performed using wires, after grafting of artificial bone. E: enchondroma; A: artificial bone; PRTS: pins and rubbers traction system; PIP: proximal interphalangeal.
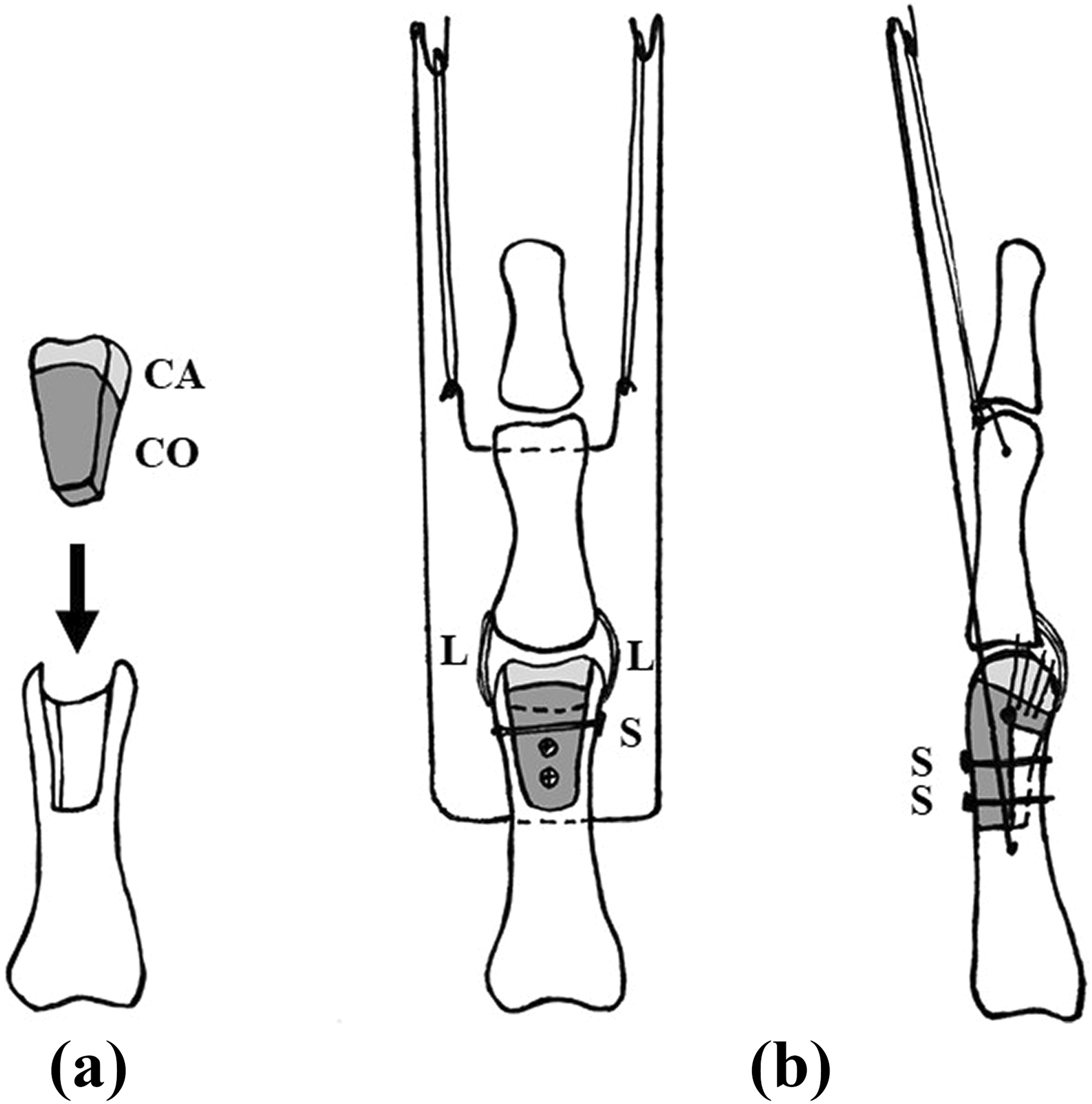
Surgical procedure of the PRTS after reconstructing with costal osteochondral graft for the condylar osteochondral bone defect in the proximal phalangeal head due to an open intra-articular comminuted fracture-dislocation of the PIP joint. (a) Costal osteochondral bone harvested from the fifth right rib was inserted into the osteochondral bone defect in the proximal phalangeal head. (b) The PRTS was attached after fixing the grafted bone with three mini screws. CA: cartilage; CO: cortex; L: collateral ligament; S: screw; PRTS: pins and rubbers traction system; PIP: proximal interphalangeal.
Postoperative treatment
Active and passive exercise of range of motion of all fingers was started immediately after surgery. Patients were also instructed by hand therapists on how to carry out their exercises at home and how to take care of pin-site by self-application of antibiotic ointment using a cotton applicator everyday. Clinical and radiological examinations were taken every week after surgery for 4–8 weeks. The PRTS were removed at 4 to 8 weeks after surgery after obtaining radiographic confirmation of fracture union.
The clinical results obtained after surgery were classified into four categories in accordance with Ishida’s evaluation. 20 For the clinical evaluation after surgery, we used two patient-oriented questionnaires which have been recognized as important tools and which have been widely used for finger injuries: the Japanese Society for Surgery of the Hand version-Quick Disability of Arm, Shoulder, and Hand questionnaire (QuickDASH-JSSH) 21 and the Visual Analogue Scale (VAS). VAS indicates that 0 denotes no pain and 10 denotes worst thinkable pain.
Radiographic and clinical assessments (the active range of motion of the metacarpophalangeal (MP) joint, the PIP joint, and the distal interphalangeal (DIP) joint, and grip strength) were evaluated at the final examination.
Results
All of the radiological and clinical findings were evaluated retrospectively. The mean period of the PRTS application was 6.4 weeks (range, 3–10 weeks). The mean follow-up period was 8.9 months (range, 5–49 months). Limited open reduction and internal fixation after applying the PRTS were performed to reduce the fracture and obtain appropriate congruency of the PIP joint by a midlateral approach in 24 cases. Surgical release of the PIP joint contracture was additionally performed in four cases, and bone graft was needed in six cases.
Anatomical union was obtained in all patients. No re-dislocation, no joint instability, no malunion, nor osteomyelitis was observed. Two cases of pin tract infection were successfully treated with local antisepsis and oral antibiotics without removal of the frame. One of two cases of pin tract infection was old fracture, one case was fresh fracture. Radiologic evidence of post-traumatic osteoarthrosis with joint space narrowing was observed in five cases.
At the final examination, the average active range of motion of the MP joint was 87.5° ± 7.8° (range, extension 0°–10°/flexion 85°–90°). The average active range of motion of the PIP joint was 74.6° ± 16.3° (range, extension/flexion −26° to 0°/66° to 100°). The average active motion of the DIP joint was 45.4° ± 11.7° (range, extension/flexion −10° to 0°/48 to 75°). The average total active range of motion of the finger was 207.0° (range, 168°–235°), 86.3% (70–98%) of the unaffected side. Particularly in fresh fractures, the average active range of motion of the MP joint, the PIP joint, and the DIP joint were 87.3° ± 9.5°, 74.6° ± 19.0°, 46.6° ± 10.9°, respectively. The average total active range of motion of the finger was 208.5°, 86.8% of the unaffected side. Conversely, in old fractures, the average active range of motion of the MP joint, the PIP joint, and the DIP joint were 87.5° ± 6.9°, 73.1° ± 17.2°, 45.0° ± 12.3°, respectively. The average total active range of motion of the finger was 205.7°, 85.7% of the unaffected side. There were no significant differences in active range of motion of the MP joint, the PIP joint, and the DIP joint age between fresh and old fractures. The average grasp strength was 14.2 kg (range, 12.2–25.3 kg), 74.2% (range, 67%–115%) of the unaffected side.
The average VAS for pain in the finger was 1.2 ± 0.9 (range, 0–5) at the final examination. The average quick-DASH score was 3.2 ± 1.2 (range, 0–16.3) at the final examination.
According to Ishida’s evaluation, clinical results were excellent in 8 hands (20.5%), good in 16 hands (41.0%), fair in 13 hands (33.3%), and poor in 2 hands (5.1%) after surgery. The average Ishida score in was 68.1 ± 20.2 (range, 30–100) at the final examination. The two poor cases were of postoperative pin tract infection. They both also had severe comminuted intra-articular fracture of the PIP joint. Their postoperative bone unions were delayed and contracture of the PIP joint occurred. Especially, in fresh and old fractures, clinical results were excellent in 5 and 3 hands, good in 11 and 5 hands, fair in 7 and 6 hands, and poor in 1 and 1 hand, respectively. Moreover, excellent result was observed in a case of an incomplete amputation at the PIP joint, good results were observed in a case of pathologic fracture due to bone tumor and a case of a condylar osteochondral bone defect due to an open proximal phalangeal fracture.
Case
A 22-year-old man sustained an intra-articular open dorsal fracture-dislocation of the PIP joint of his right ring finger in a traffic accident. At the first examination, his right ring finger was incompletely amputated, and the central slip, the lateral bands, the bilateral collateral ligaments attached to a bone fragment, the radial digital nerve and artery, and the joint capsule were ruptured (Figure 4). Radiographs showed an intra-articular dorsal fracture-dislocation of the PIP joint of his right ring finger (Figure 5(a), (b)). On the same day as injury, the PRTS was attached, after bone fragments attached to bilateral collateral ligaments were fixed with wires, the central slip, the lateral bands, the radial digital nerve and artery, and the joint capsule were sutured (Figure 6(a), (b)). The active exercise of range of motion was started immediately after surgery. The PRTS was removed 7 weeks after surgery. At 1 year after surgery, radiographs showed good congruity of the injured PIP joint (Figure 7(a), (b)). The range of motion was 0° to 90° for the MP joint, 0° to 90° for the PIP joint, and 0° to 30° for the DIP joint without pain or instability. He was pleased with the functional results. Clinical results were excellent according to Ishida’s evaluation.
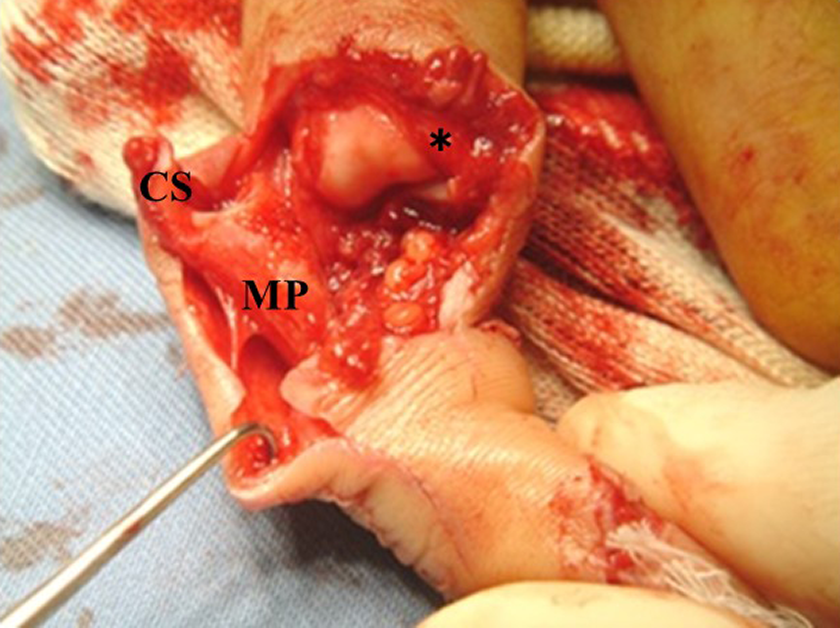
Initial photograph of the right ring finger. The right ring finger was amputated incompletely, and the central slip, the lateral bands, the bilateral collateral ligaments attached to a bone fragment, the radial digital nerve and artery, and the joint capsule were ruptured. MP: the middle phalanx;

Initial radiographs of the right ring finger: posteroanterior view (a), lateral view (b). Initial radiographs show an intra-articular dorsal fracture-dislocation of the PIP joint of the right ring finger. PIP: proximal interphalangeal.

Radiographs of the right ring finger at immediately after surgery: posteroanterior view (a), lateral view (b). Postoperative radiographs of the right ring finger show that the intra-articular dorsal fracture-dislocation of the PIP joint was fixed with the PRTS. PRTS: pins and rubbers traction system; PIP: proximal interphalangeal.

Radiographs of the right ring finger at 1 year after surgery: posteroanterior view (a), lateral view (b). Postoperative radiographs of the right ring finger show good congruity of the injured PIP joints. PIP: proximal interphalangeal.
Discussion
Treatment for unstable comminuted intra-articular fractures or fracture-dislocations of the PIP joints is commonly thought to be problematic and difficult, because these injuries may lead to pain, joint stiffness, instability, and degenerative arthritis. 1 –14,16
Several methods for these unstable fractures of the PIP joint have been reported in the literature including open reduction internal fixation, 15 extension-block pinning, 22 static external fixation, 23 and dynamic external fixation allowing active and/or passive range of motion. 1 –14,17,24 In comminuted fractures of the PIP joint with small articular fragments, fixation by extension-block pinning may not be applicable, and may not be able to maintain the reduction position, especially in old fracture-dislocations. 3,6,10 This pinning has an actual risk of causing joint stiffness following prolonged immobilization, which can be miserable in terms of hand function. 6,8,10 Static external fixation also consistently contributes to joint stiffness and osteoarthritis. 6,7,10 To avoid this, early mobilization is necessary, not only for joint stiffness but also to help the damaged articular cartilage to repair. 25 Suzuki et al. demonstrated that the clinical results could be satisfactory because even slight active motion may encourage the nutrition and remodeling of the articular surface and prevent joint stiffness. 14 Stern et al. reported that open reduction and internal fixation can accomplish anatomical reduction in some cases but should be approached carefully, 26 since extensive soft-tissue dissection around the joint may disturb smaller fragments of their blood supply and lead to joint stiffness. 26 As an alternative, a traction dynamic external system which can keep accurate alignment of the fracture and reduction of the congruent joint, while allowing early active motion, would be thought to be ideal in most patients with fracture-dislocation of the PIP joint. 1 –6,8 –10,13 –24
At present, various different dynamic external traction systems are commonly being used to treat the intra-articular fractures and fracture-dislocations of the PIP joint. 1 –14,17 –24 Almost all of those systems use pins placed through the center of rotation of the proximal phalangeal head and through various sites in the middle phalanx that allow for motion of the PIP joint. 3 –5,7,9,10,14 Among the many dynamic external traction systems, Robertson’s three-way traction device was the first to be known as a representative external traction, however the apparatus is very bulky and uncomfortable to wear. 7,12,17 Inanami’s pantograph system and Ohno’s dynamic distraction apparatus (DDA) system are similar to but more complicated than the PRTS, 7,11 because both of these systems require a special apparatus with exclusive parts.
The PRTS used in the current study was originally reported by Suzuki et al. 14 Suzuki et al. and de Soras et al. described excellent results with the use of this PRTS for comminuted unstable intra-articular fractures of the PIP joint of the digits and the interphalangeal joint of the thumb. 5,14 Deshmukh et al. related that the capsuloligamentotaxis by the PRTS achieves proper articular congruity and healing during early mobilization. 3 Presently, there are similar reports on the dynamic external traction systems by Slade et al. and other authors. 1,2,4,6,13 However, they are basically the same principle as the traction system reported by Suzuki et al. 14 They differ only in the design of bends or the insertion positions of the most proximal and distal pins that hook the rubber bands. 1,2,4,6,13
Many authors have reported that good clinical results could be achieved for the intra-articular fractures of the PIP joint and the unstable fracture-dislocations of the PIP joint using the PRTS. They showed that average ranges of motion of the PIP joint were from 56.6° to 85.0°. 1 –6,8,10,14 In the current study, the average active range of motion of the PIP joint was 74.6°. Our results were similar to those of the above mentioned reports.
The PRTS is thought to be applicable not only to fractures of the middle phalanx but also to fractures of the distal portion of the proximal phalanx. 9 Most previous reports regarding the indication of the PRTS have focused on unstable fresh intra-articular fractures of the PIP joint. 1 –6,8,10,14 Suzuki et al. described that there are PIP joint fractures where conservative treatment or open reduction and internal fixation alone is difficult to treat or may lead to joint contracture. 14 In the current study, we also use the PRTS for an incomplete amputation of a digit, a pathological fracture due to enchondroma, and a patient with transplanted costal osteochondral bone for comminuted fracture and defect of proximal phalanx condyle. In these three cases, excellent or good clinical results were obtained according to Ishida’s evaluation. Thus, we believe that the PRTS is capable of treating a wide range of complex intra-articular fractures of the PIP joint.
Furthermore, treatment for old fractures can occur joint contractures as opposed to fresh cases after surgery. It is important for old fractures to perform early exercise of range of motion of the PIP joint using the PRTS immediately after internal fixation, as similar to fresh fractures. Because early mobilization using the PRTS is necessary, not only for preventing joint stiffness but also to encourage the nutrition and remodeling of the articular surface. In this study, there were no significant differences in active range of motion of the finger, union rate, and infection rate between fresh and old fractures. Therefore, I recommend the PRTS use for old fractures of the PIP joint as similar to fresh ones.
We consider that the distinctive advantages of the PRTS over other techniques are as follows 6,14 : (1) small simple lightweight structure, (2) easy procedure, (3) minimally invasive technique, (4) only inexpensive wires and rubber bands required, and (5) possibility to perform in case of emergency. This external traction system can also be applied to the long finger or ring finger sandwiched between adjacent fingers. The PIP joint dislocation in either volar or dorsal direction is repositioned easily only by using a single reduction pin. The PRTS can also be used in combination with open reduction and internal fixation of the PIP joint. Most importantly, it is advantageous, compared to other dynamic external fixations, in that the PRTS enables exercise of the range of motion without inserting wire into the center of motion of the PIP or DIP joint.
However, it should be noted that even with the PRTS, not only the stiffness of the PIP joint but also that of the DIP joint can occur. Some authors have remarked on the reduced range of motion of the DIP joint after using the dynamic external traction system. 1,3 Agarwal et al. also indicated that secondary stiffness of the uninvolved DIP joint is an actual risk, especially when open reduction and internal reduction is simultaneously performed. 1 Some reports demonstrated that average ranges of motion of the DIP joint were from 39.6° to 46.5°. 2,3,10 These results were similar to our results. We had a total mean range of DIP joint motion of 45.4°. In the current study, the slight contracture of the DIP joint was also observed.
We consider that the reasons that extension contracture of the DIP joint can occur are as follows: (1) because the wire is inserted to the center of the middle phalanx to which the collateral ligament is attached, the exercise of range of motion of the DIP joint may become insufficient due to the resulting pain, (2) the lateral band may be adhesive at the fracture lesion, (3) DIP joint fixation by wires is required for about 1 month in case of the bony mallet finger. Of our 39 cases of fractures of the PIP joint, 8 bony mallet fingers were combined in this study. Agarwal et al. stated that the incidence of this may be lessened by careful physiotherapy immediately after surgery. 1 Thus, it is necessary to pay attention to active and passive exercise of range of motion of both the PIP and the DIP joints (Figure 8).

Active and passive exercise of range of motion of both the PIP joint and the DIP joint. PIP: proximal interphalangeal; DIP: distal interphalangeal.
Limitations
There are some limitations to this study. First, the current study had a relatively small sample size. A larger sample size may provide more detailed information to our findings. Second, the data of the current study were evaluated in a retrospective design. Finally, a weakness of the current study was relatively short follow-up, which is an insufficient expanse of time to assess possible osteoarthrosis. Future researches will address long-term.
Conclusions
The current study demonstrated good clinical results of the PRTS for comminuted intra-articular fractures and fracture-dislocations of the PIP joint.
From this study, we found that the PRTS could be used to treat various difficult unstable injuries with very good functional results. This technique can be helpful not only to achieve anatomical reduction and stable fixation of fracture fragments by capsuloligamentotaxis but also to prevent joint stiffness by early mobilization. We consider that the PRTS can be a useful dynamic external traction system because it is widely effective for various fracture types of the PIP joint in the hand.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.