
Abstract
Purpose:
Deep palmar tumors of the hand are very rare, and reported cases are usually benign. The most important issue is frequent anatomical variations with challenging surgical exposure and excision of these lesions. Some case reports or a small series of patients have been reported in the literature. The aim of this study was to present our experience with the deep palmar tumors of the hand.
Patients and Methods:
In the study, retrospective analyses of 43 patients treated with deep palmar tumors of the hand between January 1998 and June 2015 were evaluated. Tumors and tumor-like pathologies of the deep palmar space of the hand were retrospectively evaluated according to age, gender, localization, preoperative symptoms, size, site, treatment methods, histopathology, and early and late complications. Statistics and data analyses were also performed.
Results:
All 43 pathologies were benign, and histopathologic diagnoses were 10 lipomas, 8 ganglions, 5 giant cell tumor of the tendon sheath, 4 schwannomas, 3 hemangiomas, 3 palmar fibromatosis, 2 epidermal cysts, 2 neurofibroma, 1 angiolymphoid hyperplasia with eosinophilia, 1 granuloma, 1 calcifying aponeurotic fibroma, 1 digital fibroma, 1 foreign body granuloma, and 1 lipofibromatous hamartoma. The most common complication was temporary numbness and paresthesias of the digits. Marginal excision was performed in 40 patients, excision with nerve grafting in 2 patients (with neurofibroma) and carpal tunnel release in one patient with lipofibromatous hamartoma.
Conclusion:
In the deep palmar space of the hand, pathologies are closely associated with tendons, muscles, and neurovascular structures. Preoperative magnetic resonance imaging is helpful for the preoperative diagnosis, evaluating tumor extension, and successful surgical planning.
Introduction
Tumorous conditions of the hand are frequently managed by hand surgeons. Various tumors with different origins have been reported in the hand. 1 –4 Clinical characteristics and physical examinations of these lesions may vary between the different tumor types. Clinicians should be familiar with frequency, distribution, and clinical characteristics of the hand tumors and tumor-like lesions. Scientific approach to these wide spectrum of tumors is essential in the diagnosis and management process.
Interestingly, deep palmar tumors of the hand are rare, and reported cases have been usually benign. However, the most important point is that the palm of the hand has various anatomical variations, which make the exposure and removal of the lesions challenging. Tumor and tumor-like lesions of the hand can be diagnosed by patient history, physical examination, or diagnostic tools; but the definitive diagnose is made by excisional biopsies. Magnetic resonance imaging (MRI) is important to determine the characteristics and extent of soft tissue lesions and discrimination of relationship between the neurovascular structures and tendons.
When we reviewed the literature, only a few case reports or small series of patients were reported, which focused on spesific tumor types. The aim of this study was to present clinical features, frequencies, treatment strategies, and management of possible complications with the deep palmar tumors of the hand.
Patients and methods
Retrospective analyses were designed with the patients treated with deep palmar tumors of the hand. Medical records were retrospectively reviewed by searching the databases, and 51 patients were operated on between January 1998 and June 2015. The retrospectively analyzed parameters included age, gender, localization, preoperative symptoms, size, site, treatment methods, histopathology, and early complications of surgery and recurrences. The patients were invited in for a final evaluation. Forty-three patients were available for the final follow-up examinations and included in the study. Recurrences and permanent complications were evaluated in the final evaluation.
The Ethics Committee approved the study, and informed consent was provided by all patients. All patients were evaluated with physical examination and preoperative MRI for surgical planning, while X-Rays were obtained if necessary. Deep palmar space was divided into five zones: 1: thenar; 2: central, 3: hypothenar, 4: radial metacarpophalangeal (RMP), and 5: ulnar metacarpophalangeal (UMP; Figure 1). In the postoperative period, sensorial evaluations of patients consisted of a static 2-point discrimination (s2PD) test and the Semmes Weinstein monofilament (SWM) test. Recurrences were confirmed with physical examination and MRI.
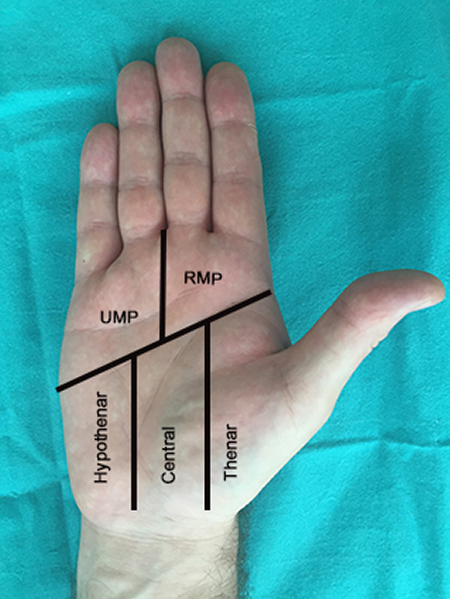
Deep palmar space was divided into five zones UMP: ulnar metacarpophalangeal; RMP: radial metacarpophalangeal.
Descriptive statistics are presented with frequency, percent, minimum, and maximum. Fisher’s exact test or Pearson χ 2 test was used to analyze categorical data. Analyzes were performed with SPSS 23.0 program. p < 0.05 was considered statistically significant.
Results
The mean age at the operation was 38.5 years (range: 9–83). There were 21 (49%) male and 22 (51%) female patients included in our study. The left side was affected in 24 (56%) patients and the right side in 19 (44%). The sizes of resected tumors were between 2 × 1 × 1 cm3 and 6 × 5 × 4 cm3. The most common preoperative symptom was enlarging mass, which was observed in all patients. Nerve compression was observed in 22 patients, half in the ulnar nerve (n: 11) and the other half in the median nerve (n: 11). Motor involvement was detected in two patients with mass in the Guyon canal. Other preoperative symptoms were functional impairment in 12 patients (28%), pain in 5 patients (12%), and pruritus in 1 patient (2.3%). Pain was the main complaint in patients with schwannoma. The mean follow-up period was 60 months (range: 13–168). All surgical procedures were performed under loupe magnification. Marginal excision was performed in 40 patients, carpal tunnel decompression in 9, Guyon canal decompression in 4, and excision with nerve grafting in 2 patients (with neurofibroma). Carpal tunnel or Guyon-Loge release was performed in 12 patients (8 ganglions, 1 schwanoma, 1 hemangioma, 1 neurofibroma, and 1 granuloma) in addition to excision. In a patient with lipofibromatous hamartoma, Carpal tunnel decompression was performed without excision. Over a 15-year period, 43 deep palmar masses with 14 different histopathological types were excised. All 43 pathologies were benign, and there were 10 lipomas (23.3%; Figure 2), 8 ganglions (18.6%), 5 giant cell tumor of the tendon sheath (GCTTS; 11.6%; Figure 3), 4 schwannomas (9.3%), 3 hemangioma (7%), 3 Palmar fibromatosis (7%), 2 epidermal cysts (4.6%), 2 neurofibroma (4.6%), 1 angio-lymphoid hyperplasia with eosinophilia (ALHE; 2.3%), 1 granuloma (2.3%), 1 calcifying aponeurotic fibroma (CAF; 2.3%), 1 digital fibroma (2.3%), 1 foreign body granuloma (2.3%), and 1 lipofibromatous hamartoma (2.3%). Preoperative MRI results and postoperative histopathology results were summarized in Table 1. The most common complication was temporary numbness and paresthesias of the digits, which was detected in 11 (25.6%) patients. In the early postoperative period, the s2PDs in the affected fingers ranged from 3 to 6 mm (mean, 4 mm) compared with the range of 2–3 mm (mean, 2.5 mm) on the contralateral hand. The SWM test results ranged from 0.4 to 1.4 g compared with 0.04–0.4 g on the contralateral hand. Numbness dissappeared between 3 weeks and 2 months.

(a) Preoperative view; (b) intraoperative view of giant lipoma; (c) and (d) giant lipoma located at thenar and central zones of the deep palmar space.
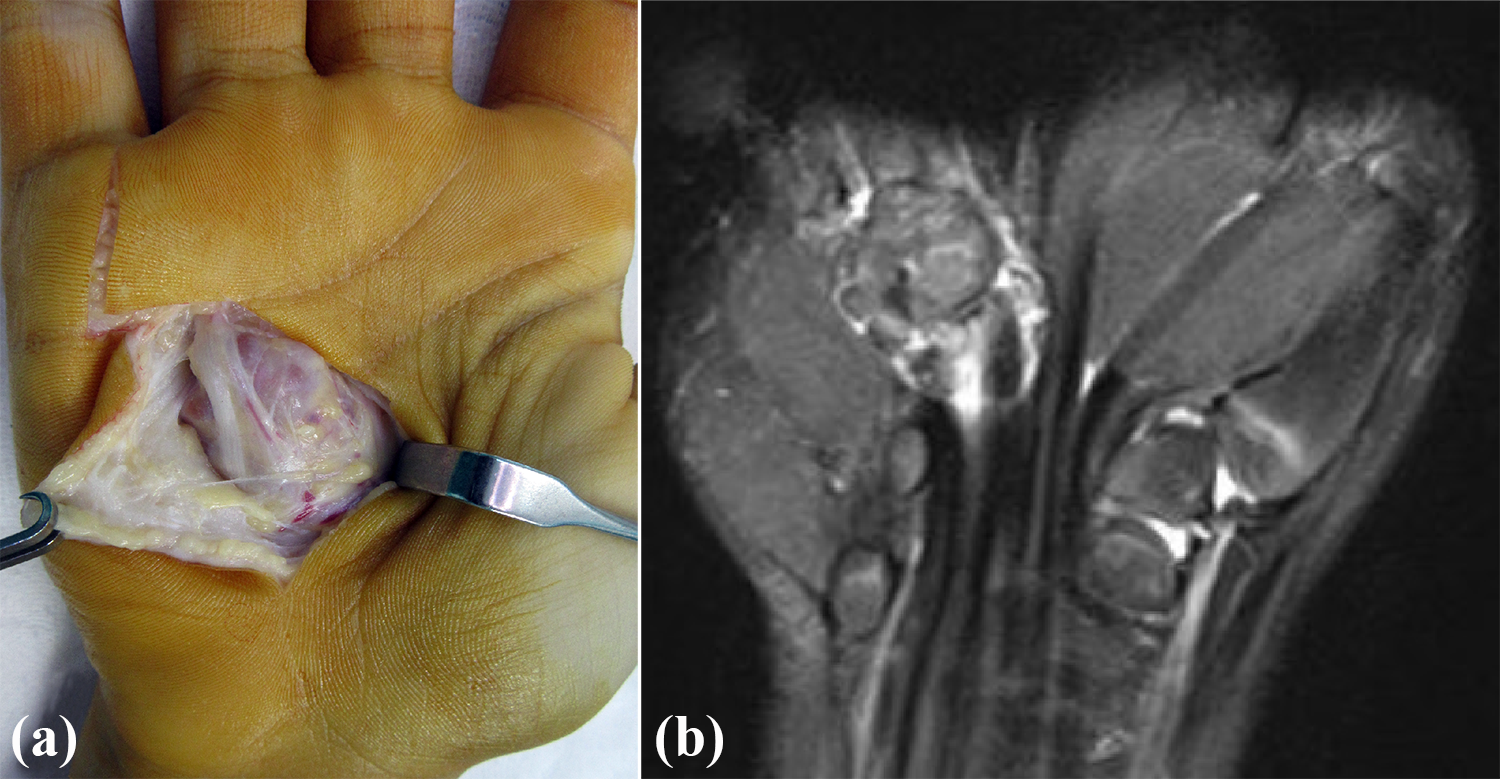
Giant cell tumor of the tendon sheath; (a) Intraoperative; (b) MRI view.
MRI diagnoses and final histopathological results of the cases.

GCtmTS: giant cell tumor of the tendon sheath; CAF: calcifying aponeurotic fibroma; ALHE: angiolymphoid hyperplasia with eosinophilia; LH: lipofibromatous hamartoma; CAF: calcifying aponeurotic fibroma; MRI: magnetic resonance imaging.
Permanent numbness of digits was reported in five patients (11.6%). The s2PDs in the affected fingers ranged from 4 to 8 mm (mean, 5.6 mm) compared with the range of 2 to 4 mm (mean, 2.8 mm) on the contralateral hand. The SWM test results ranged from 0.4 to 2 g compared with 0.07 to 0.4 g on the contralateral hand. Only three (7%) recurrences (2 ganglions and a lipoma) were observed in the postoperative first year. Two cases were reoperated; one case with ganglion refused reoperation, and followed up with the recurrent symptoms. Postoperative complications are summarized in the Table 2.
Postoperative complications.

Deep palmar space was divided into five zones and operated. Deep palmar masses occurred in the 15 central (32%), 11 thenar (23.4%), 10 hipothenar (21.2%), 6 RMP zones (12.7%), and 5 UMP (10.6%; Table 3).
Distribution of deep palmar tumors according to localization.

GCtmTS: giant cell tumor of the tendon sheath; CAF: calcifying aponeurotic fibroma; ALHE: angiolymphoid hyperplasia with eosinophilia; LH: lipofibromatous hamartoma; UMP: ulnar metacarpophalangeal; RMP: radial metacarpophalangeal.
Discussion
Tumorous conditions of the hand and wrist are prevalent and managed by hand surgeons. Patient’s history and physical examination are very important on the way to diagnosis. Imaging methods can provide additional information about the lesions. Plain radiographs can be helpful to distinguish bony lesions from soft tissue lesions. MRI plays a major role in diagnosis and preoperative evaluation, since hand lesions are mostly soft tissue origin. MRI helps us to evaluate the extension, depth, and proximity to the neurovascular structure of the deep palmar masses. 5 Depending on the size of tumoral lesions in the deep palmar space of the hand, the neurovascular structures are pushed to different places than their anatomic locations, and this changes can be detected with MRI. Thereby, MRI can play an important role in deciding surgical approach and surgical plan. 5
Ganglion cysts are the most frequently encountered pathology, which accounts for more than 50% of all masses identified in the hand and wrist region. 1 – 8 The second most common reported pathology is GCTTS. 1 – 8 Deep palmar tumors are rare, and few reports on the subject exist in the literature. Chen et al. 9 have shown that 23 patients with space occupying lesions caused Carpal tunnel syndrome. Six out of 23 lesions were tumors (2 lipomas, 2 ganglion cysts, 1 epidermal cyst, and 1 fibroma of the tendon sheath). In another study, 127 tumor and tumor-like lesions related to nerve compressions were encountered in the upper extremity and 15 deep palmar masses were excised with 10 different histopathological types. 10 In our series, the most common tumors were lipoma (23.3%) and others were ganglion (18.6%), GCTTS (11.6%), and schwannoma (9.3%), respectively.
Lipomas are solitary benign mesenchymal tumors composed of mature adipocytes. Conventional lipomas are one of the most common soft tissue tumors of the upper extremity and the most often detected in subcutaneous tissue of the arm. However, they rarely occur in the deep palmar space of the hand. 11,12 Lipomas may occur at various anatomic localizations in the subcutaneous fat, especially thenar, hypothenar, or within the carpal tunnel. 1,3,11 Lipomas greater than 5 cm are called “Giant Lipoma” and should be distinguished from the well-differentiated liposarcoma. 13 These lesions may cause clinical difficulties like grasping objects, non-tender palmar mass, paresthesias in the sensorial nerve distributions, and triggering. 1,11 –15 MRI is the best diagnostic tool for diagnosis and preoperative planning. Lipomas have high intensity on T1 images and an intermediate intensity on T2 images. 1,13,16 In Leffert’s series, 7 of the 141 cases were in the deep palmar space. 12 Oster et al. 11 reported seven cases between 1959 and 1987. Peripheral nerve entrapment, according to lipomas, are rare and only small series of case reports have been detected in the current literature. 1,3,11 –13 Surgical treatment of these pathologies results clinically excellent with functional and neurological recovery in most of the cases. 1,11 –15 In our series, lipomas were the largest tumors, and 9 out of 10 cases suffered from digital paresthesia.
Upon a literature review, little information about recurrence rates of hand lipomas was found. Leffert operated 141 upper extremity lipomas, and 6 of the 141 cases were previously excised lipomas without aggressive histological features. 12 Just one recurrence was detected 8 months postoperatively, and second operation was performed because of recurrence. Twenty-four months after the second surgery, there were no recurrences postoperatively.
Ganglions, frequently located in the dorsal wrist, are the most common soft tissue lesions observed in the hand. Other possible locations are the volar wrist, metacarpophalangeal joint over the A1 pulley, or the dorsal part of the distal interphalangeal joint. 1 –6,8,16,17 Deep palmar space is an uncommon location for ganglions. In our series, we detected 8 ganglions in the deep palmar space. Four of them were detected in the carpal tunnel and other four were at the Guyon canal in the hypothenar zone. There are three accepted treatment options: (1) observation, (2) aspiration, and (3) surgical excision (open or arthroscopic). Aspirations may result in high recurrence rates. 1,6,8,16,17 In a systemic review, Head et al. reported recurrence and complication rates in the meta-analysis after comparing arthroscopic surgical excision, open surgical excision, and aspiration. 16 Recurrence rates were 6%, 21%, and 59%, respectively. 16 Complication rates were 4%, 14%, and 3%, respectively. 16 In our series, two recurrences occurred out of eight cases (one in the carpal tunnel and one in the Guyon Canal). The patient with ganglion in the Guyon canal was reoperated at postoperative 9 months and 20 months after the second operation (no recurrences were detected). The other patient who had ganglion in the carpal tunnel refused reoperation and was followed up with the recurrence. There were no correlations between recurrences and type of tumors, region, or marginal resections.
GCTTS is the second most common lesion of the hand and also known as fibrous xanthoma or pigmented villonodular tenosynovitis. 1 –4,6,7,18 GCTTS may arise from the synovium of joints, bursa, and tendon sheaths. These tumors may occur between ages of 30 and 50 years and are predominantly observed in females. 1 –4,6,7,18 –20 Clinically, slow-growing, multi-lobulated, and firm non-tender masses may occur around the volar part of the distal interphalangeal joint in the radial three digits. 1 –4,6,7,18 –20 The typical MRI appearance is extra-articular soft tissue mass with low signal intensity on the T1- and T2-weighted MRI images. 5
Recurrence rates has been reported between 2.4% and 44%, and incomplete excision with presence of satellite lesions is the major cause of recurrences. Others are patients with degenerative joint disease, radiologic bony erosion, intra-articular invasion, presence of tendon, or capsular joint involvement. 2,18 –24 Kotwal et al. suggested low-dose local irradiation and reported low recurrence rates without any additional complications. 22 Deep palmar space is a rare region for GCTTS. Lancigu et al. reviewed 96 cases, and only 3 occurred in the deep palmar region (2 hypothenar and 1 in thenar space). 23 Monaghan et al. reported hand involvement in 93% of the patients in their series, and the palmar involvement rate was 8.4%. 25 In our series, five GCTTS were observed. Interestingly, two were in the UMP, two were RMP, and one in the hypothenar zone.
Schwannomas, slow-growing tumors, often represent with enlarging mass, pain, and neurologic deficit via compression of nerve fibers and rarely involve the nerves of the hand. They differentiate from neoplastic schwann cells, and most schwannomas are solitary lesions. Sometimes, multiple lesions on a single nerve may occur in the flexor surface of the hand and forearm. 2,3,6 Ozdemir et al. reported 14 cases, and 3 were in the palmar region. 26 In another study, Gosk et al. operated on 31 benign nerve tumors and 10 of them were in the palmar region. 27 In our series, four schwannomas were excised from the deep palmar space, and pain was the main complaint in patients with schwannoma, which is consistent with the literature.
Neurofibromas may also show similar clinic features as schwannomas; however, they have different characterictics. Although both tumors arise from schwann cells, neurofibromas may contain perineural-like cells, fibroblasts, mast cells, and mucoid matrix. 2,3,6,27 Unlike other tumors, schwannomas and neurofibromas may frequently cause pain. Total excision is more complicated than the schwannomas. 2,3,6,27 In present study, 2 neurofibromas were observed and nerve grafting was required after total excision of neurofibromas.
Epidermal cyst is the third most common tumor of the hand. They are keratin-filled cysts arising from epithelial cells that have been implanted to a subdermal space secondary to trauma or surgery. 8 Although frequent in the superficial layers of fingertips, deep palmar space is a rare location. In present study, two of the deep palmar masses were epidermal cysts and marginal excision was performed.
To our knowledge, this is the largest study about deep palmar tumors of the hand. The limitation of this study is the lack of preoperative The Disabilities of The Arm, Shoulder and Hand (DASH) scores.
Conclusion
In the deep palmar space of the hand, pathologies are closely associated with tendons, muscles, and neurovascular structures. Preoperative MRI is helpful for the preoperative diagnosis, evaluating tumor extension and successful surgical planning.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.