
Abstract
Background:
Incidence of femoral neck fracture has risen with the aging of the population and has critical implications with regard to patient death, functional dependence, and social costs. Screw fixation using triangular configurations and calcar placement are still the preferred treatment for nondisplaced femoral neck fracture, to reduce the risk of loss of reduction and nonunion. However, this method is still controversial in terms of the effects of screw trajectory, including parallel or nonparallel configurations, on fixation of femoral neck fractures. This study aimed to compare the incidence of complications between patients who have undergone fixation with a parallel or a nonparallel screw trajectory.
Methods:
We retrospectively analyzed 55 patients who were older than 60 years and diagnosed with nondisplaced femoral neck fracture from March 2014 to March 2016, and who were treated with cannulated screw fixation in our institution. Patient demographics, radiographic parameters including reduction quality, screw trajectory, and complications during the follow-up period were all evaluated.
Results:
The overall complication rate for screw fixation in elderly patients was 23.6%, and screw cut-out was the most common complication, occurring in 14.5% of all enrolled patients. Also, we found that screw cut-out occurred in more osteoporotic patients, and all screw cut-outs were in groups treated with a nonparallel screw trajectory. However, parallel screw fixation was inclined to back out more after fracture healing and had a lower risk of postoperative screw cut-out.
Conclusions:
Our results suggested that fixation with nonparallel screws for nondisplaced femoral neck fracture in elderly and osteoporotic patients might interfere with shortening of the femoral neck along with fracture healing, leaving patients at risk of postoperative screw cut-out from the femoral head.
Introduction
Incidence of hip fracture, which is one of the fractures linked with osteoporosis, has been rising along with the aging of the population and has critical implications with regard to death, functional dependence, and social costs. 1,2 Femoral neck fractures account for nearly 50% of all hip fractures. 3 Since Garden and colleagues first described the successful treatment of femoral neck fracture using crossed screws in 1961, internal fixation using 2 or 3 screws has become the preferred treatment for young patients or nondisplaced fractures, in contrast to displaced femoral neck fractures, which are usually treated with arthroplasty. 4 –7 However, even with general consensus on the benefits of fixation for femoral neck fractures, the reoperation rate, reported to be up to 10% within 1 year after injury, is still a concern. 8,9
In general, studies have demonstrated that screw fixation using triangular configurations for femoral neck fracture can provide a higher peak load, less displacement, and more energy absorption before failure. 10,11 Furthermore, calcar screw placement is essential to decrease the risk of loss of reduction and nonunion. 12,13 The quality of reduction is of critical importance and is regarded as the strongest predictor of postoperative re-displacement of the fracture. 14 However, there is still controversy regarding screw trajectory, including parallel or nonparallel configurations, for the fixation of femoral neck fracture. To the best of our knowledge, there is also a lack of biomechanical studies discussing the effect of screws trajectory on the fixation of femoral neck fracture in the current literature. A parallel screw trajectory was reported to incur a lower incidence of nonunion and osteonecrosis of the femoral head (ONFH) than a crossed screw trajectory, 15 although other studies reported spreading of the screws on the lateral view of radiographs, and that a divergent screw trajectory can instead reduce nonunion risk. 16,17
In our practice, we noticed that fixation with a parallel screw trajectory usually resulted in a tendency toward a greater screw back-out distance accompanied by a shortening of the femoral neck after fracture union, especially among elderly patients, whereas fixation with a nonparallel screw trajectory did not, and might be associated with complications including screw cut-out (Figure 1). This study aimed to assess the incidence of complications between patients who underwent fixation with a parallel or a nonparallel screw trajectory for femoral neck fracture. Since femoral neck shortening after fixation for femoral neck fracture frequently occurs and has a reported incidence of nearly 30%, 18 we hypothesized that fixation with a parallel screw trajectory, which has a potential for better screw sliding accompanied by shortening of the femoral neck after fracture union, may protect the femoral head from screw cut-out and associated complications.

A 71-year-old female diagnosed as having a nondisplaced femoral neck fracture was treated with cannulated screw fixation with a nonparallel screw trajectory. Screw cut-out was found 2 weeks after operation. She received a second operation to change the screw. The arrow shows the area of neck shortening with impaction of the femoral neck after operation. (POD: post-operative day)
Patients and methods
Patient demographics
In our institution, elderly patients suffering nondisplaced femoral neck fracture, including Garden classification type I and type II, are routinely treated with cannulated screw fixation. Therefore, we retrospectively analyzed the records of 68 consecutive patients who were older than 60 years and diagnosed with nondisplaced femoral neck fracture, and who were treated with cannulated screw fixation in our institution from March 2014 to March 2016. Screw fixation was performed by three senior surgeons (Chuang T-Y, Ho W-P, and Leu T-H), and all fixations were constructed using triangular configurations, following the principle of screw fixation through the inferomedial cortical bone of the femoral neck. 13,19 Postoperatively, all patients were routinely instructed to bear partial weight for the first 6 weeks after the operation. Thereafter, full weight-bearing as tolerated was allowed. In addition, all patients routinely received clinical and radiological follow-up 1 month, 3 months, 6 months, and each year after the operation. The exclusion criteria included patients who were followed postoperatively for less than 6 months, except those with a shorter follow-up period but with definite complications developing within 6 months after the operation. The institutional review board approval was obtained for a retrospective review of medical records and radiographs. Demographic data concerning age, gender, waiting time before screw fixation, follow-up period, and mortality were collected retrospectively from patient records. The t-score for each patient based on the bone mineral density (BMD) evaluation 1 year before and after screw fixation was also documented. All patients with confirmed diagnosis of osteoporosis routinely received pharmacological treatment with antiresorptive agents according to the clinician’s preference in our institution.
Of the 68 patients, 8 were followed up less than 6 months and were excluded from further analysis. In addition, five patients expired on the postoperative 10th, 12th, 26th, 30th, and 48th day, respectively. Cause of mortality included pneumonia, stroke, and cardiac arrest. All of the mortality events developed within 2 months after fixation surgery, and the overall mortality rate at postoperative 6 months was 8.3% (5/60). Finally, 55 patients were enrolled for radiographic and outcome assessment.
Radiographic evaluation
Diagnosis of femoral neck fracture was reached by observing the fracture line between the femoral head and neck. Basicervical femoral neck fractures, which were routinely treated with dynamic hip screw fixation in our institution, were excluded from this study. Fracture type, graded using the Garden classification on the preoperative radiograph, was recorded. Furthermore, the Garden alignment index, average distance between screw tips and the subchondral boundaries, lateral spread of the screws on lateral views of the radiograph, length choice of screw threads, and screw trajectory were all assessed using the anteroposterior (AP) and lateral views of radiographs immediately after surgery.
The Garden alignment index was used to assess the levels of reduction measured by a plain radiograph. 20 When the Garden alignment index fell within the range of 160–180°, as judged by AP views, and the range of 170–190°, based on lateral views, the reduction was declared to be “excellent”; the reduction was judged to be “good” if either of the two images fell within the range and “poor” if neither fell within the range. The average distance between the inserted fixation screws and the subchondral boundaries of the femoral head was measured using the AP and lateral views obtained by plain radiography. Cases that fell within the range of 160–180° on AP views and 170–190° on lateral views according to the average distance to the subchondral boundaries of the femoral head on both AP and lateral views were declared to have achieved “excellent” results; results were judged as “good” if only one of the two images fell within the range and as “poor” if neither fell within the range. The degree of lateral spread of the screws, expressed as a percentage and defined as the distance between the most anterior and posterior position of the screws on the lateral radiographs, divided by the maximum diameter of the femoral head, was also recorded 17 (Figure 2(a)). Whether a short or long length of screw threads was used, the screw trajectory which was classified as parallel or nonparallel, and events of drills or screws penetrating out of femoral head during operation were all recorded according to the surgical records. A nonparallel screw trajectory was defined as when the angle of any two of the three cannulated screws was more than 5° on either AP or lateral views of plain radiography (Figure 2(b)).

Lateral spread and screw trajectory measurements: (a) lateral spread on the lateral view of the radiograph = b/a and (b) nonparallel screw trajectory with angulation of 8°.
Outcome measurement
A diagnosis of osteosynthesis was made when trabeculation across the fracture line was observed on simple radiographs. Complications including postoperative infection, ONFH, nonunion and fixation failure, cut-out of screws from the femoral head, and a history of secondary operation were all documented using follow-up radiographs and medical records. A diagnosis of ONFH was made when the patient reported clinically sustained pain in the hip joint during the follow-up period, with subchondral sclerosis or segmental collapse of the femoral head on simple radiographs. 21 Nonunion and fixation failure were defined by the presence of persistent pain in the hip joint without progression of fracture healing after 6 months or re-displacement at the fracture site on simple radiographs. 22
The back-out distance of the cannulated screws and shortening of the femoral neck during fracture healing were also quantified based on the follow-up radiographs. The screw back-out distance was defined as the average distance from each screw head to the lateral femoral cortex on the AP view of the final follow-up radiographs less that measured on the plain films taken immediately postoperation (Figure 3(a)). Furthermore, to assess decreases in abductor moment arm, the difference in length between the healthy and unhealthy sides (horizontal shortening) was quantified by measuring the distance from the medial border of the femoral head to the lateral border of the greater trochanter at the final follow-up radiography visit following bone union 18 (Figure 3(b)).

Screw back-out distance and femoral neck shortening: (a) the average screw back-out distance was measured by the difference on plain films between the final follow-up and immediately postoperation, and (b) the horizontal shortening of the femoral neck on the final follow-up radiograph = a−b. (POD: post-operative day)
All of the radiographic measurements and medical records data were documented by a senior orthopedic resident (Wu Y), who was blinded to the purpose of the study and not involved in the analysis of the collected data, so as to avoid potential bias.
Analyses
All statistical analyses were performed using IBM SPSS Statistics version 20 software (IBM Co., Armonk, New York, USA). The Student’s t-test or Mann–Whitney U test was used to compare differences between two independent, ordinal groups with or without a normal distribution, respectively. For comparison of categorical variables, the χ 2 test with Fisher’s exact test was used. p Values of 0.05 or less were considered statistically significant.
Results
The average age of the 55 enrolled patients with a follow-up period of more than 6 months was 76.3 years (range, 60–94 years; Table 1). Most of the patients were female (72.7%) and classified as Garden type I (81.8%). Although not every patient received a BMD study, the average t-score was −2.74. The average follow-up time was 14.7 months (range, 6–52 months), and the average waiting time before surgery was 35.9 h (range, 5–168 h). Moreover, 22 of the 55 patients underwent cannulated screw fixation with a nonparallel trajectory, and 33 patients were fixed using a parallel trajectory. Screws with a short thread were utilized for fixation in most of the patients (80%) and achieved good to excellent Garden alignment index results and screw subchondral distance. No events of drills or screws penetrating out of femoral head during operation were documented on the surgical records among all enrolled patients. The overall complication rate was 23.6%. Screw cut-out was the most common complication (14.5%; Figure 3), and there were no postoperative infections. Of the 13 patients who suffered complications, only 4 received a secondary operation, including one for changing of the screws and 3 for bipolar hemiarthroplasty. The overall reoperation rate was 7.3% (4/55).
Patient demographics.
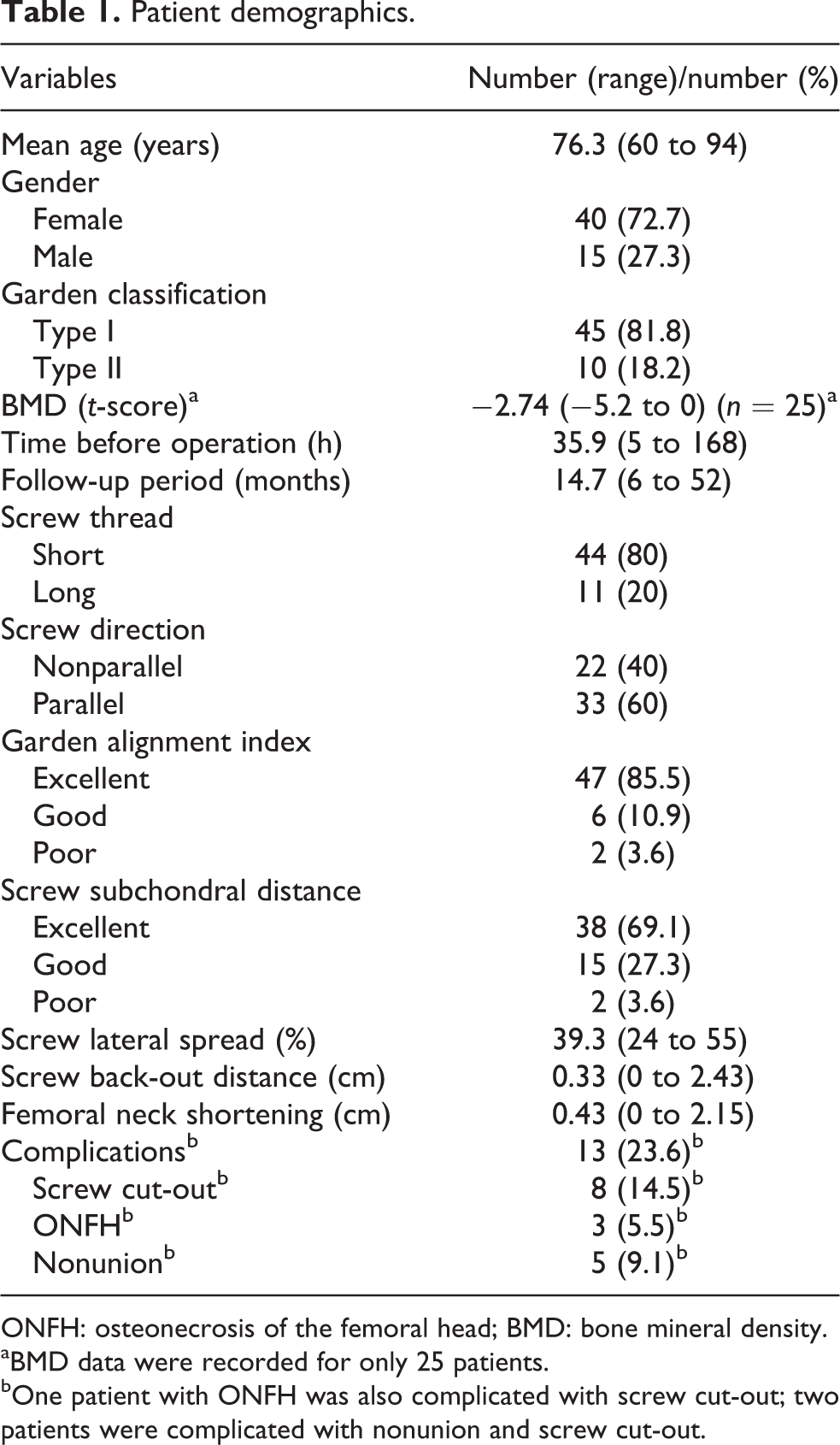
ONFH: osteonecrosis of the femoral head; BMD: bone mineral density.
aBMD data were recorded for only 25 patients.
bOne patient with ONFH was also complicated with screw cut-out; two patients were complicated with nonunion and screw cut-out.
When we compared patients complicated with or without screw cut-out, there were no differences regarding gender, Garden classification, waiting time before operation, follow-up period, choice of screw thread length, Garden alignment index, screw subchondral distance and distance of screw back-out, or femoral neck shortening (Table 2). However, patients complicated with screw cut-out tended to be older, although without statistical significance (p = 0.07). To our surprise, patients complicated with screw cut-out had all been treated with a nonparallel screw trajectory (p < 0.01) and had a significantly higher screw lateral spread percentage (p < 0.01). In addition, the t-score measured by BMD was significantly worse in patents complicated with screw cut-out than in patients without screw cut-out (p = 0.04).
Comparison of patients with or without screw cut-out.

BMD: bone mineral density.
Then, we compared patients treated with a parallel or nonparallel screw trajectory (Table 3). There were no significant differences in age, gender, t-score data, Garden classification, waiting time before operation, follow-up period, choice of screw thread length, Garden alignment index, screw subchondral distance, screw back-out distance, and femoral neck shortening between these two groups. However, patients treated with a nonparallel screw trajectory not only had a significantly higher screw lateral spread percentage (p < 0.01), but also suffered a higher risk of screw cut-out (p < 0.01) when compared with patients treated with a parallel screw trajectory. Moreover, patients treated with a parallel screw trajectory were inclined to have greater screw back-out, although the difference was insignificant (p = 0.08).
Comparison of patients treated with a nonparallel or parallel screw trajectory.

ONFH: osteonecrosis of the femoral head; BMD: bone mineral density.
Discussion
Fixation for nondisplaced femoral neck fractures in elderly patients is still the main treatment option in current practice. 6,23 A single-center retrospective cohort study in Norway included 383 patients who underwent parallel screw fixation for nondisplaced femoral neck fractures with up to 10 years of follow-up and found that the 1-year mortality rate was 32% among males and 17% among females 70 years or older, respectively. 8 In addition, 8% of these patients received at least one subsequent surgery within 1 year postoperatively, and 25% of the patients needed conversion to arthroplasty in the long term. Similarly, in our review of 60 patients 60 years or older who underwent cannulated screw fixation for nondisplaced femoral neck fractures and were followed up for at least 6 months, we found that the 6-month mortality rate was 8.3%, and all mortalities occurred within 2 months after operation. The overall complication rate was 23.6%, but the reoperation rate was only 7.3%. In general, fixation for nondisplaced femoral neck fracture using cannulated screws is still an acceptable treatment of choice in our institution.
In our study, screw cut-out was the most common complication and occurred in 14.5% of all enrolled patients. Compared to the patients without screw cut-out, those who suffered screw cut-out were more osteoporotic, they had all undergone fixation with a nonparallel screw trajectory, and there was greater screw lateral spread on lateral radiographs. Furthermore, when comparing parallel and nonparallel screw trajectories, parallel screws were inclined to back out further after fracture healing. However, those patients who had undergone fixation with a nonparallel screw trajectory were more at-risk of postoperative screw cut-out in our study. Our finding implied that a nonparallel and widely spread screw trajectory might interfere with shortening of the osteoporotic femoral neck during fracture healing, leading to the screws possibly cutting out from the femoral head (Figure 4).
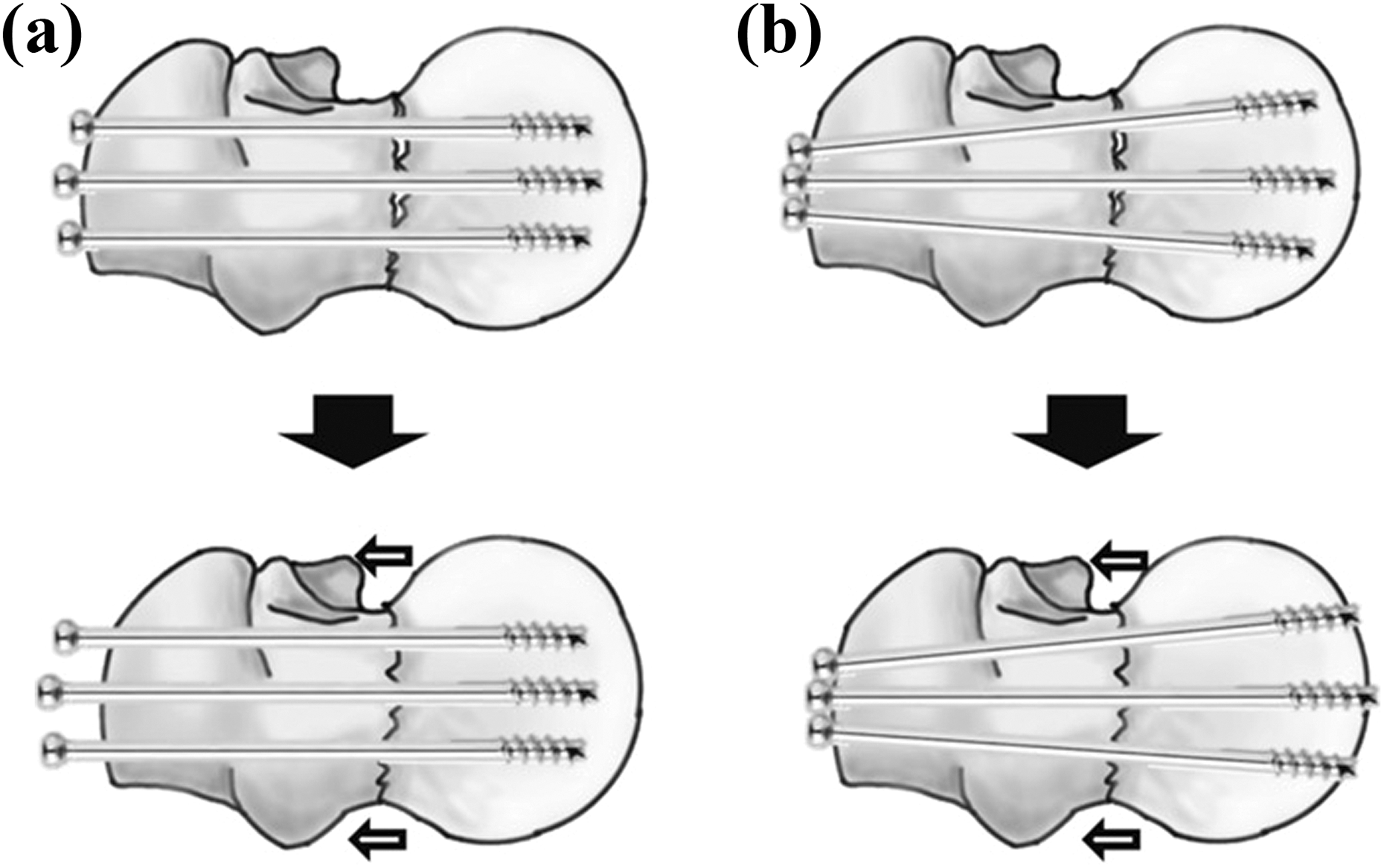
Assumption for screw back-out and cut-out in (a) parallel and (b) nonparallel screw trajectories, respectively, during fracture healing, accompanied by shortening of the femoral neck.
Our results conflicted with those of previous studies promoting a divergent screw trajectory and greater lateral spread of the screws on the lateral radiograph in order to reduce complications. 16,17 Gurusamy et al. reported that a reduced spread of the screws on the lateral view was associated with an increased risk of nonunion of the fracture, but they enrolled patients diagnosed only with displaced intracapsular fracture of the hip and with an age distribution ranging from 22 to 86 years old. 17 In another study, Papanastassiou et al. found that divergent screws could reduce nonunion risk, but this study also enrolled patients with displaced and nondisplaced femoral neck fracture and with a relatively younger mean age (48 years old). 16 In contrast to these studies, our study patients were older (mean age 73.6 years, ranging from 60 to 94 years old) and had a diagnosis of nondisplaced femoral neck fracture. Also, our study group was inclined to be osteoporotic and had a potential for shortening of the femoral neck accompanied by fracture healing, which might explain the difference in our reported results.
The relatively small case number and short follow-up period, which might lead to an underestimation of the true rate of complications or mortality, were the main limitations in our study. Even so, we believe that the significant difference between parallel and nonparallel screw trajectories in our study is convincing enough to set up an assumption worthy of further biomechanical or clinical studies. Another limitation may be that three surgeons performed the fixation surgeries, which may lead to a potential bias affecting the final surgical outcomes. Besides, our study did not compare functional outcomes between groups. Since previous studies reported that shortening of the femoral neck was associated with a poor functional outcome, 18 further study might be needed to clarify the association between functional outcomes and screw trajectory. Last but not least, our results are based on a retrospective analysis, which may mask the true events of drills or screws penetrating out of femoral head during operation omitted on the medial records by the surgeons and potentially increasing the postoperative screw cut-out risk. These limitations may hinder our ability to reach a strong conclusion. Further prospective, blinded clinical studies and experiments based on the biomechanical designs will be needed to strengthen our finding.
Conclusions
Although fixation for femoral neck fracture in young patients with strong bone quality may benefit from divergent screw configurations to minimize complications, our clinical results suggest that nonparallel screw configurations in fixation for nondisplaced femoral neck fracture among elderly and osteoporotic patients might interfere with shortening of the femoral neck along with fracture healing, leaving patients at risk of postoperative screw cut-out from the femoral head.
Footnotes
Author contributions
YW and THL contributed equally to this work.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.