
Abstract
Background:
Recently, several in vitro biomechanical studies that used dual small locking plate fixation for humeral shaft fractures have investigated. However, in vivo studies about dual plate fixation for humeral shaft fractures are limited. The purpose of our study was to report the outcomes of dual small plating for humeral shaft fractures in comparison with those of single large fragment plating.
Methods:
Sixty consecutive patients who underwent an open reduction internal fixation for humeral shaft fractures at our institution from September 2014 to December 2017 were included. Single 4.5-mm locking compression plate (LCP) fixation was used in the first 40 cases, and dual 3.5-mm LCP fixation was used in the final 20 consecutive cases. Data were collected to define patient characteristics, injury mechanism, clinical outcomes, time to surgery, operative time, estimated blood loss, and complications. Using simple radiography during the follow-up period (6, 12, 24, and 52 weeks after surgery), the shoulder and elbow joint ranges of motion (ROM) were also evaluated.
Results:
Demographic data, time to surgery, surgical time, and estimated blood loss had no significant differences between the two groups. No significant differences were observed in nonunion rate and union rate 3 months after surgery. However, two patients (5%) in the single 4.5-mm LCP fixation group showed metal failure and breakage. No significant differences were found in postoperative shoulder and elbow ROM. Three patients (7.5%) in the single plating group and one patient (5%) in the dual plating group developed radial nerve palsy after surgery. No vascular injury and deep infection were observed in either group.
Conclusion:
For diaphyseal humeral fractures, dual 3.5-mm LCP fixation to the humerus is a possible treatment choice. This method showed satisfactory union rate, ROM, and complication rate, without increasing surgical time, in comparison with the conventional single 4.5-mm LCP fixation.
Introduction
The humeral shaft is the region just proximal to the supracondylar ridge and immediately distal to the surgical neck. 1 Humeral shaft fractures typically occur with direct or indirect trauma and account for approximately 3% of all orthopedic injuries. 2,3 Internal fixation with a single large fragment plate is the conventional strategy for surgical management of humeral shaft fractures. 4 In some patients with smaller humeri, large fragment plate fixation is difficult because of the limitation of the diaphyseal shaft length and/or diameter. 5 The drawbacks of the large fragment plate fixation include difficulty of adjusting the number of screws, which can be placed on plates, undesirable stress shielding with bulky fixation, and the need for pre-contouring of the plate to match the diverging anatomy of the metaphysis of the humeral shaft. 5
A recent literature indicates that use of a dual plate is better than that of a large fragment plate in respect of yielding better mechanical properties. 6 In 2013, Kosmopoulos and Nana described that the seven-hole plate lateral and nine-hole plate anterior (90 apart) configuration resulted in optimal fixation with small (3.5-mm) fragment locking plates. 7 In 2016, Karakasli et al. 4 reported that in young adults, eight- to four-hole construction is an option and that an eight- to eight-hole combination may be an option for patients with osteoporosis with 3.5-mm locking plates.
Recently, several in vitro biomechanical studies that used dual small (3.5-mm) locking plate fixation for humeral shaft fractures have investigated plate positioning and the proper number of screws. However, in vivo studies about dual plate fixation for humeral shaft fractures are limited. The goal of our study was, therefore, to report the outcomes of dual small (3.5-mm) plating for humeral shaft fractures in comparison with those of single large (4.5-mm) fragment plating. We hypothesized that clinical and radiologic outcomes would not differ according to the plating methods.
Method
This study received approval from our institutional research ethics committee, and informed consent was obtained (DKUH 2018-12-020). Sixty consecutive patients who underwent an open reduction internal fixation (ORIF) at our institution from September 2014 to December 2017 were included in this study.
The inclusion criteria were humeral shaft fractures classified as 12-A, 12-B, or 12-C according to the classification scheme of the AO/Orthopaedic Trauma Association, 8 age > 18 years, and treatment with open reduction and plate fixation. The exclusion criteria were ipsilateral around elbow injuries, open fracture, and revision cases, including those for nonunion and malunion. Single 4.5-mm locking compression plate (LCP) fixation (Synthes, Solothurn, Switzerland) was used in the first 40 cases, and dual 3.5-mm LCP fixation (Synthes, Solothurn, Switzerland) was used in the final 20 consecutive cases.
Data were collected to define patient characteristics, injury mechanism, clinical outcomes, time to surgery operative time, estimated blood loss, and complications (radial nerve injury, deep infection, stiffness, metal failure, and nonunion). Injury radiographs were reviewed, and the AO/Orthopaedic Trauma Association classification was used to classify the types of fractures. 8 Using simple radiography performed during the follow-up period (6, 12, 24, and 52 weeks after surgery), “union” was defined as the absence of a fracture line or the presence of a bridging callus. Shoulder and elbow joint ranges of motion (ROM) were also assessed.
Surgical technique
Single 4.5-mm LCP fixation group
General anesthesia or brachial plexus block was selected by the anesthesiologist, considering the desire and general condition of the patient. With the arm stretched out on a hand table and the patient positioned supine, the fracture was exposed through an anterolateral approach using a previously described technique. 9,10 The biceps muscle was medially retracted, and the brachialis was split for exposing the humerus. The deltoid insertion was partially elevated to obtain space for plate osteosynthesis. The radial nerve was explored and protected preoperatively through this approach. After subperiosteal dissection, the interpositioned soft tissue and hematoma at the fracture site were removed.
Reduction and fixation maneuvers of the fracture were performed with the elbow flexed. After reduction of the fracture, alignment was confirmed with an image intensifier. Then, a 4.5-mm locking plate and screws were applied at the anterolateral aspect of the humerus with three or four bicortical screws placed on either side of the fracture. Suction drains were inserted before the closure of the wounds, and postoperative assessments of neurology were rechecked and documented immediately after surgery (Figure 1).

Simple radiographs of a 30-year-old man who received 4.5-mm single locking compression plate fixation. (a and b) Preoperative anteroposterior and lateral radiographs showing a displaced humeral shaft fracture. (c and d) Plain radiographs obtained 3 months after surgery, showing complete union of the humeral shaft fracture.
Dual 3.5-mm LCP fixation group
The same position and approach were used for dual 3.5-mm LCP fixation. A detailed description of the surgical procedure follows. After fracture reduction, a short 3.5-mm LCP was applied on the anteromedial surface of the reduced humerus, with two bicortical screws placed on either side of the fracture. Then, a 3.5-mm narrow LCP was applied on the anterolateral surface of the humerus, with four bicortical screws placed on either side of the fracture (Figure 2).
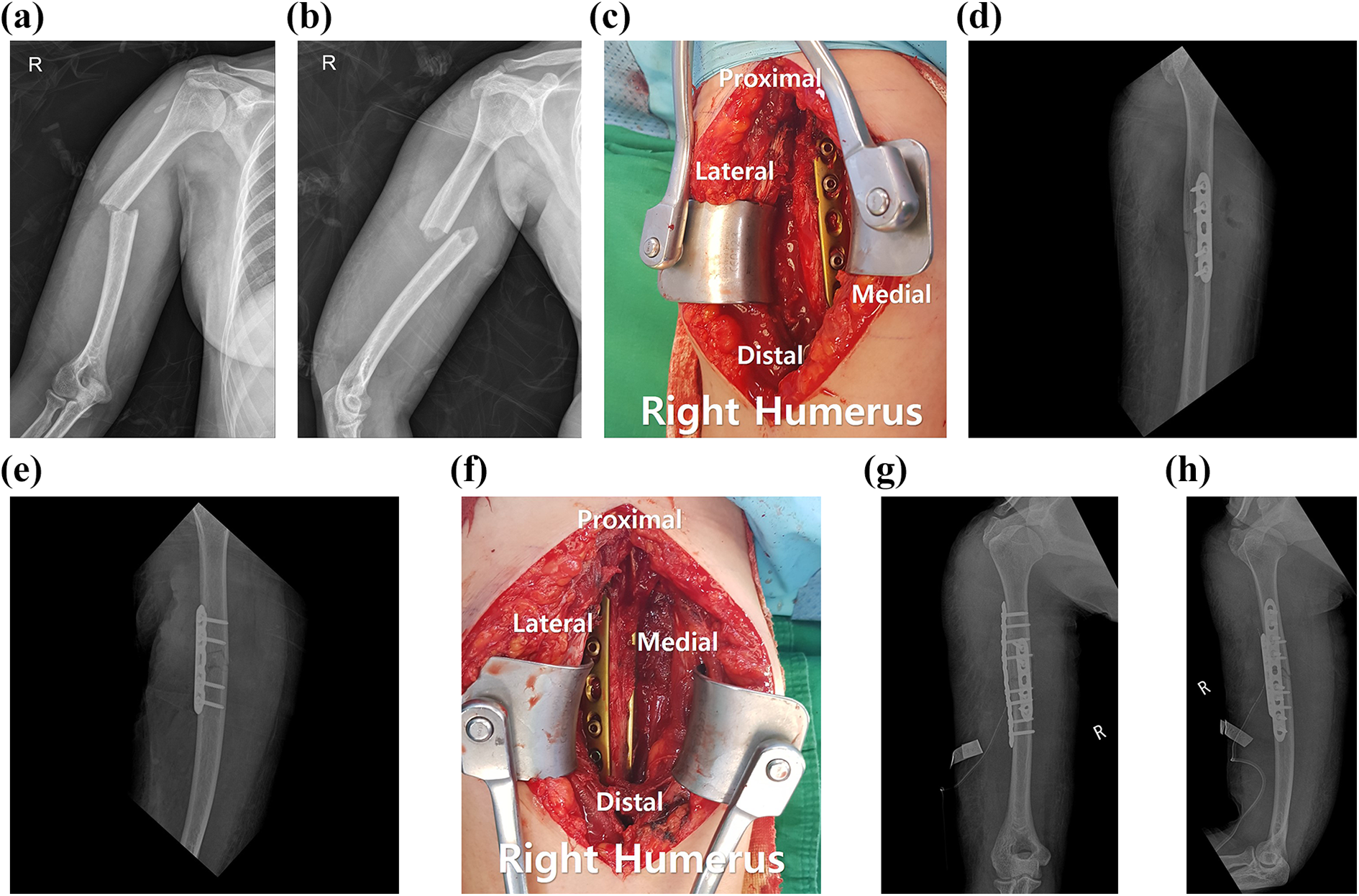
Simple radiographs of a 36-year-old woman. (a and b) Preoperative anteroposterior and lateral radiographs showing a displaced humeral shaft fracture. (c) At first, a 3.5-mm five-hole locking compression plate was applied on the anteromedial aspect with the reduction plate technique. (d and e) Reduction and alignment on intraoperative radiographs. (f) Finally, a 3.5-mm nine-hole locking compression plate was used on the anterolateral aspect. (g and h) Postoperative anteroposterior and lateral radiographs showing dual plate fixation with orthogonal configuration and eight- to four-hole construction.
Postoperative management
After the operation, no external immobilization was required. Velpeau bandage was applied for a week to relieve the immediate postoperative swelling. The patient was placed in a sling for comfort, and ROM of the elbow and the shoulder were allowed 1 week after surgery.
Statistical analyses
To determine the normal distribution of the continuous data the Kolmogorov–Smirnov test was performed, the continuous variable was analyzed using an independent t test, and the noncontinuous variable was analyzed using the Pearson χ2 test. All statistical analyses were performed using the Statistical Package for Social Sciences version 21.0 (SPSS Inc., Chicago, IL, USA), and the level of significance was set at p<0.05.
Results
Demographic data
The study included 20 women and 40 men, with ages ranging from 18 to 83 years. The initial injuries were caused by traffic accident in 26 cases, fall in 16 cases, and sport-related injury in 18 cases. No significant differences were found in demographic data, except the follow-up period, between the two surgical groups (Table 1).
Demographic data.
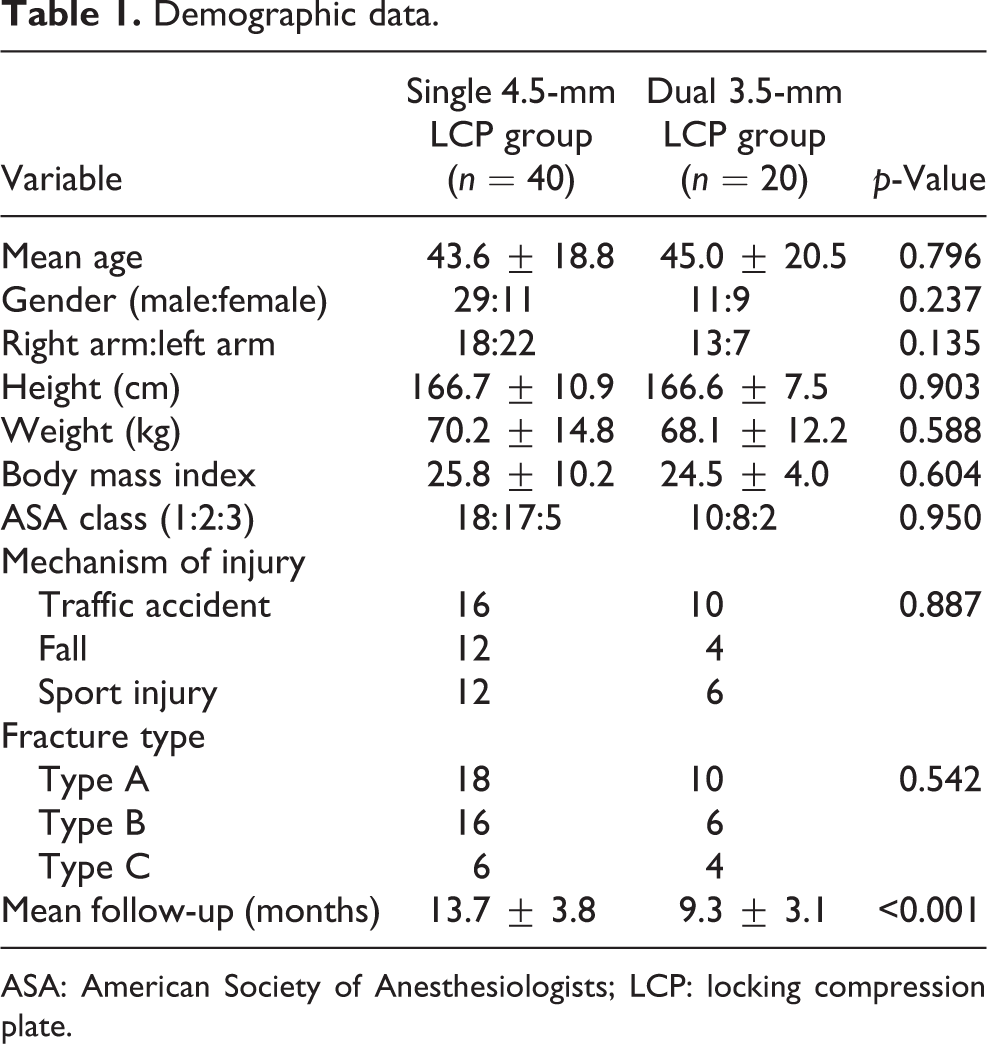
ASA: American Society of Anesthesiologists; LCP: locking compression plate.
Clinical outcomes
The time to surgery was 4.5 ± 3.6 days in the single plating group and 4.7 ± 3.9 days in the dual plating group. The surgical time was 84.1 ± 31.6 min in the single plating group and 71.2 ± 22.8 min in the dual plating group. The estimated blood loss was 179.4 ± 89.8 ml in the single plating group and 157.8 ± 46.5 ml in the dual plating group. No significant differences in time to surgery, surgical time, and estimated blood loss were found between the two groups (Table 2).
Intraoperative finding.

LCP: locking compression plate.
Union was observed 12 weeks after surgery in 31 (77.5%) of the 40 patients in the single plating group. In seven patients (17.5%), healing took longer during the follow-up period. Of the patients who underwent dual plate fixation with iliac bone grafting, one patient (2.5%) showed metal failure at 24 weeks and another patient (2.5%) showed metal breakage with nonunion at 52 weeks after surgery (Table 3).
Results and complications between the two groups.
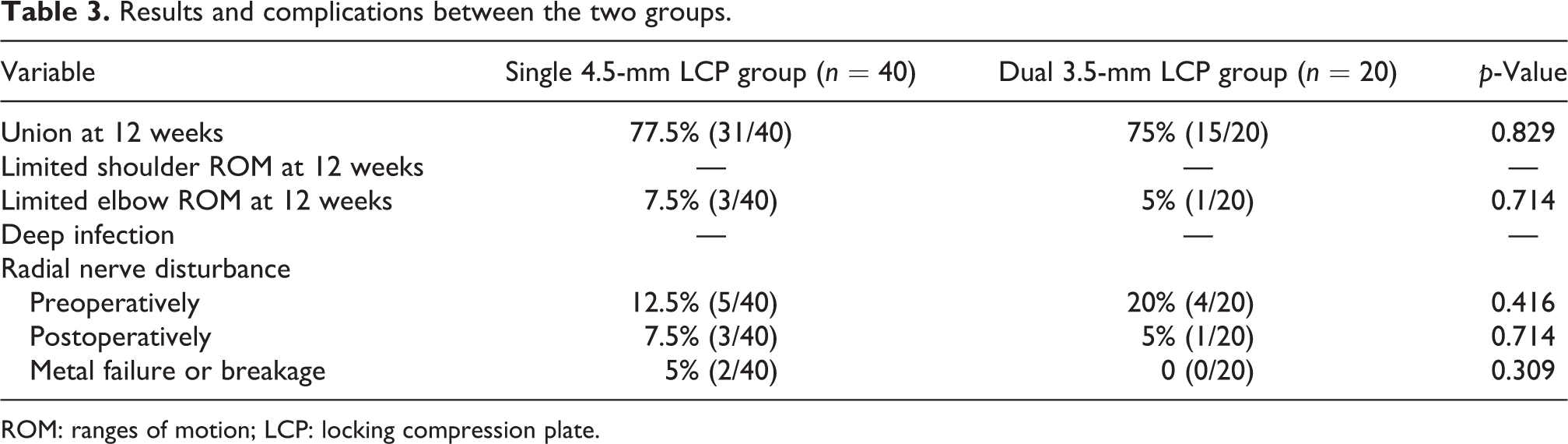
ROM: ranges of motion; LCP: locking compression plate.
Union was observed 12 weeks after surgery in 15 (75%) of the 20 patients in the dual plating group. Five patients (25%) had longer healing times during follow-up. No metal failure and nonunion were observed in the dual 3.5-mm LCP fixation group (Table 3).
Full ROM of the shoulder was restored at 12 weeks after surgery in both groups. Three patients (7.5%) in the single plating group had slightly reduced elbow ROM at 12 weeks after surgery. One patient (5%) in the dual plating group had a slightly reduced elbow extension at 12 weeks after surgery, although full elbow ROM was restored at 24 weeks after surgery (Table 3).
Complications
Three patients (7.5%) in the single plating group and one patient (5%) in the dual plating group developed radial nerve palsy after surgery, probably owing to operative manipulation. Three patients in the single plating group returned to normal function from 6 to 12 weeks after surgery. One patient in the dual plating group recovered from radial nerve palsy after receiving neurotrophic drugs at 24 weeks after surgery. No vascular injury and deep infection were observed in either group (Table 3).
Discussion
In this study, humeral shaft fractures treated with dual 3.5-mm LCP fixation showed satisfactory union rates, ROM, and complication rates, without increasing surgical time, in comparison with the conventional single 4.5-mm LCP fixation.
Given the increased rate of operative fixation of humeral shaft fractures, a large fragment plate construct is considered the standard for internal fixation. 11 Use of 4.5-mm standard cortical bone screws in large fragment plates is generally successful with recommendations that three to five screws be implanted proximally and distally. 6 Particularly for the humeral shaft fractures, at least four screws are required on either side of the fracture site. 12
Since the 19th century, dual plating for long bone fracture management has been used. 13 Dual plating techniques in humerus fracture management are rarely reported. Choi et al. 14 introduced a dual plate fixation technique for comminuted proximal humerus fractures. Lee et al. 1 and Prasarn et al. 15 described that satisfactory outcomes were achieved from dual plate fixation of distal diaphyseal humeral fractures. However, in some patients with smaller humeri, the diaphyseal shaft length and/or diameter available for fixation are limited, consequently making it difficult to use large fragment plates. The difficulty of adjusting the number of screws that can be placed on plates, the undesirable stress shielding with bulky fixation 5 , and the need for pre-contouring of the plate to match the diverging anatomy of the metaphysis of the humeral shaft are the drawbacks of using large fragment plates. Recently, several in vitro studies have been reported. Watts et al. 6 described that the use of dual plates is better than large fragment plates in respect of yielding better mechanical properties. Karakasli et al. 4 and Kosmopoulos et al. 7 also reported that 3.5-mm dual plating showed sufficient mechanical properties through various plate configurations. Moreover, Gausden et al. 16 reported an in vivo study that the triceps-sparing posterior approach to the humerus with a 3.5-mm pelvic reconstruction plate and 3.5-mm distal humerus dynamic LCP resulted in a low incidence of secondary radial nerve palsy and high union rates.
Plates typically are implanted using either a posterior or anterolateral approach. The posterior approach allows observation of the posterior and lateral plate placement and fractures directly, but because the nerve is in the middle of the operative fields, the nerve needs to be dissected carefully. 16 By contrast, the anterolateral approach avoids direct observation of the nerve and allows for anterior and lateral plate placement. Moreover, orthogonal plate configuration with eight- to four-hole construction is recommended in previous biomechanical studies. 4,7 Therefore, all the patients in the dual 3.5-mm LCP fixation group were treated with orthogonal plate configuration and eight- to four-hole construction (anterolateral aspect eight holes and anteromedial aspect four holes) through the anterolateral approach.
When using a single plate, absolute stability can be obtained with longer conventional large fragment plates, and extensive skin and soft dissection are inevitably needed. 17 By contrast, dual plate fixation can be performed with a smaller incision and less working length than one large fragment plate. 1 Especially partial release of the deltoid insertion is inevitable in anterolateral plating. Although no statistical difference in clinical outcomes was detected, partial release can be the source of postoperative shoulder pain or abduction weakness.
Increasing of screw number is inevitable in dual 3.5-mm LCP fixation, at least 12 screws are necessary for 8- to 4-hole construction. Even though increasing of screw number, there was no increase in surgical time. This result is considered as saving the reduction time, reduction of complex fracture is not easy without temporary fixation. Reduction plate technique with anteromedial short 3.5-mm LCP is useful for maintaining reduction. Archdeacon et al. 18 have termed the technique of unicortical fracture fixation plates applied to maintain reduction until definitive fixation as reduction plating. The humerus contains a deltoid tubercle on its lateral aspect, which continues distally as a cylindrical-shaped shaft, and it has widened epicondyles at the distal portion to form the medial and lateral of the humerus. 19,20 Therefore, plate contouring is necessary for anterolateral plating, Kosmopoulos et al. 7 also described that the 3.5-mm plate is easier for plate contouring than the 4.5-mm plate, and the 3.5-mm plating requires a smaller working length than the 4.5-mm plating. Although a lateral dissection of the anterolateral 3.5-mm plate fixation can be reduced than 4.5-mm plating, medial side soft-tissue dissection is necessary for orthogonal plate configuration (anteromedial and anterolateral). Even though additional medial side soft-tissue dissection, there were no differences of union rate at 3 months after surgery and nonunion rate.
This study has several limitations. First, this study was a retrospective study, and only 20 patients were included in the dual 3.5-mm LCP fixation group. However, the sample size of the control group was sufficient for comparison. A retrospective power analysis determined that 16 patients were needed in each group to obtain a 10% difference between the groups, with an α level of 0.05 and a β value of 0.80. Second, the cases with six-cortex fixation on either side of the fracture site were not excluded in the single 4.5-mm LCP fixation group, although eight- to four-hole construction was performed in all patients in the dual 3.5-mm LCP fixation group. Third, polytrauma, including ipsilateral upper extremity fractures, was not excluded only except for around elbow injuries. Therefore, the comparison of clinical outcomes between the two groups was limited.
Although several in vitro biomechanical studies of dual 3.5-mm LCP fixation have been reported, to our best knowledge, this is the first in vivo study that reports the clinical and radiological outcomes of dual 3.5-mm LCP fixation through an anterolateral approach. 4,6,7
Conclusion
Dual 3.5-mm LCP fixation to the humerus is a possible treatment choice for diaphyseal humeral fractures. As our initial hypothesis, this method showed satisfactory union rate, ROM, and complication rate, without increasing of surgical time, in comparison with the conventional single 4.5-mm LCP fixation.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.