
Abstract
Purpose:
To compare the hindfoot correction using clinical and ultrasonography assessment in clubfoot patients undergoing Achilles tendon tenotomy with patients corrected with casting alone.
Method:
A prospective observational study on idiopathic clubfoot patients less than 3 months old. Clinical assessment was done using hindfoot Pirani score and measurement of ankle dorsiflexion. Serial ultrasonography was done to measure the length and thickness of the Achilles tendon pre-hindfoot correction, 3 and 6 weeks post-hindfoot correction. Independent t-test was used to analyse the increase in ankle dorsiflexion, improvement in length and thickness of Achilles tendon between the two groups. Mann–Whitney U test was used to analyse the improvement in hindfoot Pirani score. Pearson correlation test was used for correlation in between clinical severity and ultrasonography assessment.
Results:
Twenty-three patients with bilateral clubfoot and four with unilateral clubfoot were recruited with a total of 50 clubfeet. Each group consists of 25 feet with a mean age of 2 months. Marked improvement in hindfoot correction was noted in tenotomy group compared to non-tenotomy group as evidenced by significant increase in Achilles tendon length, ankle dorsiflexion and improvement of hindfoot Pirani score. No significant difference in Achilles tendon thickness was noted between the two groups. Positive correlation was demonstrated between increase in Achilles tendon length and increase in ankle dorsiflexion as well as improvement in hindfoot Pirani score.
Conclusion:
We would like to propose Achilles tendon tenotomy in all clubfoot patients as it is concretely evident that superior hindfoot correction was achieved in tenotomy group.
Introduction
Clinical severity of the clubfoot is commonly assessed with Pirani scoring which has been proven to be a reliable assessment tool in evaluating the outcome of the clubfoot treatment. 1 Ponseti method is the widely accepted treatment regime which involves manipulation, serial casting with or without percutaneous Achilles tendon tenotomy. 2 Hindfoot rigid equinus is the most difficult deformity to correct due to the shortening of the Achilles tendon in clubfoot patients. 3
The importance of the successful hindfoot correction for good outcome and prevention of the relapse of rigid equinus have been highlighted in the literature. 4,5 In addition, based on a retrospective review of 221 clubfeet, Marleix et al. have advocated Achilles tendon tenotomy for all clubfoot patients regardless of the severity of the clubfoot as significant improvement in results was observed in group of clubfoot patients who underwent Achilles tendon tenotomy with a lesser rate of secondary surgery compared to group of patients who were corrected with casting alone. 6
Hence in this study, we would like to compare the hindfoot correction in a group of clubfoot patients undergoing Achilles tendon tenotomy with a group of patients whereby correction is achieved by casting alone. To our knowledge, no study has been previously conducted to compare the hindfoot correction, changes in the length and thickness of Achilles tendon throughout Ponseti regime in these two groups of patients. This research will be a pioneer study in the field of hindfoot correction in clubfoot patients.
Materials and methods
A prospective observational study was conducted in University Malaya Medical Centre (UMMC) clubfoot clinic from January 2017 to May 2018. Newly diagnosed idiopathic clubfoot patients less than 3 months old within the study period were recruited. The exclusion criteria were positional clubfoot, recurrent or complex clubfoot, patients with neurological disorder, arthrogryposis, metatarsus adductus and other foot deformities.
All the patients were started on serial casting based on the Ponseti method. After successful forefoot and midfoot correction, the patients were divided into two different groups based on clinical assessment by the same paediatric orthopaedic surgeon. Patients with ankle dorsiflexion less than 15° will undergo percutaneous Achilles tendon tenotomy (Group A), meanwhile patients with ankle dorsiflexion 15° and above will be corrected via casting alone (Group B). There was no difference in terms of age, gender, body weight and other socio-demographic factors between both the groups.
Parents were explained in detail regarding the study and procedures by the same paediatric orthopaedic surgeon and informed consent was taken from them. Ethical approval for this study was obtained from the UMMC Medical Research Committee. Twenty-seven patients were recruited in the study with a total of 50 feet (25 feet per group). All casting and bedside percutaneous Achilles tendon tenotomy were done by the same paediatric orthopaedic surgeon to prevent inter-observer bias. Ultrasonography assessment was done by a radiologist who was blinded to the procedures. The clinical assessment of hindfoot correction post-procedure was done by a different paediatric orthopaedic surgeon who was also blinded to prevent bias.
GE Venue 40 ultrasound machine (GE Health care , Milwaukee, Wisconsin, US), L8-18i-SC wide band linear transducer with an imaging frequency of 8–18 MHz was used to measure the length and thickness of the Achilles tendon. Ultrasound was done using the same technique for all the patients. Patient’s ankle was dorsiflexed maximally to make the Achilles tendon taut. The tendon was measured longitudinally from the calcaneum insertion point until the musculo-tendinous junction of medial gastrocnemius as shown in Figure 1 to measure the length of Achilles tendon. 7 Besides that, the thickness of the Achilles tendon was measured 0.5 cm from the calcaneal insertion point to compare the changes in thickness of the tendon in both group of patients.

Ultrasonography measurement of Achilles tendon length (measured from calcaneum insertion point until the musculo-tendinous junction of medial gastrocnemius).
Prior to hindfoot correction, baseline ultrasound scan of the tendon was done. Subsequently, the scans were repeated 3 weeks after Achilles tendon tenotomy in Group A patients and after 3 weeks of the final casting in Group B patients. The scans were also done in both groups after 6 weeks of hindfoot correction. The difference between values during 6 weeks post-correction and pre-hindfoot correction was used to assess the improvement in length and thickness of Achilles tendon. These measurements were done based on the ultrasonography evidence of continuity of tendon which has been demonstrated within 3–6 weeks after tenotomy. 8,9
Clinical assessment of hindfoot correction was done using the established hindfoot Pirani score and measurement of the ankle dorsiflexion. Passive ankle dorsiflexion was done by applying pressure over the head of metatarsals and the quantitative measurement was done using goniometer. The improvement in hindfoot Pirani score and ankle dorsiflexion was measured using the difference between values during 6 weeks post-correction and pre-hindfoot correction.
Data were analysed using SPSS version 25. Independent t-test was used to analyse the increase in ankle dorsiflexion, improvement in length and thickness of Achilles tendon between the two groups of patients. Mann–Whitney U test was used to analyse the improvement in hindfoot Pirani score (%). Pearson correlation test was used for correlation in between clinical severity and ultrasonography assessment. The statistical analysis was conducted with 95% of confidence interval and a p value of <0.05 as threshold of statistical significance.
Results
Twenty-three (85.2%) patients with bilateral clubfoot and four (14.8%) with unilateral clubfoot were recruited with a total of 50 clubfeet. Groups A and B both consist of 25 clubfeet each. There were 14 (51.9%) male and 13 (48.1%) female patients. The mean age of the patients was 2 months and the mean body weight was 3.8 kg. There was no significant statistical difference in terms of age, gender, body weight and other socio-demographic factors between the two groups.
Marked improvement in hindfoot correction was noted in Group A patients compared to Group B as evidenced by significant increase in Achilles tendon length (Figure 2), ankle dorsiflexion (Figure 3) and improvement of Hindfoot Pirani score. However, there was no statistical significant difference in increase of Achilles tendon thickness between the two groups. The statistical analysis of these parameters is described in Table 1.
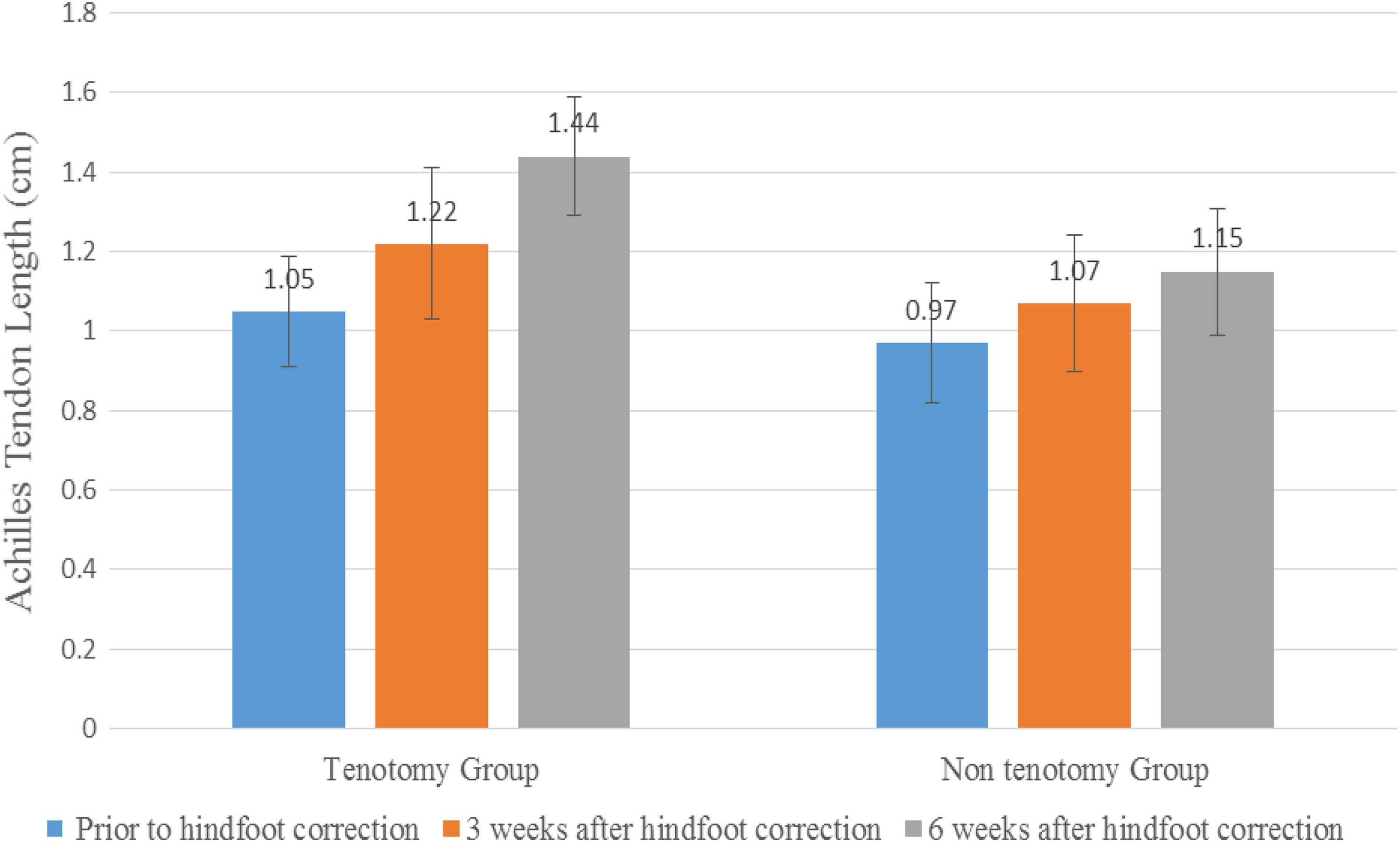
Comparison of the mean value of Achilles tendon length prior to hindfoot correction, 3 and 6 weeks after hindfoot correction in both group of patients.
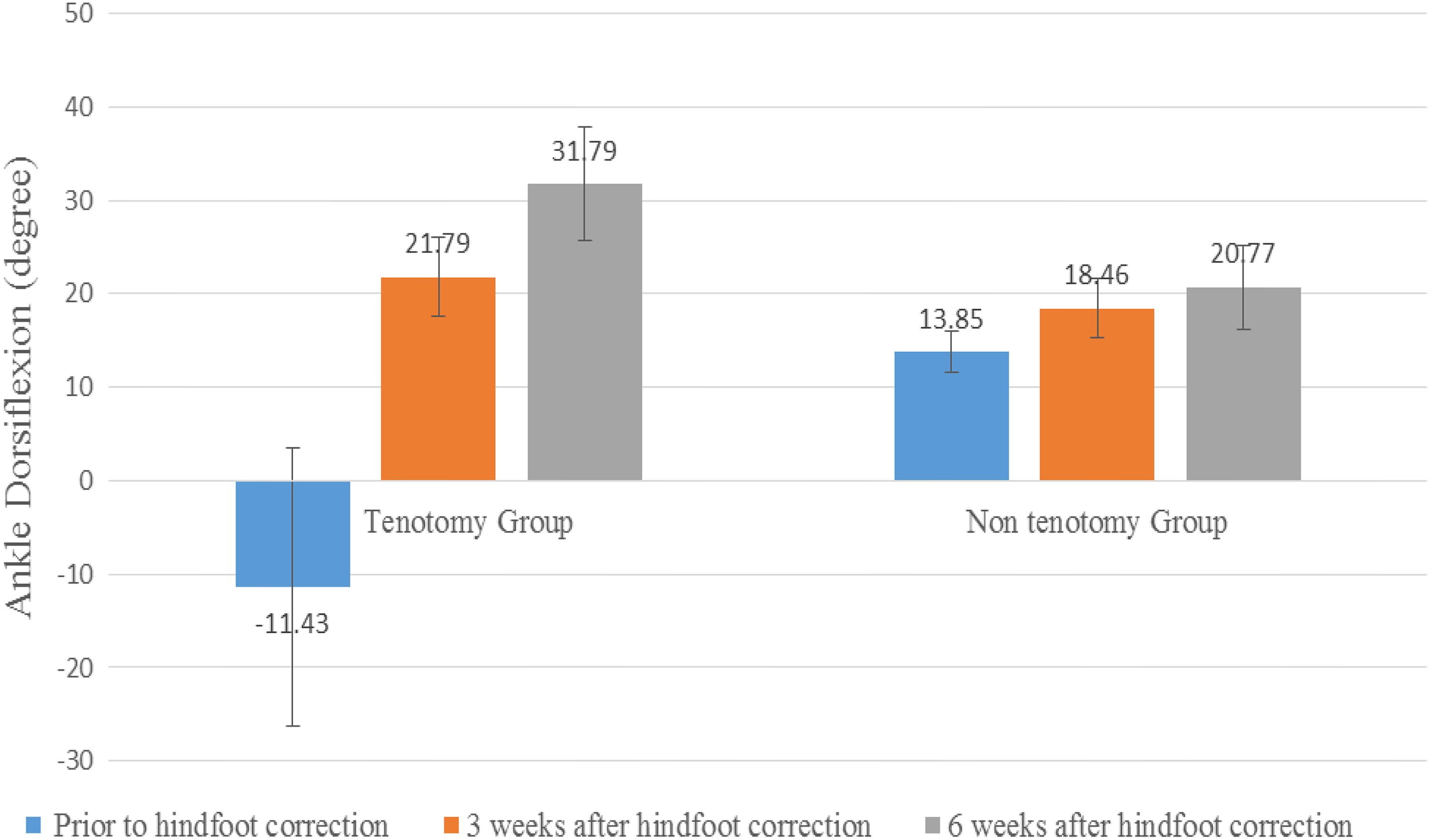
Comparison of the mean value of ankle dorsiflexion prior to hindfoot correction, 3 and 6 weeks after hindfoot correction in both group of patients.
Hindfoot correction comparison between tenotomy and non-tenotomy group.

SD: standard deviation.
aIndependent t-test.
bMann–Whitney U-test.
Positive correlation was demonstrated between improvement in clinical severity (Hindfoot Pirani score) and increase in Achilles tendon length as shown in Figure 4. Apart from that, significant positive linear relationship was also shown between increase in ankle dorsiflexion and increase in Achilles tendon length as demonstrated in Figure 5.

Correlation between increase in length of Achilles tendon and improvement in hindfoot Pirani score.

Correlation between increase in length of Achilles tendon and increase in ankle dorsiflexion.
Discussion
Ponseti method is currently accepted as the gold standard treatment for idiopathic clubfoot which has a remarkable correction rate and an excellent functional outcome. 2,10,11 Equinus deformity is only addressed after fully correcting the cavus, adductus and varus deformity. Hindfoot deformity can be corrected via Achilles tendon tenotomy or casting alone. Theoretically, the tendon creep potential allows permissive lengthening of Achilles tendon during manipulation and casting. 12 Achilles tendon tenotomy is done as a part of the protocol in Ponseti technique if the ankle dorsiflexion is less than 10–15° after successful forefoot and midfoot correction. 11,13
Percutaneous Achilles tendon tenotomy is a bedside procedure which is relatively safe with very minimal complications reported. 6,14 Evaluation of the tendon healing property has been done extensively with dynamic and static ultrasonography in the literature. Spontaneous healing of Achilles tendon has been reported to occur within 6 weeks after tenotomy. 8,9 Studies on ankle power and gait analysis in post-tenotomy patients have negated the possibility of any unfavourable impact of Achilles tendon tenotomy in clubfoot patients. 15 –17
Clinical severity of the hindfoot deformity is an established predictive factor of relapse in clubfoot apart from non-compliance to brace. 4,5,18,19 Hindfoot correction plays a vital role in the management of clubfoot as incomplete correction will result in dire consequences. In this study, we have used clinical as well as ultrasonography assessment to compare the hindfoot correction between the patients who undergo tenotomy and patients corrected by casting alone.
Besides hindfoot Pirani score, measurement of ankle dorsiflexion is commonly used in studies to determine the severity of the hindfoot deformity and to assess the correction in clubfoot patients. 20,21 The mean ankle dorsiflexion achieved 6 weeks post-tenotomy in our study was 31.79° as opposed to 20.77° in the non-tenotomy group. The statistically significant improvement of ankle dorsiflexion in the tenotomy group as shown in Table 1 implies that better hindfoot correction was achieved in patients undergoing percutaneous Achilles tendon tenotomy. Our results were comparable to a study of radiographic evaluation of idiopathic clubfeet conducted in 2007 in which Radler et al. had augmented the improvement of ankle dorsiflexion observed in post-tenotomy patients. 20
Ultrasonography measurement of Achilles tendon length in this study enables us to have an objective assessment of the hindfoot correction. 22 The increase in Achilles tendon length in patients undergoing tenotomy was statistically significant compared to patients treated with casting alone. This was reiterated by the positive correlation shown between the increase in Achilles tendon length and the improvement in the ankle dorsiflexion. Similar relationship was demonstrated between the two parameters in a cadaveric study done in 2006. 23 Studies on measurement of Achilles tendon length in clubfoot have been scarcely reported in the literature. Bialik et al. in 2006 have conducted a research on Achilles tendon length in 101 normal and clubfoot patients; however, the focus of the study was to assess the flexibility of the tendon and need of tenotomy. 22
There was no significant difference in the increase of thickness of Achilles tendon between the two groups of patients in our study. Similar outcome was obtained by Agarwal et al. in 2012, in which the ultrasonography evaluation of the thickness and size of the Achilles tendon in clubfoot patients before and after tenotomy showed no significant difference. 8
Our limitation will be the short duration of study conducted in a single institution. A longer follow-up study in future would provide more information on functional outcome and relapse in these group of patients.
Conclusion
Based on our clinical and ultrasonography assessment, marked improvement of hindfoot Pirani score, ankle dorsiflexion and Achilles tendon length demonstrates that superior hindfoot correction was achieved in patients undergoing tenotomy compared to casting alone. Hence, we would like to propose percutaneous Achilles tendon tenotomy in all clubfoot patients for better hindfoot correction.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.