
Abstract
Purpose:
Metaphyseal, proximally anchored uncemented stems for total hip arthroplasty provide bone preservation and decrease the incidence of proximal stress shielding and thigh pain. Our study investigated the clinical and radiological outcome of the DePuy Proxima™ short stem at a minimum of 7 years.
Methods:
Eighty-one consecutive patients (86 procedures) under the age of 70 undergoing primary total hip replacement at two arthroplasty centres were enrolled. Follow-up was clinical (Harris Hip Score (HHS), thigh pain and satisfaction) and radiological (subsidence, malalignment and loosening) at 6 months and yearly thereafter.
Results:
Average age was 50 (range 32–65) with 79% (68 of 86) being male. Preoperative diagnosis included primary osteoarthritis (OA) 36%, avascular necrosis of femoral head 51%, dysplasia 9% and post-traumatic OA 4%. HHS improved 51 points at latest follow-up (from 40 to 91). We had 3.5% (3 of 86) periprosthetic fractures, one requiring revision. We had one dislocation, no infections and no thigh pain. Malalignment rate (≥5° off neutral) was 12% (10 of 86), not affecting clinical results.
Conclusion:
Overall stem survival was over 97% at 7 years. The DePuy Proxima provides excellent clinical results at a minimum of 7 years post-operatively.
Introduction
Total hip arthroplasty (THA) is arguably the most successful orthopaedic intervention performed in large numbers today. The indications for surgery have expanded to patients who are young and active and are suffering from debilitating degenerative disease of the hip. 1 Using cementless fixation has gained popularity in the last two decades and is undoubtedly the fixation of choice in the United States today (≥90%). In the United Kingdom, fully uncemented THA has overtaken fully cemented THA in 2008, as the most popular fixation combination, while hybrid fixation has recently gained popularity. 2 Using an uncemented stem carries the risk of exposing the patient to potential thigh pain, the incidence of which is variable, depending on stem design, but can be more than 11%, 3,4 and proximal stress shielding, which is frequently seen with stems which load in the diaphysis. Avoiding the above issues and preserving bone stock for potential future revision procedures have led to the development of short metaphyseal stems that offer a more proximal fixation in the metaphyseal cancellous bone. These stems have the advantage of potentially allowing for a future revision using conventional primary stems. 5 As most of these short stems are relatively new, there is little evidence regarding their medium-term clinical and radiological outcome. A recent review has found that less than a quarter of the studies reporting on metaphyseal stems have a follow-up period exceeding 5 years. 6
We report our medium-term results with the use of the Proxima™ stem in THA, clinically evaluating our first 86 consecutive cases. We hypothesized that medium-term Proxima stem results are comparable with traditional uncemented stems without thigh pain and frequent major complications.
Materials and methods
Consecutive patients undergoing total hip replacement (THR) in two large regional arthroplasty centres were enrolled in our study. The study began in September 2006 shortly after the introduction of this particular lateral flare design stem and lasted till May 2011. Patients required to fulfil inclusion criteria to be considered for the use of the Proxima (DePuy, Leeds, UK) short stem. The Proxima stem is made of forged titanium alloy, with a Duofix™ (DePuy, Warsaw, Indiana, USA) hydroxyapatite (HA) (porous coating and HA) surface coating. Nine sizes of standard as well as high-offset stems for each side are available. Cementless Duraloc™ (DePuy, Leeds, UK) porous-coated cups (DePuy) with 10° lipped polyethylene liners and 28-mm metal or ceramic heads were used in all cases.
Patients met inclusion criteria if they were relatively young (age less than 70 years of age), were active (working part- or full-time), were not suitable for a resurfacing procedure and had one of the following diagnoses in their hip: hip primary osteoarthritis (OA), avascular necrosis (AVN) of the femoral head, secondary OA due to mild-to-moderate hip dysplasia or previous trauma.
Exclusion criteria were preoperative templating showing small stem size (size one or two) for patients whose weight was over 100 kg, severe hip dysplasia, previous hip osteotomy or other acquired femoral deformity, a cortical index (diameter of the femur minus the diameter of the femoral canal 10 cm below the lesser trochanter, divided by the diameter of the femur at the same level, times 10) less than 3 and severe osteoporosis.
Basic demographics were collected, including age, gender and weight. All patients were followed up clinically and radiologically at 6 weeks, 6 months, 1 year and yearly thereafter. Clinical follow-up included recording all complications (acute myocardial infarction, deep vein thrombosis, pulmonary embolism, periprosthetic fracture, dislocation, neurovascular injury, etc.). Patient outcome was documented using the Harris Hip Score (HHS) 7 and potential thigh pain was also noted separately. Radiological assessment was performed with the use of standardized pre- and post-operative radiographs. Radiological examination focused on established issues, such as subsidence, implant malposition, loosening, proximal stress shielding and implant survivorship. Implant migration was assessed according to Martell et al. 8 Implant stability was evaluated according to Engh et al. 9 based on the radiological features of the bone–implant interface. Criteria for radiological loosening of the implant were defined as a radiolucent zone greater than 3 mm or a horizontal and/or vertical migration greater than 2 mm with an adjacent radiolucent zone. 10 Stem alignment was rated as normal if its deviation from the axis of the femoral shaft was 5° or less. A deviation of 6–10° was rated as ‘varus’ or ‘valgus’ and a deviation exceeding 10° was rated as ‘severe varus’ or ‘severe valgus’. All procedures were performed by two experienced arthroplasty surgeons, using the same (supine) position, and utilizing an anterolateral approach, with a minimized exposure, using a routine operating table, with no image intensifier. Patients received the same low molecular weight heparin for 42 days post-operatively as the method of thromboprophylaxis. Patients were allowed to partially weight-bear, using crutches from the first post-operative day, and were allowed to fully weight-bear after 4 weeks post-operatively.
Results
During the 5-year period, 81 patients undergoing 86 procedures met our inclusion criteria. Basic demographic data can be found in Table 1. The majority of patients either had primary OA (36%; 31 of 86) or AVN of the femoral head (51%; 44 of 86), with the remainder having mild dysplasia (9%; 8 of 86) or post-traumatic OA (4%; 3 of 86). Functional outcome was assessed with the use of the HHS. Preoperative and post-operative HHS values are demonstrated in Table 2.
Basic demographic data.
HHS values during the study.
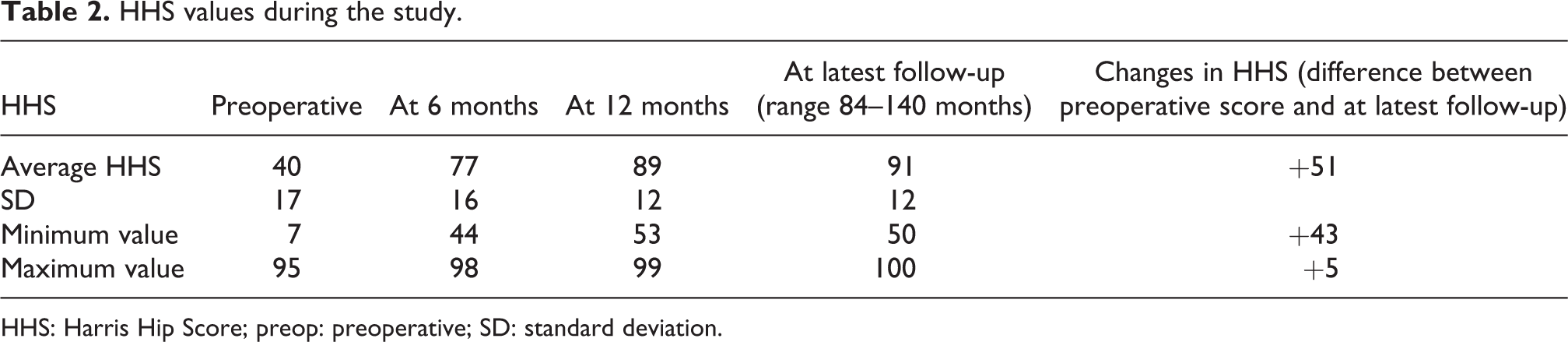
HHS: Harris Hip Score; preop: preoperative; SD: standard deviation.
Complications
During the study, two patients died of an acute coronary event unrelated to surgery, leaving 79 patients and 84 hips who completed the study, but all patients were included in the complication and radiological analysis. In terms of complications, we did not observe any infections, deep vein thrombosis or pulmonary embolism. We had two intraoperative periprosthetic fractures, requiring open reduction and internal fixation with a plate. One of these cases eventually required a revision. One patient had a post-operative Vancouver B1 periprosthetic fracture after adequate trauma. This fracture was treated conservatively, and the fracture healed uneventfully (although with a few millimetres of subsidence), with the patient being very happy with the result at 9.3 years post-operative, with an HHS of 40 preoperative and 91 at last follow-up (Figure 1(a) to (c)). The overall periprosthetic fracture rate was thus 3.5% (3 of 86). All fractures occurred in the first 20 cases. We had one dislocation, due to a cup malposition, where the cup required eventual revision, with the stem staying in situ. We did not observe any patients with thigh pain, during the study. At the latest follow-up all of the patients said that they would be happy to undergo the same procedure again.

(a) Immediate post-operative XR of left hip following uncemented THR using the Proxima short stem in a 48-year old male patient. (b) Three weeks after THR patient had a fall and suffered a Vancouver B1 periprosthetic femoral fracture. The fracture was treated conservatively. (c) At latest follow-up, 7 years after THR. The fracture has fully healed and remodelled. The hip function is excellently. THR: total hip replacement.
Radiological follow-up
We had one case of subsidence, where the reason for the change in the position of the stem was an undersized implant. This patient eventually required a revision procedure (Figure 2(a) and (b)). The main coronal alignment of the Proxima stem was found to be in severe varus (>10°) position on two occasions, while another eight stems were measured to be in varus (5–10°), giving an overall malalignment rate of 12% (10 of 86). The rest of the stems were in a normal position, as per our criteria. Other than the one subsided stem requiring revision, there was no femoral component loosening around our femoral components. Our overall survivorship for the Proxima femoral component at the end of the study (at an average of 9.3 years) was 98.8% (83 of 84), with failure due to aseptic loosening as the end point. The all cause stem revision rate at the end of the study was 2.4% (2 of 84). A 7-year Kaplan–Meier survival rate of 97.6% was determined for Proxima short stems (Figure 3).

(a) Two years after THR subsidence and osteolysis are visible around the Proxima stem in a 50-year-old male patient. (b) The uncemented short stem was revised to an Exeter stem. Patient is asymptomatic with excellent function. THR: total hip replacement.
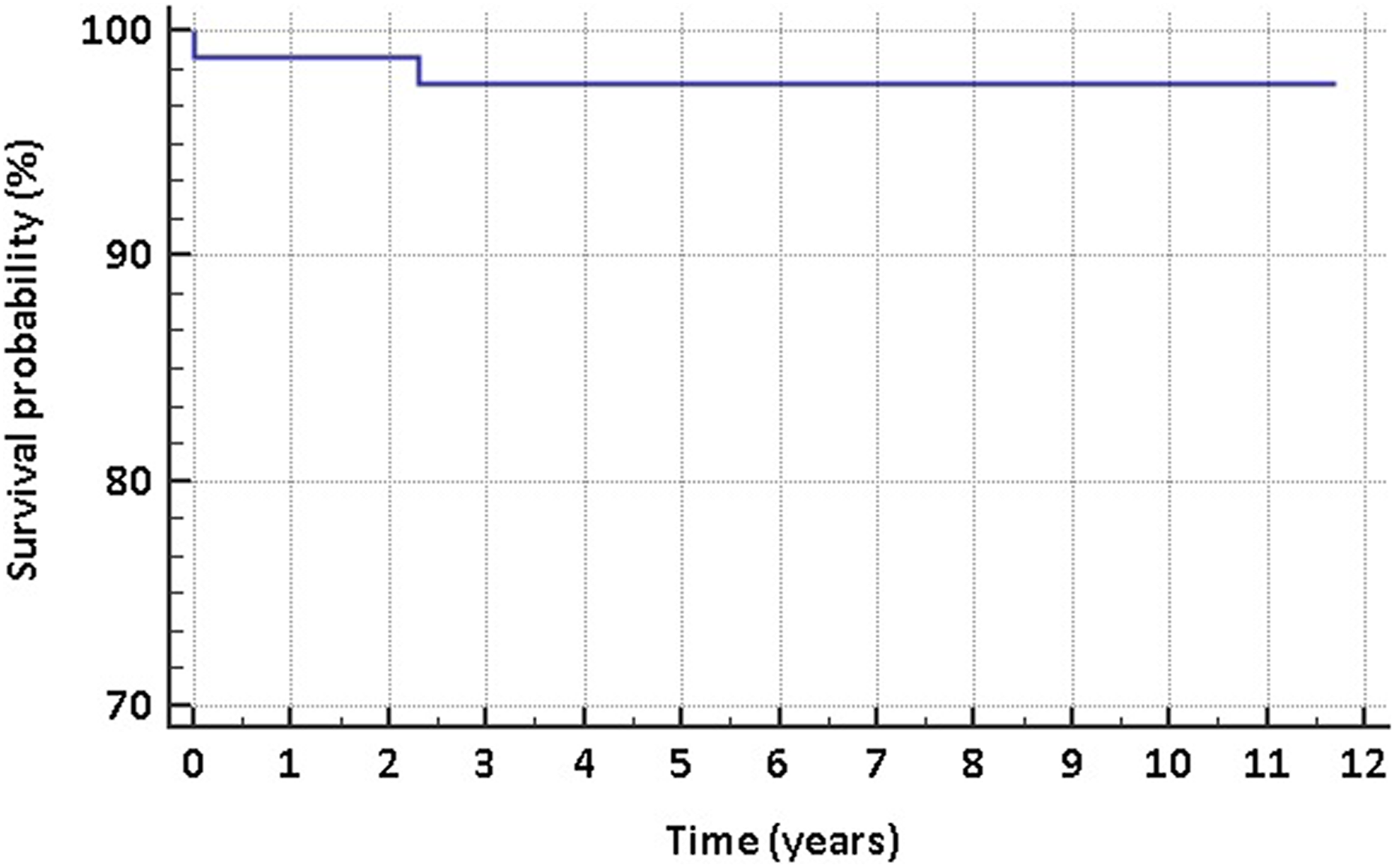
Graph to show Kaplan–Meier survivorship of the Proxima short stem.
Discussion
Uncemented short stems are very tempting proposition as they load the proximal femur more physiologically, 11 thus potentially avoiding thigh pain and proximal stress shielding. These implants also preserve proximal femoral bone stock and can be inserted in a minimally invasive fashion. However, skepticism exists regarding their use, due to several reasons, including the learning curve involved and potential complications such as stem malalignment, incorrect sizing, subsidence and intraoperative fractures. Furthermore, well-established uncemented stems offer reliable long-term results with a low complication rate. 12 Uncemented short stems need to establish that they have a comparably low complication rate to conventional uncemented stems and an equivalent survivorship if they are to gain widespread acceptance and use.
Our study demonstrated that at over 7 years follow-up, the Proxima stem performs very well, with all cause stem survivorship over 97%, which is on course to equal or better established guidelines by NICE which recommend only implants which have a maximum of 5% revision rate in the first 10 years following implantation. 13
Available literature on short stems shows a heterogenous picture. Some stems have proven to be reliable in the short term, 14 while studies of others showed varied results. 15 Early studies of the Proxima stem have focused on surgical technique, 16 migration pattern and bony integration using radiostereometric analysis and/or dual energy X-ray absorptiometry (DXA). 17 –19 There have been several clinical studies regarding this implant, but they are limited by either the length of follow-up 20 or the patient number. 21
Thigh pain is a common complaint following uncemented hip arthroplasty using conventional stems, with up to one in eight patients affected, some of which eventually require revision. 3 A recent review of short stems found a variable rate of thigh pain with various short-stem designs, with an overall thigh pain rate of 0.4%. 6 However, among the lateral flange designs such as the Proxima, no thigh pain was reported, and similarly we had no patients complaining of this particular complication.
Early periprosthetic fractures after uncemented THR are major complications and thus a serious concern when considering new implants. The frequency of intraoperative and early periprosthetic fractures (within 30 days) differs as per surgeons experience, but also by stem design, and can range from 0.3% to 2.5%, 22 although much higher numbers have been reported, over 5% for primary hips and 20% for revisions. 23 We experienced three periprosthetic fractures, giving us a 3.5% fracture rate. It has to be stressed that all fractures happened, among our first 20 cases, thus our learning curve constituted to their occurrence. Some technical points also need to be mentioned here, such as the level of femoral neck resection which should be more proximal and less oblique (flatter), to preserve proximal bone stock and to provide a wider entrance to the femoral canal. Ender et al. 24 reported a higher revision rate with the CUT™ (ESKA Implants, Lübeck, Germany) stem if a more diagonal (traditional) resection was performed. The around the corner technique required for the Proxima stem facilitates the use of minimally invasive approaches, but at the same time precludes the use of intramedullary guides and can also result in a varus position when the tip of the stem can touch the lateral cortex contributing to a potential fracture. During the learning phase, the use of fluoroscopy is advisable.
Malalignment (varus or valgus malalignment of ≥5°) of short femoral stems is not unusual and the reported incidence is over 20%. 6 With lateral flare design, such as the Proxima, malalignment seems to be less frequent, just over 14%. In our study, this was even lower at 12% (10 of 86). While varus or valgus alignment might contribute to early failure in conventional uncemented and cemented femoral stems (which at least partially are fixed in the diaphysis), the importance of this radiological finding remains to be seen with uncemented short stems. Malposition leads to a change in femoral offset, thus influencing the abductor lever arm. A stem positioned in varus also carries the risk of increasing the torque at the bone implant interface, which might increase the incidence of loosening. Long-term follow-up studies are needed to assess the effect of stem malposition on functional outcomes and survivorship.
Conventional uncemented stem designs are often associated with proximal femoral stress shielding and component migration. Outcome relates to these factors. 25 In our series, we did not observe any macroscopic bone mineral density change, although no formal bone mineral density measurement was undertaken routinely, thus our assessment is subjective. Neither vertical (subsidence) nor horizontal (change in varus or valgus malalignment) component migration was experienced apart from one stem, which was undersized and eventually subsided.
Functional outcome is paramount for both the patient and the surgeon. Our overall increase of 50 points in the HHS over the reported period is in line with previous reports. 16 In addition, all of our patients were satisfied and would undergo the operation again.
Our study has several weaknesses, most notably the lack of a control group. Our patient group was young (average age of 50 years), with some high-risk patient groups excluded (systemic inflammatory conditions and abnormal proximal femoral anatomy). However, it is still one of the largest series of this particular stem design, with a reasonably long medium-term follow-up. Our results are comparable with the established so-called conventional stem designs. Our complications were concentrated to the first 20 cases, that is, the learning curve.
Conclusion
We can state that midterm results of the Proxima short stem are comparable to traditional uncemented stems. In our experience, once the short but steep learning curve is passed, the implantation of the Proxima stem is safe and reproducible.
Further long-term prospective comparative studies are required to establish the role of short femoral stems in the treatment of end-stage OA of the young and active patient.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.