
Abstract
Purpose:
The aim of the present study was to investigate the correlations among the preoperative and postoperative knee laxity, the clinical results, and the type of remnant tissue following the anterior cruciate ligament (ACL) reconstruction.
Methods:
One hundred ninety-two patients (male, n = 101; female, n = 91; mean age, 27.1 years) with ACL-deficient knees who had undergone double-bundle reconstruction were included. The time between injury and surgery (TBIS) was 34.7 weeks (range, 1–504 weeks). The subjects were divided into four groups according to the Crain’s classifications and factors such as the age at surgery, gender, TBIS, side-to-side difference (SSD), Tegner activity score (TAS), and Lysholm score were compared.
Results:
The percentage of patients with ACL remnant pattern types 1, 2, 3, 4 was 19% (37 knees), 52% (101 knees), 9% (19 knees), and 18% (35 knees), respectively. The TBIS of the patients with Crain type 4 was significantly longer in comparison to the other groups (p < 0.01). A significant difference was observed in the preoperative SSD of the Crain type 3 and Crain type 4 (6.2 ± 3.4 mm, 9.3 ± 3.6, respectively) groups. The TBIS in patients with Crain type 4 was significantly longer in comparison to the other groups (p < 0.01). There were no significant differences between the groups in terms of the postoperative SSD, TAS, or Lysholm score.
Conclusion:
This study suggests that a Crain type 3 remnant was associated with a significantly lower preoperative SSD. In addition, the TBIS in patients with Crain type 4 was found to be significantly longer in comparison to the other groups.
Level of Evidence:
Level III, case–control study.
Keywords
Introduction
The anterior cruciate ligament (ACL) remnant has been reported to play an important role in anterior knee constraint, 1 proprioception, 2 and the biomechanical function. 3 According to the injury pattern and history, the ACL remnant may have different appearances and can be classified into four types according to the Crain description. 4 Maeda et al. 3 reported that a preserved type 3 remnant could increase anterior knee stability; however, the relationship between the types of preserved ACL remnant and the knee function has not been well documented. It remains unclear whether all types of ACL remnant are related to a positive result.
The aim of the present study was to investigate the correlations among the preoperative and postoperative knee laxity, the clinical results, and the type of remnant tissue following the ACL reconstruction. The authors hypothesized that the different remnant types would be associated with different results.
Materials and methods
Two hundred ten consecutive patients with ACL-deficient knees who underwent double-bundle (DB) reconstruction between April 2013 and August 2015 were evaluated. Patients who underwent ACL reconstraction in both knees and those with an open physis were excluded from the study. Patients who showed a concomitant grade 3 medial collateral ligament injury or grade 3 lateral collateral ligament injury were also excluded. Postoperative three-dimensional (3-D) computed tomography (CT) was performed in all cases to rule out malposition of the tibial and femoral tunnels. The final study population included 101 men and 91 women. The time between injury and surgery (TBIS) was 34.7 weeks (range, 1–504 weeks). The present study was approved by the internal review board of the authors’ institution (no. 29022001).
Arthroscopic evaluation
The configuration of the ACL remnant and its attachments to the femur and tibia was classified into one of four types according to Crain’s method of classification 4 : the ACL was wrapped around the PCL (type 1), the ACL was observed to have healed to the roof of the notch (type 2), the ACL remnant appeared to have healed to the lateral wall of the notch or the medial aspect of the lateral femoral condyle in a position anterior and distal to the ACL anatomic footprint (type 3), or no identifiable ligament tissue remained (type 4; Figure 1). There were no knees in which the remnant tissue had completely disappeared. The presence of a concomitant cartilage injury and meniscus (none, meniscal repair, partial meniscectomy, and subtotal meniscectomy) injuries was also evaluated.
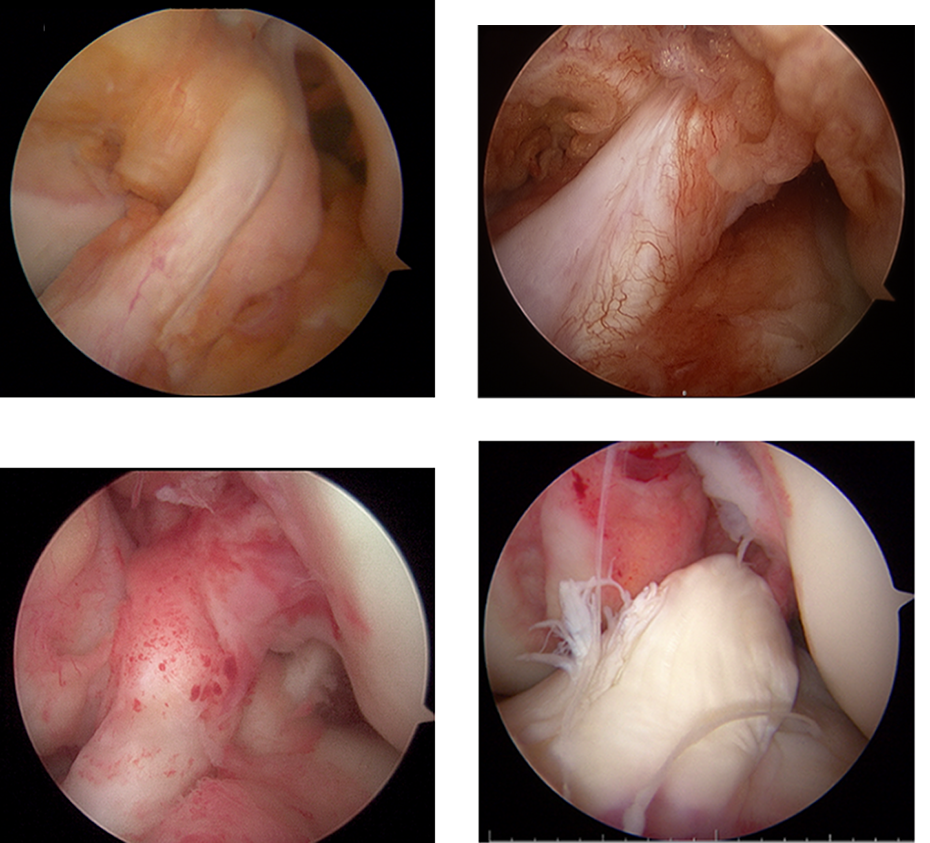
Classification of remnants (types 1, 2, 3, and 4).
There were 87 torn medial menisci and 80 torn lateral menisci. Seventy-four of the medial meniscal tears were repaired, 13 were treated with partial meniscectomy. Fifty-two of the lateral meniscal tears were repaired, 28 were treated with partial meniscectomy.
The surgical procedure for remnant preserving DB reconstruction
Anatomic DB ACL reconstraction was performed using a hamstring tendon according to the concept of anatomic DB reconstruction. 5 If the diameter of either the anteromedial (AM) or posterolateral (PL) graft was <5 mm, the gracilis tendons were added. An EndoButton CL device (Smith & Nephew Endoscopy, Andover, Massachusetts, USA) was attached at the looped end, and a Telos artificial ligament (Telos, Marburg, Germany) was attached at the other end.
Only the residual tissue of the normal femoral attachment area was peeled off from the bony surface using a monopolar radiofrequency probe. Femoral tunnels were made behind the resident’s ridge, 6,7 just anterior to the cartilage margin. The outside-in technique was used to make the AM and PL tunnels.
The tibial remnant of the ACL was preserved as it was without any removal. The two guide wires were placed within the remnant tissue. It was decided that the AM tibial tunnel insertion should be lateral to the medial intercondylar ridge and posterior to the transverse ligament or Parsons’ knob 8 at 90° of knee flexion. A 2.4-mm guide wire was inserted into the AM tunnel. A 5.0–7.0-mm tunnel was then drilled over the guide wire for the AM tunnel. A 2.4-mm guide wire for the PL tunnel was then inserted slightly posterolateral from the AM tunnel. Stapling was performed on the tibial side at 30° of knee flexion for graft fixation. Tibial fixation of the AM and PL bundles was carried out with 30 N of traction applied to each bundle 9 (Figure 2).
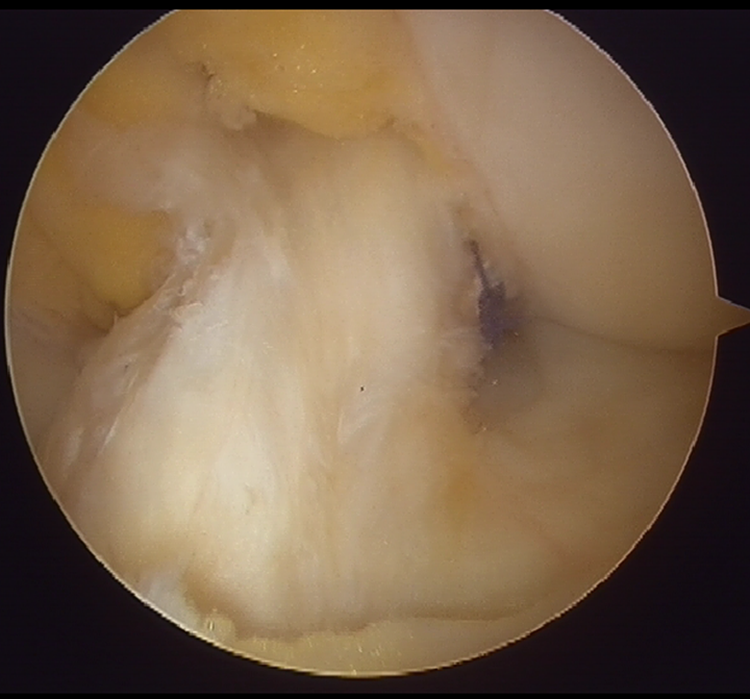
Double-bundle reconstruction with remnant tissue preservation. The AMB was not visible because it was covered by the remnant tissue. AMB: anteromedial bundle.
Postoperative rehabilitation
A continuous passive motion machine was used from day 2. Partial weight-bearing activity (one-third of the patient’s body weight) was permitted from week 2. Full body weight-bearing was permitted from week 4. Jogging was started from 4 months after surgery. Full-speed running was allowed at 6 months after surgery. A complete return to competitive sports was then allowed at 8 months after surgery.
Postoperative evaluation
All of the patients underwent a clinical examination at 1 year after surgery. We examined the side-to-side difference (SSD) of the anterior translation using a Telos device, the Lysholm score, and the Tegner activity score (TAS). 10
Computed tomographic evaluations
The location of the tunnel
At 2 weeks after surgery, the femoral tunnel position was measured by the femoral quadrant method, and the tibial tunnel position was measured by the tibial quadrant method using 3-D CT. 11 The locations of the anteromedial femoral tunnel, posterolateral femoral tunnel, anteromedial tibial tunnel, and posterolateral tibial tunnel were measured.
Statistical analyses
The subjects were divided into four groups according to their Crain’s classifications. A one-way analysis of variance and the Tukey’s honestly significant difference test were used for comparisons between groups. All of the statistical procedures were conducted using the SPSS software program (version 19.0 J; SPSS Inc). p Values of <0.05 were considered to indicate statistical significance.
A post hoc analysis was performed using a one-way analysis of variance. The G-Power 3.1 software program was used to perform the analysis. 12 Post hoc tests showed that the power regarding the preoperative SSD was 0.80 with a significance level of 0.05.
Results
The demographic and clinical characteristics of each group are shown in Table 1.
The patient demographics and preoperative data.
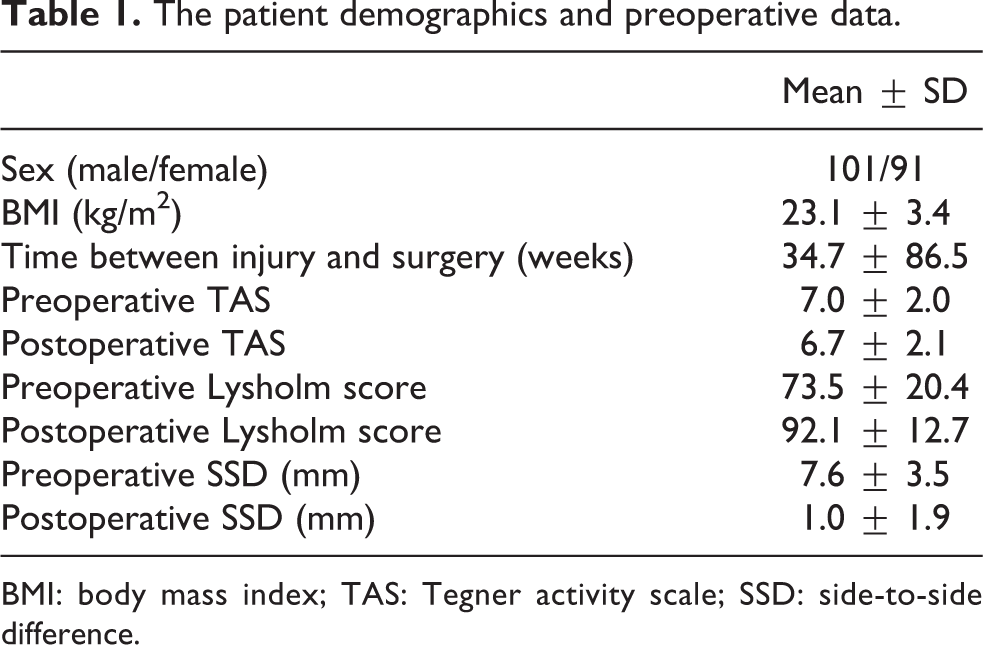
BMI: body mass index; TAS: Tegner activity scale; SSD: side-to-side difference.
The percentage of the patients who were classified as having ACL remnant pattern types 1, 2, 3, and 4 was 19% (37 knees), 52% (101 knees), 9% (19 knees), and 18% (35 knees), respectively. The age, gender, and body mass index values of the patients in the four groups did not differ to a statistically significant extent. The TBIS of the patients with Crain type 4 was significantly longer in comparison to the other groups (p < 0.01). A significant difference was observed in the preoperative SSD of the Crain type 3 and Crain type 4 (6.2 ± 3.4 mm, 9.3 ± 3.6, respectively) groups. The postoperative SSD, TAS, and Lysholm score of the four groups did not differ to a statistically significant extent. Significant differences were observed in the pivot shift test results of the four groups. The location of the tunnel in the four groups did not differ to a statistically significant extent (Table 2).
The clinical findings for each group.

BMI: body mass index; TAS: Tegner activity scale; SSD: side-to-side difference; FAMT: femoral anteromedial tunnel; FPLT: femoral posteromedial tunnel; TAMT: tibial anteromedial tunnel; TPLT: tibial posteromedial tunnel; SD: standard deviation.
a p < 0.05.
b p < 0.01.
Discussion
The most important finding of the present study was that although the clinical results of the four groups did not differ to a statistically significant extent, the presence of a Crain type 3 remnant was associated with a significantly lower preoperative SSD. In addition, the TBIS of the Crain type 4 patients was significantly longer in comparison to the other groups.
Crain et al. 4 reported that the pattern of scar formation after types 1, 2, 3, and 4 ACL rupture was 38%, 8%, 12%, and 42%, respectively. The TBIS of this study was 78 weeks. The incidence of Crain type 4 ruptures was greater than that observed in the present study (TBIS, 34.7 weeks). This may have been caused by the differentiation of the TBIS. The histology of ACL healing has been well documented. 13 Several studies have described the rapid degeneration and resorption of the ACL after acute rupture. 14 –17 Murray et al. 14 reported four distinct healing phases representing a relatively delayed and incomplete healing response spanning more than a year after injury. Thus, in the reports of Crain et al., 4 which included cases that had been treated over a 1-year period, the incidence of type 4 ruptures was high.
Crain et al. 4 reported that anterior laxity after debridement was observed in the patients with type 1 (mean, 1.3 mm), type 2 (mean, 3.4 mm), type 3 (mean, 4.3 mm), and type 4 (mean, 0.2 mm). Maeda et al. 3 reported that the preserved type 3 remnant could increase anterior knee stability. Nakase et al. 18 reported that the type 3 ACL remnants contributed to anteroposterior and rotatory knee laxity evaluated at 30° of knee flexion using the navigation system. The results of the present study also show that Crain type 3 remnant contributed to the most anteroposterior knee laxity. Nakase et al. hypothesized that compared with remnants at other insertion sites, the type 3 remnant, which is continuous near the ACL anatomical insertion on the femur, contributed significantly more to anterior and rotatory knee laxity. We also support their opinion.
The present study showed that the preoperative rotatory knee laxity of Crain type 4 was more lax than that observed in other groups. While it has been reported to not contribute to rotational stability, 2,3 in contrast, Nakase et al. did report that Crain type 3 remnant contributed to rotatory knee laxity. 18 However, these reports did not include Crain type 4. Because Crain type 4 did not show any continuity with the remnant, it was therefore thought that the remnants of Crain type 4 did not contribute to rotational stability.
Several reports have investigated the relationship between TBIS and the different remnant types. Nakase et al. 18 reported that the TBIS of patients with a type 4 remnant was longer than that in patients with other types. The present study shows that the TBIS in the patients with Crain type 4 was significantly longer in comparison to the other groups. Since the absorption of remnants occurred during the long waiting period, 14 it was suggested that the presence of some factor in types 1, 2, and 3 was changed in type 4. Since types 1, 2, and 3 TBIS was within 1 year after the injury, ACL reconstruction should be performed within 1 year after the injury to prevent resorption of the remnant.
Few reports have investigated the associations between postoperative results and the types of remnants. Kondo et al. 19 reported that remnant preservation in anatomic DB ACL reconstruction did not significantly improve the subjective or functional results in short-term evaluations, but that they significantly improved postoperative knee stability. The degree of initial graft coverage significantly affected the postoperative knee stability. The present study shows that the postoperative Lysholm scale and SSD values of the four groups did not differ to a statistically significant extent. Since we did not evaluate the initial graft coverage of the remnant, it is possible that the initial graft coverage influenced the postoperative results. The preservation of the synovium during reconstruction surgery in cases involving a Crain type 3 remnant was difficult because it was located close to the ACL femoral footprint and could easily have been damaged during the preparation of the femoral tunnel. 20 Although the patients with Crain type 3 remnants showed significantly decreased preoperative SSD values, this may be the reason why no significant difference was observed in the postoperative results.
The present study was associated with several limitations. First, with respect to the items for which no significant differences were detected, it is possible that the lack of statistical significance was due to the low statistical power of the present study. Second, the number of patients with each type of remnant was different. Third, the initial graft coverage of remnant was not evaluated and it is possible that this factor influenced the postoperative results.
To the best of the authors’ knowledge, the relationship between the remnant type and the clinical results of patients undergoing DB ACL reconstraction using hamstring tendon autografts has not previously been investigated. In addition, the present study had some notable strengths: the gender, type of graft, and surgical techniques that were performed were comparable among the four groups and the patients underwent the same rehabilitation program. Although the clinical results of the four groups did not differ to a statistically significant extent, the results of the present study suggest that a Crain type 3 remnant was significantly associated with a decreased preoperative SSD. In addition, the TBIS of the patients with Crain type 4 was significantly longer in comparison to the other groups.
Conclusion
The Crain type 3 ACL remnants were shown to contribute to preoperative anteroposterior knee laxity. Although there were no significant differences among the groups with regard to the clinical results, it is suggested that Crain type 3 remnant should be preserved during ACL reconstruction.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.