
Abstract
Purpose:
We aimed to evaluate (1) the intraoperative parameters, (2) cup position, (3) complications, (4) long-term results, and (5) the survivorship of cementless total hip arthroplastys (THAs) with use of ceramic bearings in patients with a history of acetabular fracture.
Methods:
We compared 57 THAs in patients, who were treated due to previous acetabular fracture (posttraumatic group), with 57 propensity score-matched THAs in patients, who were operated due to femoral head osteonecrosis (osteonecrotic group), at a minimum of 5-year follow-up.
Results:
The operation time was longer (p = 0.008), and the volume of transfusion was larger (p = 0.0.23) in the posttraumatic group. The cup abduction (39.4° ± 6.0° vs. 39.7°±4.8°) and anteversion (24.7° ± 8.0° vs. 26.7°±7.7°) were similar between the two groups. There was one dislocation in the posttraumatic group. There was no ceramic fracture in either group. One posttraumatic patient underwent excision of exuberant heterotrophic ossification at 3 years after the arthroplasty. The mean University of California, Los Angeles activity improved from 3.6 to 4.9 points in the posttraumatic group and 3.5 to 5.2 points in the osteonecrotic group. All acetabular cups and femoral stems had bone-ingrown stability. When reoperation for any reason was used as the end point, the 10-year survival rate was 98.3% (95% CI: 95.0–100) in the posttraumatic group and 100% in the osteonecrotic group.
Conclusion:
In our study, posttraumatic patients had longer operation time and larger volume of transfusion than osteonecrotic patients. However, medium-term results and survivorship were similar with those of osteonecrotic patients.
Introduction
Acetabular fractures occur primarily in young adults involved in high energy trauma. 1 Although modern operative techniques and fixation devices have been developed, 13–44% of the patients with previous acetabular fracture would have posttraumatic osteoarthritis of the hip and necessitate total hip arthroplasty (THA). 2 –4 THAs in these patients are challenging because of scarring from the previous injury and surgery, distorted anatomy of the pelvis, defective acetabulum, and complications involving previous hardware. 5 Due to these challenges, some retrospective reviews have reported poor results after THAs performed for posttraumatic osteoarthritis, 6 –8 and other studies have reported higher rate of complications and lower rate of survival than THAs performed for other indications. 4 In those studies, mainly conventional metal-on-polyethylene bearings were used. 4 Another risk factor of the failure is the young age of patient population. These young patients might require future revision because the longevity of THA falls short of their life expectancy. Recently, durable alternative bearings have been introduced. 9 Highly crosslinked polyethylene and hard-on-hard bearings have demonstrated extremely low rate of wear. However, no study has reported the results of THAs with use of the modern bearings in posttraumatic osteoarthritis of the hip.
The purpose of this study was to evaluate the operative parameters, complications, long-term results, and survivorship of cementless THA using ceramic bearing in patients with posttraumatic osteoarthritis, by comparing those of propensity score-matched patients with femoral head osteonecrosis.
Materials and methods
Patients
Between May 2003 and June 2012, 61 patients (61 hips) underwent cementless primary THA due to posttraumatic osteoarthritis after acetabular fractures at a tertiary referral institution. Ceramic-on-ceramic bearing was used in all of the 61 THAs. Two patients (two hips) died and two patients (two hips) were lost to follow-up before a minimum follow-up of 5 years. This left 57 THAs, which were subjects of this study.
There were 31 men (31 hips) and 26 women (26 hips) with a mean age of 31.9 years (range: 6–79 years) at the time of trauma and a mean age of 52.5 years (range: 19–83 years) at the time of index hip arthroplasty. The mean body mass index (BMI) was 25.3 kg/m2 (range: 18.7–34.6 kg/m2). Among the included 57 patients, 51 patients had been treated not in our hospital, but elsewhere. Twenty-six hips had been treated with internal fixation for the acetabular fracture and 31 hips had been treated conservatively. Mean interval between acetabular fracture and THA was 19.0 years (range: 2–720 months). The 57 patients were followed for a mean duration of 7.8 years (range: 56–162 months).
We used patients, who underwent THAs due to femoral head osteonecrosis (FHON), as a control group, because that disease has an adult onset and is not associated with a serious anatomical distortion of the acetabulum. Fifty-seven control THAs were abstracted from our database of primary THAs due to FHON by propensity score matching for gender, age, BMI, time of arthroplasty (1 year), and length of follow-up 10 (Table 1).
Demographics of patients.

THA: total hip arthroplasty; BMI: body mass index; UCLA: University of California, Los Angeles activity scales; ASA: American society of Anesthesiologists physical status classification.
Surgical techniques
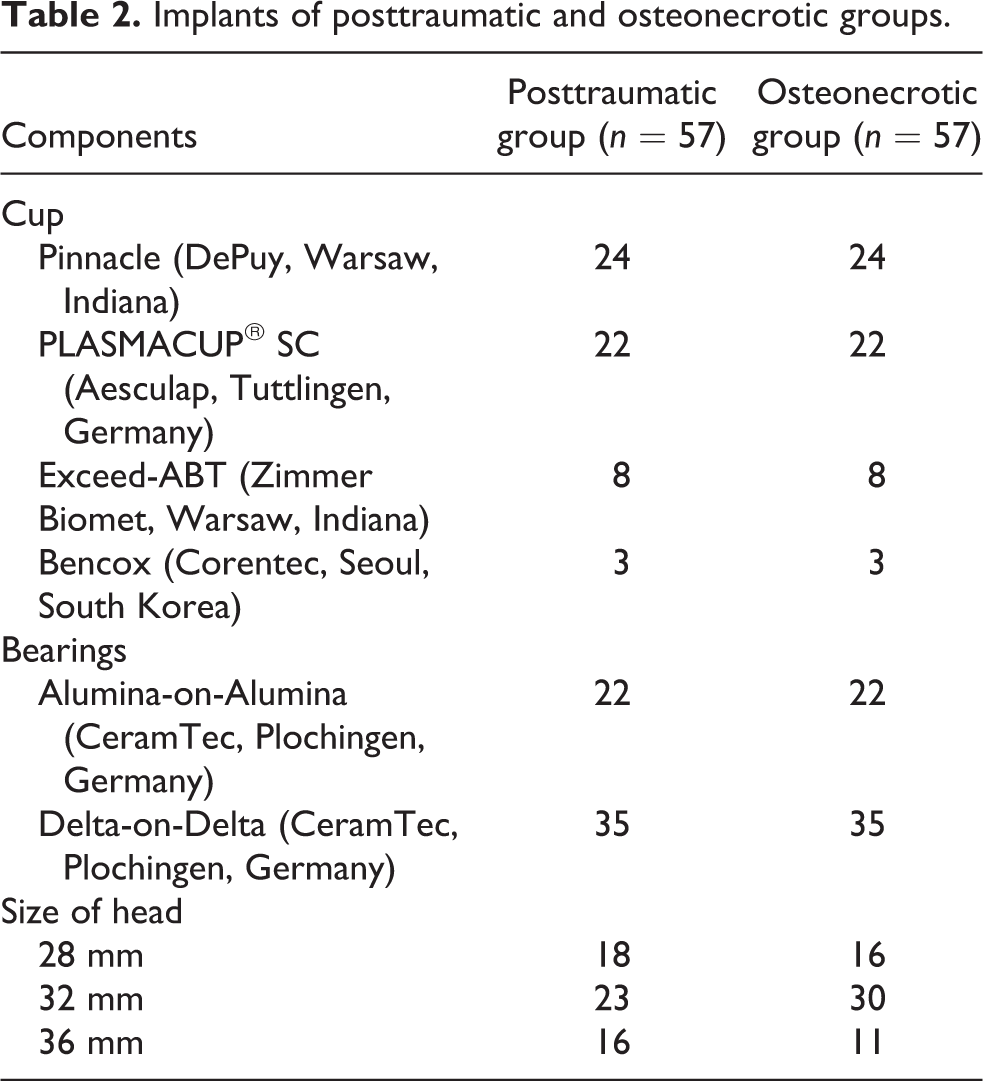
All operations were performed by four senior hip surgeons. In the posttraumatic group, posterolateral approach was used in 45 hips, anterolateral approach in 4 hips, combined approach in 7 hips, and tri-radiate approach in 1 hip. In the FHON group, posterolateral approach was used in 49 hips, anterolateral approach in 7 hips, and combined approach in 1 hip. Cementless prostheses and ceramic-on-ceramic bearings were utilized in all THAs (Table 2).
Implants of posttraumatic and osteonecrotic groups.
The target position of acetabular cup was 40–45° abduction and 20° anteversion. 11 In all patients, preoperative CT scan was performed for planning of THA. On the preoperative CT scan, we measured abduction and anteversion of the acetabulum to guide the cup positioning during the operation according to the method of Ha et al. 12 If the depth of the osseous cavity was not sufficient to cover the acetabular component with host bone after acetabular reaming, the medial acetabular wall was more reamed to the level of medial cortex to deepen the cavity using the Dorr’s technique, and the medial placement technique was used. 13,14
The acetabular and femoral components were inserted in a press-fit manner.
To prevent dislocation, the posterior capsule and short external rotators were tightly repaired to three drill holes in the trochanteric crest in cases of posterolateral approach. 15 In cases of anterolateral approach, abductor muscle was tightly repaired.
Patients were encouraged to walk with toe-touch weight bearing with the aid of two crutches for 4 weeks and then were allowed weight bearing as tolerated.
Evaluation
Routine follow-up visits were scheduled for 6 weeks, 3, 6, 9, and 12 months, and every 6 months thereafter.
We evaluated the operation time, perioperative blood loss, requirement of transfusion, hospital stay, cup position, periprosthetic joint infection (PJI), rate of dislocation, University of California, Los Angeles (UCLA) activity scales, 16 noise, ceramic wear, periprosthetic osteolysis, ceramic fracture, implant loosening, heterotopic ossification, and the survivorship of THA.
The noise was classified into snapping, clicking, popping, grinding sensation, and squeak. 17
Two independent observers, who did not participate in THA, evaluated radiographs. The 6-week anteroposterior and cross-table lateral radiographs were considered to be the baseline studies for radiographic comparison.
The abduction of the acetabular component was measured by the method of Engh et al. 18 The anteversion of the acetabular component was calculated by the method of Woo and Morrey. 19 The fixation of the acetabular component was classified according to the method by Latiner and Lachiewicz 20 and that of the femoral component according to the method of Engh et al. 21 Wears of the bearing surfaces were measured by the method by Livermore et al. 22 Osteolytic lesions were defined according the criteria of Engh et al. 23 Heterotopic ossification was classified according to the method of Brooker et al. 24
Statistical methods
We used Fisher’s exact test for categorical variables and the Mann–Whitney U-test for numerical variables to compare the results of both groups. A p-value of less than 0.05 was considered significant.
Kaplan–Meier Survivorship analysis was performed using three end points: revision of any implant, re-operation for any reason and any re-operation, and radiological evidence of osteolysis or loosening. We used SPSS version 16.0 (SPSS Inc., Chicago, Illinois, USA). The design and protocol of this study were approved by the institutional review board of our hospital, which waived informed consents of patients.
Results
Operative parameters
Operation time was longer (p = 0.008), and the amount of transfusion was larger (p = 0.023) in the posttraumatic group than in the osteonecrotic group (Table 3). No patients in either group had neurological complications, venous thromboembolism, or periprosthetic joint infection after the arthroplasty.
Comparisons between posttraumatic group and osteonecrotic group.
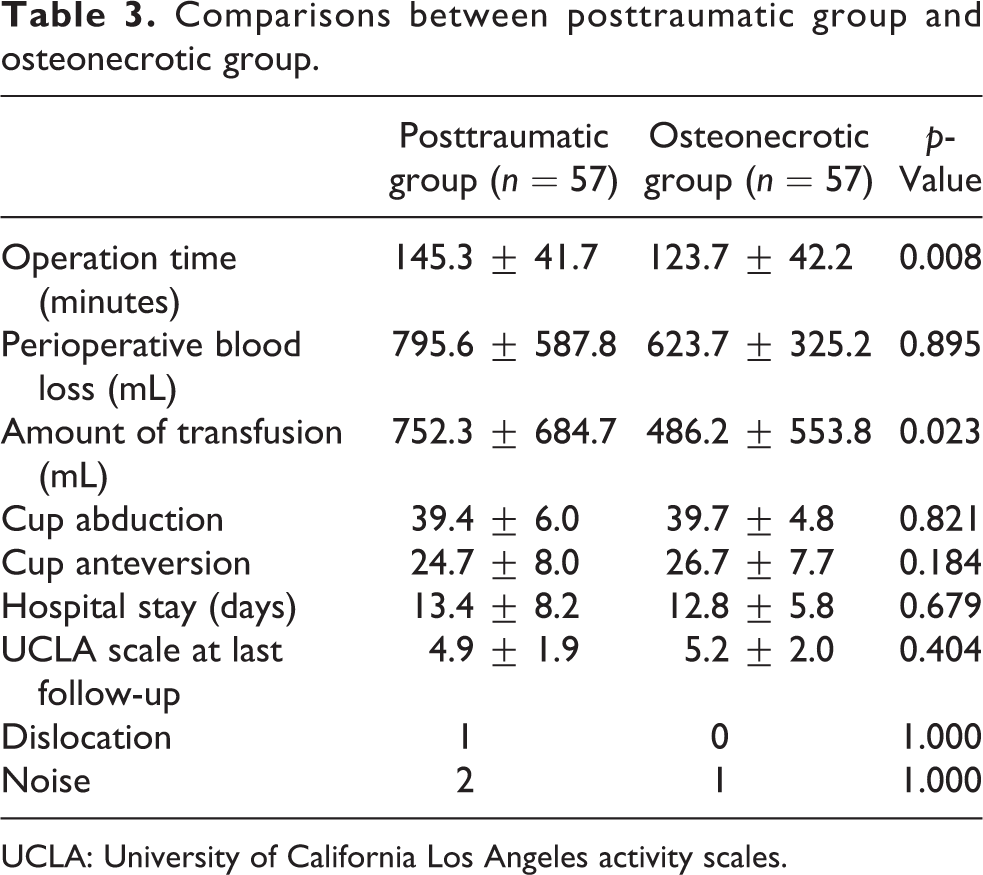
UCLA: University of California Los Angeles activity scales.
Cup position
The cup anteversion (39.4° ± 6.0° in the posttraumatic group and 39.7°±4.8° in the osteonecrotic group) and abduction (24.7° ± 8.0° in case group and 26.7°±7.7°) were similar between the two groups (p = 0.184 and 0.821) respectively) (Table 3).
Complications
There was one dislocation in the posttraumatic group. The dislocation occurred on 12 days after the arthroplasty due to a fall and was treated successfully with a closed reduction and an abduction brace for 3 months. There was no ceramic fracture during the follow-up.
Two patients (3.5%) in the posttraumatic group and one patient (1.8%) in the osteonecrotic group were experienced noise; grinding in one posttraumatic patient and one osteonecrotic patient, snapping in one posttraumatic patient. These noises were not associated with pain or functional limitation.
Clinical outcomes
At the time of the latest follow-up, the mean UCLA activity improved from 3.6 to 4.9 points in the posttraumatic group and 3.5 to 5.2 points in the osteonecrotic group.
Radiologic outcomes
All of the acetabular cups and femoral stems had radiographic evidence of bone ingrowth at the last follow-up. There was no detectable wear of ceramic bearings and no periprosthetic radiolucent line or osteolysis around any cup or stem (Figure 1).

A 54-year-old woman underwent THA because of posttraumatic arthritis on the right hip. (a) Preoperative radiograph. (b) Immediate postoperative radiograph. (c) 10 years follow-up radiograph, which shows bone-ingrown stability. THA: total hip arthroplasty.
Radio-reactive lines were observed in two posttraumatic hips, which were operated with Corail stems (DePuy, Warsaw, Indiana, USA) in zone 1, and in one osteonecrotic hip, which were operated with BiContact stem (Aesculap, Tuttlingen, Germany; zones 2, 3, 5, and 6). They were <2 mm and did not progress in any hip.
Grade IV heterotopic ossification developed in one posttraumatic patient. The ossification was excised at 36 months after the THA (Figure 2).

A 72-year-old man underwent THA because of posttraumatic arthritis on the left hip. (a) Preoperative radiograph. (b) Immediate postoperative radiograph. (c) 3-year follow-up radiograph, which shows grade IV heterotopic ossification. (d) Radiograph after excision of heterotopic ossification. THA: total hip arthroplasty.
Survivorship
No prosthetic revision was required during the follow-up period in either group. When revision of any implant was used as the end point, the survival rate was 100% at 10 years in both groups. When reoperation for any reason was used as the end point, the 10-year survival rate was 98.3% (95% CI: 95.0–100) in the posttraumatic group and 100% on the osteonecrotic group (Figure 3).
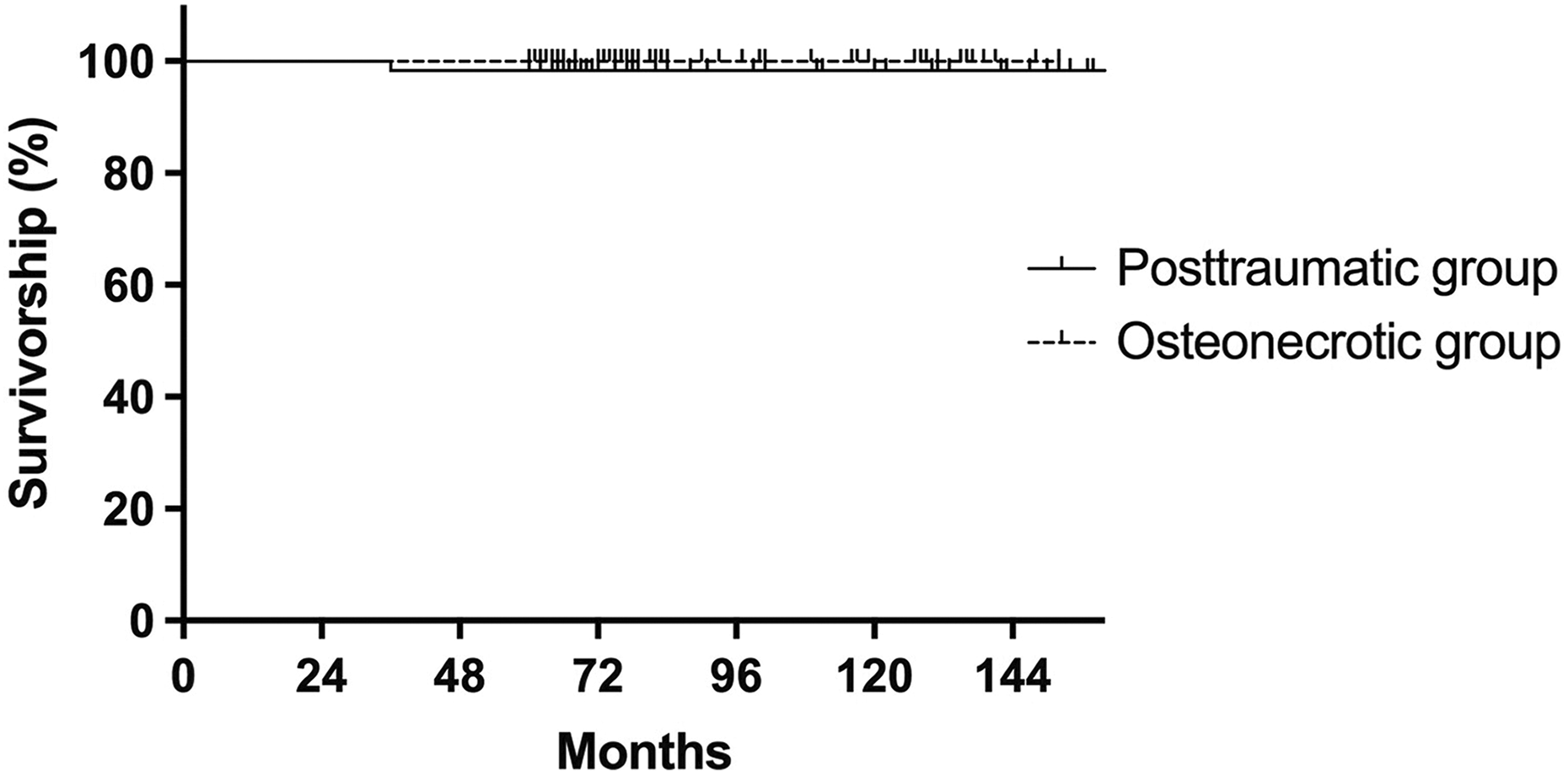
The Kaplan–Meier survival curve with any reoperation for any reason as the end point. Tick marks indicate censored data.
Discussion
THA of posttraumatic osteoarthritis of the hip is technically demanding and associated with high rate of failure. 6 –8 This is the first report on the cementless THA with the use of a ceramic-on-ceramic bearing in these cases. This study revealed satisfactory results and excellent survival at minimum 5 years follow-up without detectable wear, osteolysis, PJI or prosthetic loosening.
During conversion THA after acetabular fractures, surgeons face several challenging problems, including difficult surgical dissection due to posttraumatic/postoperative adhesion and scar tissue, anatomical alteration or defect of the acetabulum, and previous fixation devices. 25,26
Previous studies have reported conflicting results after THA in patients with traumatic osteoarthritis after acetabular fracture. 4,6 –8,27 Some studies reported comparable results of THAs for traumatic arthritis to those of THAs for nontraumatic arthritis. Bellabarba et al. reviewed 30 THAs, which were performed with use of a cementless acetabular component for the treatment of posttraumatic osteoarthritis after acetabular fracture. 27 The intermediate-term clinical results were similar to those after THA for nontraumatic arthritis. However, other studies reported inferior outcome compared to THAs due to nontraumatic osteoarthritis. 4,6 –8 Morison et al. 4 compared 74 THAs after acetabular fractures with the same number of THAs performed for other indications. The 10-year survivorship was lower in posttraumatic patients than in the matched cohort (70% vs. 90%). Posttraumatic patients had a higher rate PJI (7% vs. 0%), dislocation (11% vs. 3%), or heterotopic ossification (43% vs. 16%). Romness and Lewallen 28 retrospectively reviewed 55 THAs in 53 patients with a history of previous acetabular fracture. At a mean follow-up of 7.5 years, the incidence of radiographic acetabular loosening was 52.9%, and the rate of acetabular revision was 7.8%.
In most of prior studies, conventional metal-on-polyethylene bearings were used. Recently, some studies reported excellent outcomes of THA with use of modern bearings. Lai et al. performed THA with ultra-high-molecular weight polyethylene articulation in 31 patients with traumatic arthritis. 29 The survivorship was 100% at the mean of 6.3-year follow-up. 29
Our study has several limitations. First, it was a retrospective review of a single cohort. Second, all THAs were done by four high-volume hip surgeons in a tertiary referral institution. The results might be otherwise, if THAs were done other surgeons. Third, we exclusively used ceramic-on-ceramic bearing and we could not compare our results with those of other bearings. Fourth, the severity and type of previous acetabular fractures, which might have influenced the postoperative results, were not included in our analysis. We could not evaluate the effects of previous fracture configuration, because majority of patients (89.5%, 51/57) had been treated for the fracture elsewhere, and their initial radiographs were not available.
In the literature, THAs due to posttraumatic arthritis have been known to be associated with worse outcome than other types of osteoarthritis. Two main reasons for the worse outcome were as follows: (1) insufficient coverage of metal shell due to defective acetabulum and (2) difficult cup positioning due to posttraumatic deformity of the acetabulum. 5,6,8
However, we used medialization technique to obtain sufficient acetabular coverage in patients with deficient acetabulum, 13,14 and we performed preoperative CT scan for accurate positioning of acetabular cup. 12 In our study, the results of THA due to posttraumatic arthritis were comparable with those due to osteonecrosis.
Conclusion
The results of cementless THA with use of a ceramic bearing were satisfactory and the survivorship was excellent in patients with posttraumatic arthritis of the hip at a mean follow-up of 7.8 years.
Footnotes
Author contribution
Young-Kyun Lee and Ki-Choul Kim equally contributed this work and should be considered as co-first authors.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.