
Abstract
Background:
This study aimed to explore a new surgical technique for gap balance by tightening the medial collateral ligament (MCL) in total knee arthroplasty (TKA) in patients with fixed valgus deformity.
Materials and Methods:
A prospective analysis was performed on 15 patients (16 knees) with a fixed valgus deformity that was corrected by tightening the MCL during TKA. A single surgeon performed all the 16 TKAs using nonconstrained posterior substituting implant, with two knees treated with long-stem tibial prosthesis. Clinical scores, knee stability, and radiographic evaluations were recorded preoperatively and postoperatively.
Results:
Complete weight-bearing could be carried out under the protection of the brace postoperatively. At the third month after surgery, X-rays showed the brace was not worn. The mean follow-up was 26.6 months (range 12–42 months). The average preoperative mechanical axis was 15.4 ± 2.3° (range 11–25°), and postoperatively it was 0.6 ± 0.1° (range 0–2°). No complication relative to the technique occurred.
Conclusion:
This new surgical technique has demonstrated excellent early clinical results and can be a good supplement for fixed valgus knee arthroplasty.
Introduction
Valgus deformity is found in 10–15% of the patients who undergo primary total knee arthroplasty (TKA). Valgus knees have a variety of complications, such as instability, recurrent valgus deformity, wound problems, patellar osteonecrosis, patellar maltracking, and peroneal nerve palsy. 1 –3 One specific problem presented by fixed valgus deformities is lateral contracture, which means the lateral soft tissues, including the lateral collateral ligament (LCL), popliteus tendon (POP), posterolateral capsule (PLC), iliotibial band (ITB), and posterior capsule, can become contracted. Therefore, releasing the lateral structure is necessary for the fixed valgus deformity. Since the medial collateral ligament (MCL) is often attenuated or incompetent on the medial side, restoring the tension of the MCL is also important. 4
When restrictive prostheses are used in TKA, only the lateral structures need to be released and there is no need to consider the laxity of the medial ligament. 5 –7 However, when nonrestrictive prostheses are used, after releasing the lateral structures, the MCL needs to be advanced. Several techniques are used to tighten the MCL, 3,8 –12 such as cutting the MCL at midsubstance and imbrication, moving the tibial attachment of the MCL to the distal tibia, and removing the femoral attachment of the MCL to the proximal femur. There are three methods to perform the last one: sliding the osteotomy of the medial epicondyle and fixing with screws 9 ; recessing the MCL with a bone block from the femoral epicondyle and replanting overhead 10 ; removing the MCL from the epicondyle and resetting with a surgical staple. 11 These procedures either destroy the ligament integrity or need internal fixation, which may cause ligament failure.
Here we introduce a novel technique to tighten the MCL, which has demonstrated excellent early clinical results.
Materials and methods
The study was approved by the clinical ethics committee of our hospital, and all participants signed informed consent. From November 2014 to February 2017, 15 patients were enrolled according to the following criteria: fixed valgus knee, intact mediolateral collateral ligament, having received this new surgical approach. Exclusion criteria included Charcot joint, rickets, knee valgus caused by fractures, ligament damage. A prospective analysis was conducted on the enrolled patients. All the 15 patients (1 male and 14 females, 16 knees) with fixed valgus deformity underwent knee arthroplasty by a single surgeon. After lateral contracture release, the gap balance in extension was not achieved in their knees, then they were addressed with the MCL tightening technique.
Valgus angle, laxity of MCL, and stability of the knee joint were examined. Full-length weight-bearing radiography was obtained at each follow-up. The clinical outcomes were measured by the Hospital for Special Surgery (HSS) Score, visual analog score (VAS) score, Knee Society Knee Score, and Knee Society Functional Score, both preoperatively and postoperatively. All 16 knees were treated with a condylar nonconstrained posterior substituting implant (Legion, Smith & Nephew, Memphis, Tennessee, USA); two knees had long tibial stems to enhance the stability of the tibial plateau prosthesis (Legion, Smith & Nephew, Memphis, Tennessee, USA). The follow-ups were performed at 1, 2, 3, 6, and 12 months and then annually.
Surgical technique
Preoperative osteotomy planning was previewed on full-length weight-bearing radiographs. Constrained implants, long stems, and augmented prostheses were prepared according to the lateral bony deficiency of the tibia and femur. The medial parapatellar approach was used in all patients. Osteophytes around the patellar surface were removed and lateral retinacular release was performed when necessary to evert the patella.
The tibial cut was orthogonal to the tibial mechanical axis on the coronal plane with no slope on the sagittal plane. Augmentation of the lateral tibial components was applied in cases with severe lateral defects. Osteotomy of the distal femur was performed according to the preoperative planning. The archer point of the intramedullary rod was deviated toward the lateral condyle.
The posterior capsule and PLC complex were transected along the proximal tibial border, and the ITB was released using the “pie-crusting” technique by creating multiple small cuts in the ITB to elongate it while maintaining its continuity. An extensive spacer was used to test ligament balance in the extended state. A rectangular gap was achieved in most patients with fixed valgus knee without the release of LCL and POP.
If a sufficiently stable extension gap was not achieved by releasing the lateral structures, the MCL was advanced. Firstly, the medial plateau was split longitudinally 10–15 mm from the medial edge with a saw and expanded into a crack with an osteotome, with the continuity of the distal cortical bone carefully maintained (Figure 1(b)). Secondly, cancellous bone was packed into the crack with the grafting device, and the ligamentous balance was tested again. In case of slightly loose MCL, bone grafting was performed gradually to gain soft tissue balance in extension. Thirdly, the anteroposterior (AP) and the transepicondylar axes were used as references for the correct femoral rotation to ensure that the posterior condylar resection was parallel to the tibial cut and perpendicular to the tibial mechanical axis (Figure 2).

(a) After lateral release, a spacer block was used to check the extension gap. (b) Sagittal splitting on the medial plateau was approximately 15 mm from the medial edge of the tibial plateau. The cancellous bone was compressed into the crack resected from another place and the MCL was tightened by squeezing and broadening the medial plateau. (c) Bone cement covered the graft and medial bone block, and the MCL was tightened. MCL: medial collateral ligament.

The AP and the transepicondylar axes were used as references to achieve the correct femoral rotation. AP: anteroposterior.
After lateral release, with lateral stability and an optimal insert, the MCL laxity of greater than 10 mm in extension was considered as dysfunctional. Therefore, a constrained implant or sliding osteotomy of medial femoral condylar was needed. The widening width was kept within 20 mm to prevent the instability of the tibial prosthesis. The medial soft tissue was dissected as little as possible to ensure the integrity of the medial periosteum, because it was considered as the key to bone healing (Figure 3).

(a) The patient, a 65-year-old woman, had a rigid valgus knee. The mechanical axis was 14° and many osteophytes were present around with contracted LCL. (b) After lateral release, the residual laxity of MCL was 4 mm and the widening length of the medial plateau was 12 mm, which perfectly balanced the ligament. Union occurred in 3 months. (c) The yellow area was bone graft and the continuity of the distal cortex was maintained. LCL: lateral collateral ligament; MCL: medial collateral ligament.
For the elderly patients with severe osteoporosis, this technique might result in medial bone collapse due to the insufficient holding power at the medial tibial plateau. This problem was solved with a long-stem tibial prosthesis (Figure 4).

In a 79-year-old woman, the long stem of the tibial prosthesis was used to provide sufficient support for the medial tibial plateau.
X-ray examination was performed at each follow-up to detect the collapsed medial plateau, the displaced fractured fragments, and the absorption of the filled bone graft area. Bone healing was defined as no significant change for three consecutive months.
Results
All the 16 knees treated with this MCL advancement procedure had satisfactory outcomes. The patients obtained satisfactory initial stability and flexion. They were able to perform extension exercises and full weight-bearing under the protection of the brace after operation. Complete weight-bearing without brace was allowed when X-rays show fracture healing at the third month postoperatively. Patients with long stem on the tibial side were allowed full weight-bearing walking without brace.
The patients’ feedback included pain relief, restoration of the affected limb to normal shape, and improved knee function. After lateral release, the average medial laxity of MCL was 3.6 ± 0.5 mm, and mean broadened width of the medial plateau was 10.2 ± 1.7 mm. The mean mechanic alignment was improved from valgus 15.4 ± 2.3° (range 11–25°) to 0.6 ± 0.1° (range 0–2°) (Table 1).
Patient data.

MCL: medial collateral ligament; BMI: body mass index; SD: standard deviation.
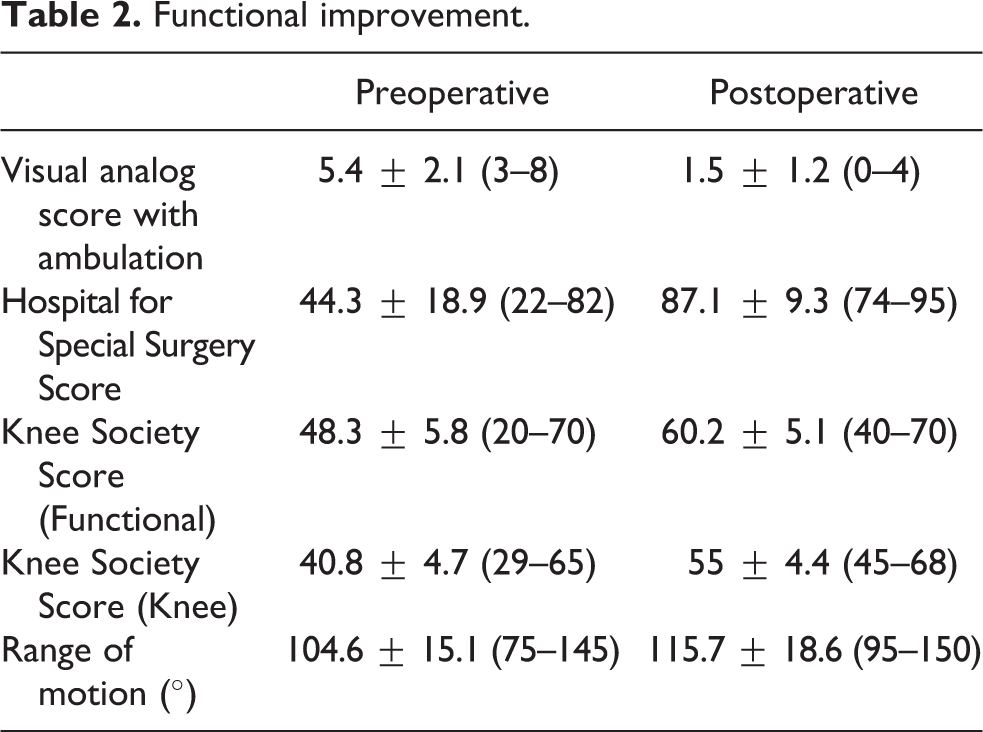
The average VAS decreased from 5.4 ± 2.1 (range 3–8) preoperatively to 1.5 ± 1.2 (range 0–4) postoperatively. In physical examination, no patient had medial or lateral laxity after the ligament advancement procedure. The average range of motion increased from a preoperative arc of motion of 104.6 ± 15.1° (range 75–145°) to 115.7 ± 18.6° (range 95–150°) postoperatively. The average Knee Society Knee Score improved from 40.8 ± 4.7 (range 29–65) preoperatively to 55 ± 4.4 (range 45–68) postoperatively. The average Knee Society Functional Score improved from 48.3 ± 5.8 (range 20–70) preoperatively to 60.2 ± 5.1 (range 40–70) postoperatively. The average HSS increased from 44.3 ± 18.9 (range 22–82) preoperatively to 87.1 ± 9.3 (range 74–95) postoperatively (Table 2).
Functional improvement.
Patients were followed up for 12–42 (mean 26.6) months. All knees had good patellar positions and were clinically stable in both the mediolateral and AP planes. No radiolucency was noted. There were no incidents of pulmonary embolism, peroneal nerve palsy, wound problems, patellar maltracking, or medial collapse at the latest follow-up.
Discussion
There are several strategies to achieve soft tissue balance with fixed valgus knees in TKAs. Restrictive prosthesis or semi-restrictive prosthesis, combined with complete release of lateral soft tissue, is commonly used. Xie and Lyons 5 followed up 214 patients with valgus knees for TKAs, and found that 38% of them needed three releases and 14% needed four or more releases. It is generally believed that the more loosening of lateral structures, the more restrictive prostheses are needed. Nevertheless, good stability cannot be achieved without the laxity of MCL. 13 However, extensive loosening of the lateral structure can destroy the rotational stability of knee joint under knee flexion, concentrate the stress of polyethylene liner and increase the wear. At the same time, the radiolucent lines may appear earlier on the tibial plateau, which are visible in 70% of the patients. 14,15 Many documents consider LCL and POP as important structures for the lateral and femoral rotational stability, so they should not be injured during operation. 16,17 In our trial, a nonrestrictive prosthesis was used, without the release of LCL and POP, so theoretically, a better long-term clinical effect can be achieved.
Sliding osteotomy of the femoral condyle is also a classic procedure for addressing the valgus deformity of knee undergoing TKAs. Sliding osteotomy can be performed laterally to the distal end of the femoral condyle to match the relaxed MCL, and the osteotomy block can be fixed with screws. 18,19 Conjeski and Scuderi modified the technique by releasing the lateral supporting structures with a shingle of bone from the lateral femoral epicondyle to correct the fixed valgus deformity, including attachment points of both LCL and POP. 20 However, lateral sliding osteotomy enlarges the joint space and requires a thicker insert, which may lead to joint instability and peroneal nerve paralysis. 1 –3,20 Zhong et al. 12 and Mou et al. 9 described an upward sliding osteotomy of the medial condyle of the femur, followed by screw fixation, with satisfactory clinical results. Mou et al. 9 followed up 28 patients who underwent TKAs with their LCL and POP preserved during lateral soft tissue release for an average of 54 months. However, the MCL was so strong that nearly half of the cases followed up had malunions, even with screw fixation. 21 In our study, despite the increased track of the MCL, the intact MCL, the integral distal periosteum of the osteotomy, together with the fact that no screw fixation was used, all demonstrate a stronger healing ability.
In our study, we split the medial tibial plateau, compacted the graft, widened the medial tibial plateau, and tightened the MCL. This technique did not require any auxiliary tools or extra implants, which eliminates the problem of hardware fixation in a relatively osteopenic medial femoral condyle. The application of the technique prolonged the knee replacement operation for 10–15 min. During the surgery, special attention was paid to protect the integrity of the bone cortex and periosteum at the longitudinal division because both were crucial for bone healing. At 3 months after the operation, all the knees healed at the longitudinal osteotomy. After lateral release, all the 16 knees showed medial laxity of MCL with a mean laxity of 3.6 ± 0.5 (range 2–6) mm. The mean broadened width of the medial plateau was 10.2 ± 1.7 (range 7–14) mm, almost three times the length of the MCL laxity. If the residual laxity in the operation is greater than 10 mm, a restrictive prosthesis was recommended.
In this study, the two most concerned problems were the nonunion of the osteotomy and the collapse of the medial platform. Fortunately, the medial tibial plateau fracture was firmly fixed in situ by bone cement. All patients obtained satisfactory initial stability, and they could perform flexion and extension exercises after operation. Complete weight-bearing could be carried out under the protection of the brace. And at the third month after surgery, X-rays on fracture healing showed that the brace was no longer worn. In patients with long stem on the tibial side, the medial tibial plateau was sufficiently supportive and stable for full weight-bearing walking without the brace. All the patients were able to walk freely and no complications, such as medial collapse, joint instability, prosthesis loosening, and incision problems, were found at the last follow-up.
This technique allows early ambulation without any other internal fixation. It has demonstrated satisfactory clinical results in patients and could be a good supplement for fixed knee arthroplasty. However, the follow-up time of this study is short, and no comparative study with other surgical methods has been carried out. Therefore, further studies with large sample sizes and longer follow-up are required to corroborate our results.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the National Natural Science Foundation of China (grant no. 81171720).