
Abstract
Purpose:
Knee arthropathy is a frequent complication affecting hemophilic patients, which can cause severe pain and disability. When conservative measures fail, total knee arthroplasty (TKA) may be performed.
Methods:
Eighteen TKA were performed in 15 patients with hemophilia during a 24-year period in a Hemophilia Comprehensive Care Center. All patients were evaluated by a multidisciplinary team constituted by a hematologist, an orthopedic surgeon, and a physical medicine and rehabilitation physician. Mean follow-up was 11.3 years.
Results:
Ten-year survival rate with prosthesis removal as end point was 94.3%. At last, follow-up visual analog pain scale score was 3.2 points, knee osteoarthritis outcome scale was 86.7 points, and mean range of motion was 88°. Only two patients required perioperative transfusion. Complication rate was 27.8% and included two infections, two prosthesis stiffness, and one case of recurrent hemarthrosis.
Conclusion:
After appropriate medical optimization and with prompt rehabilitation, TKA can be performed in hemophilic patients with good clinical results and survivor rates comparable to nonhemophilic patients.
Introduction
Hemophilia A and B are X-linked inherited bleeding disorders, in which there is deficiency of coagulation factors, factor VIII (FVII) or factor IX (FIX), causing excessive bleeding. 1 In severe hemophilia (≤1% of normal activity of FVII or FIX), joint bleeding episodes may occur as frequently as 20–30 times per year. 1,2
Hemophilic arthropathy is the result of repeated intra-articular bleedings, with recurrent inflammation and subsequent articular destruction. 3 Any joint can be involved in this pathology, but the most affected are the knee (Figure 1), elbow, and ankle. The inflammatory response resulting from intra-articular bleeding affects patients’ quality of life (QOL) by causing acute and chronic debilitating pain as well as loss of function. 4,5

Photograph of the knee of a 25-year-old patient with hemophilic arthropathy. Note the marked swelling of the joint.
Current management of these patients is based on prophylaxis of the hemorrhagic episodes, by periodically administering the coagulation factor in deficit, in patients with severe disease. Chemical and radiosynoviorthesis are options in chronic synovitis in order to delay and avoid progression to arthropathy. 6 In cases of severe hemophilic arthropathy, surgical treatment should be considered. 6
Total knee arthroplasty (TKA) is an effective treatment to relieve pain and improve function in patients with advanced hemophilic knee arthropathy. 7 Most literature on TKA in hemophilic patients, however, reports small series of cases, with modest results and significant complications, such as quadriceps contracture, loosening, infection, and deformity. 1,3,8
The objective of this study was to assess and report the mid- and long-term results of TKA in the treatment of knee hemophilic arthropathy in a Hemophilia Comprehensive Care Center. Our hypothesis was that, through a multidisciplinary approach, with appropriate pre and postoperative management of bleeding, good clinical results and lower complication rates could be obtained.
Patients and methods
Patients
Fifteen patients (18 knees) with hemophilia who underwent TKA between 1990 and April 2013 in the same institution were reviewed. Ethical approval for data collection and analysis was obtained from the local ethics committee. Patient demographics (age, comorbidities as HIV, HCV, or HBV) and type and severity of hemophilia were obtained. All patients were evaluated in a multidisciplinary appointment by a hematologist, an orthopedic surgeon, and a physical medicine and rehabilitation physician.
Hematological management
Preoperatively, routine hematological and biochemical analysis were performed. All patients undertook laboratory testing for inhibitors for FVII and FIX inhibitors.
The perioperative factor substitution regimen was prescribed by a hematologist. FVII and FIX were administered by bolus to raise FVII and FIX to appropriate levels prior to surgery. Initial FVII dosage was 40–50 IU/kg and initial FIX dosage was 60–80 IU/kg. The targeted peak FVII levels were 80–100% and FIX levels were 60–80% preoperatively with the goal of maintaining trough levels of 40–50% for the first 3 postoperative days. Factors VIII and IX trough levels were regularly monitored and replaced if needed.
All patients received mechanical thromboprophylaxis with the wearing of compression stockings, and no pharmacologic antithrombotic prophylaxis was used throughout the study period.
Surgical procedure
Surgery was performed in a bloodless field with the use of a tourniquet, and a standard midline incision and a medial parapatellar approach were used. All surgeries were performed by same surgeon. Prosthesis components were cemented with antibiotic-loaded bone cement. Different types of prosthesis (12 cruciate sacrificing and 6 semi-constrained) were used in order to address different joint states and degree of instability.
Patients received prophylactic antibiotics preoperatively and for the first 24 h after surgery (third generation cefalosporin or clindamycin). Drains were removed 48 to 72 h after surgery.
Patients started active exercises on the second postoperative day, which was maintained for the first 8 postoperative weeks or longer. Patients were allowed partial weight bearing with crutches for 6 weeks, after which they started full weight bearing.
Outcomes measured
Demographic data, presence of associated comorbidities, hemophilia type, and presence of inhibitors were collected in all patients.
The following clinical data were analyzed: range of motion (ROM), visual analog pain scale (VAS), and knee osteoarthritis outcome scale (KOOS) (which measures pain, other symptoms, function in daily living (ADL), function in sport and recreation (Sport/Rec), and knee-related QOL). KOOS consists of five subscales, ranging from 0 to 100 (100 indicating no symptoms and 0 indicating extreme symptoms). 9 To ascertain patient satisfaction, they were asked if they would accept to undergo the same procedure.
Complications associated with the surgery such as blood loss, need for blood transfusion, infection, and revision surgery were also recorded. Periprosthetic infection was classified as early or late with symptoms presenting less or more than 4 weeks after arthroplasty, respectively, according to the classification by Segawa and Tsukayama. 10
Statistical analysis
Descriptive statistics were computed with SPSS for Windows, version 20.0. Kaplan–Meier survivorship analysis was performed to determine prosthetic survival rates. Means were calculated for normally distributed data. p < 0.05 was considered to represent a significant difference between means. Prosthetic failure was defined as removal for any reason.
Results
Fifteen patients were included in the study, all men, with a mean age of 39 years. One patient had hemophilia type B and all others had hemophilia type A. All but two patients were seropositive for hepatitis C, seven were seropositive for HIV, and one patient had chronic kidney disease under hemodialysis. The mean follow-up was 11.3 years. (Table 1). Two patients died during follow-up, due to nonorthopedic complications. Follow-up data and clinical scores from these two patients report to their last clinical evaluation.
Patient demographics.

Functional outcomes
All patients started physiotherapy during hospital stay. Mean ROM at last follow-up was 88°. Mean VAS at last follow-up was 3.2 points. Mean KOOS at last follow-up was 86.7 points (Table 2).
Clinical scores.

KOOS: knee osteoarthritis outcome scale; QOL: quality of life.
All patients were very satisfied with the results and would undergo the same surgery if needed.
Bleeding
Hemoglobin levels significantly decreased from preoperative (14.3 g/dL (range 9.4–17.2)) to day 2 after surgery (10.2 g/dL (range 7.4–12.5)) (p < 0.001). Two patients (11.1%) needed blood transfusion during hospital stay. No fatal bleedings were observed.
Complications
No neurovascular complications were registered. There were five complications (27.8%). One case of recurrent hemarthrosis (5.6%), which did not resolve with coagulation factor administration, was drained surgically, 2 weeks after index surgery. Two cases of joint stiffness (11.1%), which were successfully manipulated under general anesthesia at 4 and 5 weeks after index surgery. One case of early (2 weeks) prosthetic infection (5.6%) occurred and was treated with surgical debridement, polyethylene substitution, and appropriate antibiotics. In one case of late prosthetic infection (5.6%), which did not resolve with repeated surgical debridements, the prosthesis was removed and an arthrodesis was later performed. Both infections occurred in immunosuppressed patients.
Prosthesis survival rate was 94.4%% at 11.3 years (Figure 2). Figure 3 depicts illustrative X-rays of one case.
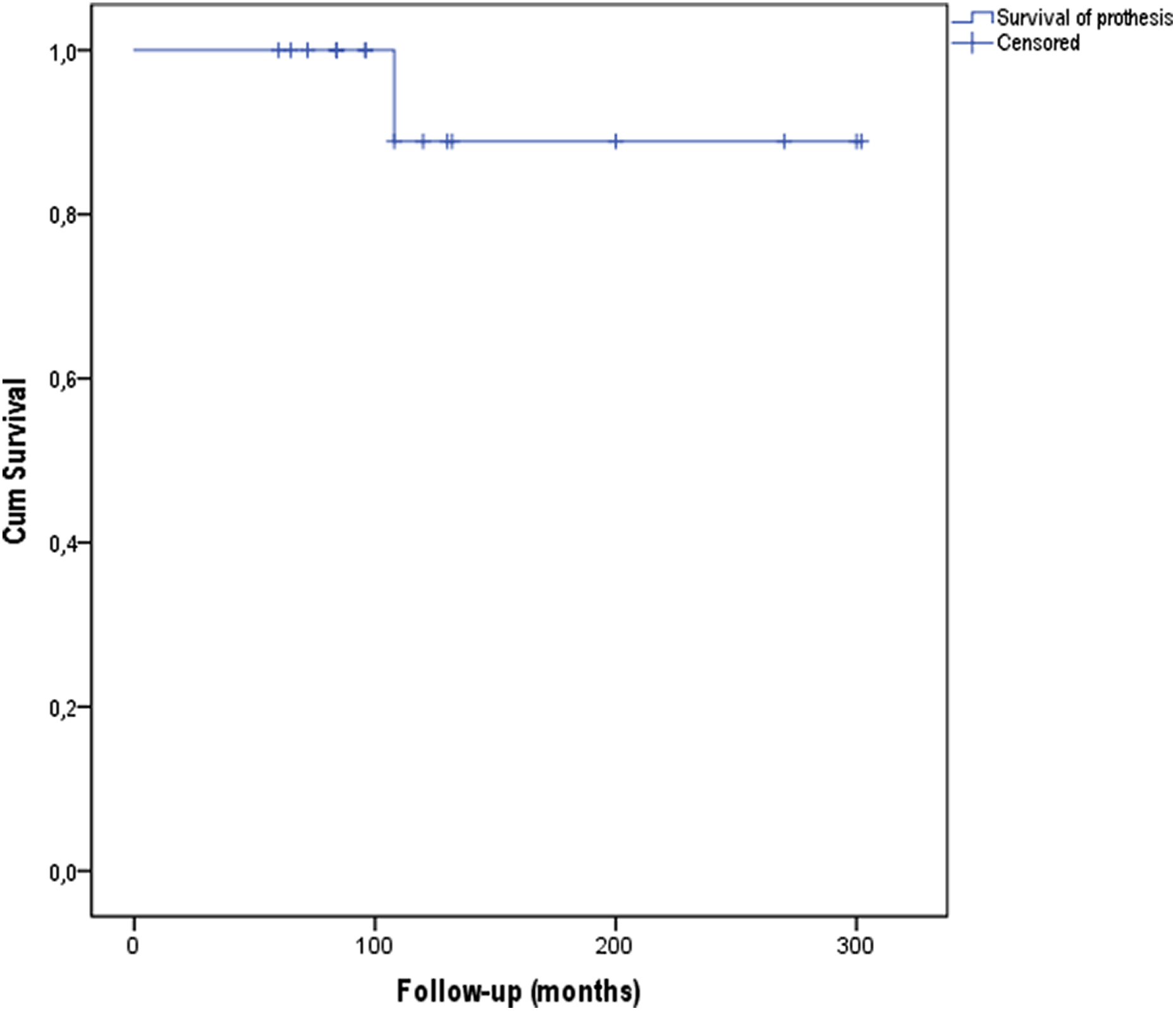
Kaplan–Meyer survival analysis. Cumulative survival of TKA in hemophilic patients with prosthesis removal as end point. TKA: total knee arthroplasty.

X-rays of a 63-year-old patient with hemophilic arthropathy submitted to a semi-constrained knee replacement. (a) preoperative AP view, (b) preoperative lateral view, (c) preoperative axial view, (d) AP view 8 years after surgery, (e) lateral view 8 years after surgery.
Discussion
While TKA is an effective treatment for primary arthritis and hemophilic arthropathy of the knee, the pathophysiology of both conditions is substantially different. In hemophilic arthropathy, repeated intra-articular bleeding occurs, with subsequent intra-articular deposit of hemosiderin and iron, which lead to upregulation of pro-inflammatory cytokines and, consequently, synovial hypertrophy and articular cartilage destruction. 8 The main objective in total joint replacement surgery is to reduce the level of pain in the affected joint. In patients with bleeding disorders, however, the results of TKA are expected to be inferior to those in patients without bleeding disorders. 11
The best predictor of postoperative ROM is the preoperatory ROM. When compared with nonhemophilic patients with knee arthritis, patients with hemophilic arthropathy of the knee tend to have lower preoperative ROM. That is explained by the marked muscular atrophy and fibrosis, accompanied by knee flexus that are often found in these patients due to numerous intra-articular hemorrhages. In a retrospective analysis of 70 TKA performed in hemophilic patients at 9.2 years, Goddard and colleagues report a mean ROM of 79°, 1 the same mean ROM reported by Westberg and colleagues in a retrospective analysis of 107 arthroplasties performed for hemophilic arthropathy at 11.2 years. 3 In this study, ROM at last follow-up was relatively higher—88° (70°–120°). While, as aforementioned, this is mainly related to the preoperative ROM, which due to the retrospective nature of the present study could not be evaluated, it is possible that this higher than previously reported ROM is due to the early initiation of rehabilitation together with an appropriate preoperative bleeding control.
The average KOOS score at last follow-up was 86.7 points, with the subscale with the lowest values being that evaluating function in sport and recreation. Nonetheless, all patients reported a significant pain relief and improvement in QOL and daily life activities. According to Wang and colleagues, patient satisfaction with pain relief is higher than satisfaction with functional improvement. 12 Significantly, all patients available for follow-up said they were extremely satisfied and would be willing to undergo the same surgery again.
In this study, prosthesis survival rate at 11.3 years was 94%, results higher than those found in other studies and identical to TKA in patients without hemorrhagic disorders. In hemophilic patients at an average follow-up of 10 years, Westberg and colleagues report a survival rate of 88%, 3 Silva and colleagues of 83%, 5 Wang and colleagues of 83%, 12 and Zingg and colleagues of 86%. 13 The mean age at the time of surgery was 39 years in this study. TKA in young patients without bleeding disorders has been associated with shorter implant survival time compared to elderly patients. 14 Diduch and colleagues 15 report a survival rate of 87% at 18 years with component removal for any cause as end point in 108 TKAs performed in patients under the age of 55. Lonner and colleagues report a 90% survival after 8 years in 32 TKAs in patients under the age of 40 16 while Duffy and colleagues report a survival rate of 85% at 15 years in 74 TKAs in patients under the age of 55. 17
The rate of periprosthetic infection after primary TKA in nonhemophilic patients is reported to be approximately 1%. 18 In patients with bleeding disorders, however, these rates are considerably higher: 13–16% in some earlier studies 5,19 and relatively lower in the more recent literature. 3,20 –23 Similarly, in this study, there were two cases of infection (11.1%). This high infection rate relative to primary knee replacement may be due to multiple reasons, such as HIV and HCV coinfections, as previously reported. 21 Additionally, and further contributing to the high periprosthetic infection rate in these patients, may be the regular administration of intravenous injections of coagulation factor. An aseptic technique for administration of coagulation factor concentrate is of highest importance in hemophilic patients, particularly those with an arthroplasty, and has been thoroughly discussed in the literature. 14,16,18,24,25
Another frequent complication in these patients is increased blood loss. In this study, there was a significant blood loss with a drop of 4.1 g/dl from preoperative values. However, and due to the preoperative optimization of these patients, which had an average preoperative value of 14.3 g/dL and also due to careful hemostasis during surgery, only two patients required blood transfusion after surgery. Furthermore, the amount of blood loss is comparable to that described by Solimeno (5.8 g/dl) 23 and Westberg (4.3 g/dL) 3 in hemophilic patients but also in nonhemophilic patients. 26,27
This study has several limitations. It is retrospective and lacks preoperative clinical scores. Additionally, the patient number is relatively small. However, the follow-up is one of the longest reported in the literature and adds to the available knowledge of the results of this procedure in hemophilic patients.
The institution in which this work was undertaken is a Hemophilia Comprehensive Care Center. They are evaluated by a multidisciplinary team consisting of a hematologist, an orthopedic surgeon, and a physical medicine and rehabilitation physician. This is important since pre and postoperative hematological optimization and postoperative rehabilitation of these patients are crucial for their adequate treatment and optimal outcome. Despite the challenge that constitutes performing TKA in this subpopulation of patients, results from this study are encouraging. Nonetheless, hemophilic patients and their attending physicians should be aware to the increased risks of performing an arthroplasty and to the inferior clinical results when compared to nonhemophilic patients.
Footnotes
Author contributions
Marta Santos Silva and Ricardo Rodrigues-Pinto contributed equally to this work
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.