
Abstract
Purpose:
In this study, we asked the question of whether non-invasive (NI) extendible bone tumour implants are as reliable and reduce infection when compared with patients who received a minimally invasive (MI) extendible implant.
Methods:
Forty-two NI extendible bone tumour implants were investigated at a mean follow-up of 22 months (range, 1–87 months) and 63 MI implants at a mean follow-up of 49 months (range, 1–156 months).
Results:
Kaplan–Meier analysis showed that the probability of MI implant survival was 58.8% compared with 78.6% in NI patients. No significant difference between these two patient groups was found. Infection was the main reason for failure in the MI implant group where nine (35%) implants were revised. However, only one (11%) NI implant was revised for infection (p = 0.042). None of the NI implants failed due to aseptic loosening; however, six (23%) MI implants were revised for aseptic loosening of the intramedullary stem. Four (15%) of the failed MI implants were revised due to full extension and five (56%) of failed NI implants were replaced as the implant had been fully extended where the patient still required growth.
Conclusion:
Where possible, an NI massive prosthesis should be used in this patient group. Our results suggest that MI prostheses should be infrequently used due to the high incidence of infection. Lengthening of NI prostheses is painless, can be carried out in the clinic and is more cost-effective. However, further work is required to increase the amount of growth potential available in these implants.
Introduction
Skeletally immature patients diagnosed with bone cancer are candidates for limb salvage surgery using an extendible prosthesis. Resection of the bone tumour often involves removing an epiphyseal growth plate, reducing growth of the affected limb. The concept of extendible endoprosthetic replacements was first introduced in Stanmore, England, in 1976 and has been in use since 1983. 1 Extendible devices offer children near normal development and overcome leg-length discrepancy benefiting functional restoration, rapid rehabilitation and quality of life improvement. Minimally invasive (MI) extendible prostheses were designed and introduced in the early 1990s with intramedullary stem fixation and a screw extension mechanism within the shaft of the implant. Extension of the device was produced by making a small skin incision and inserting an Allen key into the screw mechanism that when turned, extended the implant. The main disadvantage of using MI devices is the open surgical procedure that is required to lengthen the implants and the younger the child, the more lengthening procedures are needed. The risk of deep infection increases with the number of surgical procedures and is one of the most devastating complications in bone tumour endoprosthetic surgery. 2 Additional complications associated with multiple surgical procedures for limb lengthening are increased exposure to anaesthetics, ankylosis, nerve damage, soft tissue damage and amputation. 3 Often with the use of MI prostheses, the limb is over extended to reduce the number of surgical procedures.
As a result, non-invasive (NI) growing implants have been developed and these include the Phenix prosthesis 4 and the Stanmore NI growing prosthesis. 5,6 These NI extendable prostheses can be lengthened without the need for repeated surgery. The Juvenile Tumour System (Stanmore Implants, Elstree, UK) introduced in 2002 as an NI implant combines a magnetic disc, a gearbox and a drive screw, where lengthening is controlled using electromagnetic induction. 7 Once implanted, the leg is placed within the centre of a circular external rotating magnetic field, which synchronizes with and turns a magnetic disc located in the shaft of the prosthesis. The magnetic disc drives the gearbox that lengthens the prosthesis at a controlled rate of 0.23 mm per minute. 8 The Stanmore NI extendable prosthesis can be lengthened in small increments without the need for surgical intervention. The aim of this study was to investigate the effectiveness of the Stanmore MI and NI extendible prosthesis inserted into patients over a 16-year period between 1994 and 2010.
Materials and method
Between 1994 and 2010, 105 limb salvage surgeries using MI and NI extendible growing prostheses were performed on skeletally immature patients. Sixty-three patients (31 male and 32 female) received an MI prosthesis and 42 (23 male and 19 female) received an NI implant. MI prostheses were implanted between 1994 and 2009 and NI prostheses between 2002 and 2010. All surgeries were performed for primary bone tumour treatment where osteosarcoma was the most common diagnosis. Twenty-nine patients (69.0%) who received an NI implant and 54/63 (85.7%) MI patients were diagnosed with osteosarcoma. All remaining patients were treated for Ewing’s sarcoma (13 NI patients and 9 MI patients). The mean MI patient age was 11.67 years (range, 4–16 years) and NI, 10.09 years (range, 5–18 years). Patients in the MI group were followed up at a mean of 49 months (range, 1–156 months) and patients in the NI group, 22 months (range, 1–87 months). Sixty-one distal femoral, 21 proximal tibial, 15 proximal femoral, 4 proximal humeral, 2 mid-femoral and 2 total femoral implants were investigated. Each patient received a unilateral implant with 57/105 (54.3%) inserted into the right limb and 48/105 (45.7%) into the left. The mean amount (with standard error) of bone resected in NI patients was 202.48 ± 8.13 mm and 162.46 ± 6.94 mm in MI patients. Depending on bone quality and surgical choice, implants were either cemented or uncemented (35.7% NI and 49.2% MI implants were cementless devices) and all surgeries were performed at a single institution. No patients were recalled and all data were obtained from the medical records. This study was approved by the Royal National Orthopaedic Hospital Institutional Review Board (SE10.017), where appropriate patients received neoadjuvant chemotherapy and all met the criteria for limb salvage.
All prostheses were manufactured on a customized, case-by-case basis. The extension shaft and intramedullary stem were made from titanium alloy (Ti 318, Ti6Al4V), and, when indicated, the stem was shaped to follow the natural curvature of the bone. All NI and MI implants that involved replacement of the knee joint used a SMILES™ rotating hinge total joint (Stanmore Implants). A hydroxyapatite collar, which has previously been shown to enhance osteointegration and bony bridging at the transection site, 9 was located adjacent to the transection site and shoulder of the implant in all patients. The MI implant design consisted of a hollow extension tube that incorporated an extension module manufactured from CoCrMo alloy. The extension module consisted of a telescopic worm wheel screw gearing mechanism that operated with an Allen key. In the MI group, the lengthening procedure required access to the gearing mechanism, which was accomplished through a small skin incision made under general anaesthesia. The Stanmore NI extendible implant has been previously described 5 –8 and extension was undertaken in the outpatient clinic without anaesthesia, using electromagnetic induction of a magnet-driven gearbox within the implant at a rate of 0.23 mm/min at a power of 50 or 100 V. In the NI implant group, the time taken to lengthen the implant was dependent on the discrepancy in leg-length and the site of implantation.
Statistical analysis
Failure was defined as the need for revision of the component and conversion to a different prosthesis. In the NI group, the inability to lengthen was recorded as having a failed gearbox. In the MI implant group, the inability to lengthen was recorded as having a failed extension mechanism. Prostheses with collapsed lengthening mechanisms were listed as failed and recorded as collapsed prostheses. Implants revised due to full extension were also recorded as endoprosthetic failure; however, during revision surgery, only the implant shaft was replaced leaving the intramedullary stem fixation undisturbed. Implant loosening secondary to infection was classified as a failure; however, amputation due to local recurrence and irreversible ischemia were not included in the implant survivorship analysis as these were unrelated to the durability of the prosthesis. The duration of follow-up was from the time of surgery to the time of the latest evaluation. Implant survival was calculated using Kaplan–Meier analysis using overall prosthetic revision and failure due to infection and full extension as the end points. The number of implants that failed due to aseptic loosening was also recorded. Cases without failure were censored either at the time of death or on the date of the last follow-up. The Mantel–Cox log-rank test was used to compare implant survivorship where a p value of <0.05 was considered significant. All analyses were performed using SPSS software (version 17.0; SPSS, Chicago, Illinois, USA).
Results
Five MI patients died of metastatic disease and a sixth MI patient died (6.7%) following cardiac arrest. In the NI group, one patient died of metastatic disease. Twenty-five of the 63 (39.7%) MI implants inserted were revised (Figure 1) and 9 of the 42 (21.4%) NI implants were revised (Figure 2).

Reasons for implant removal in the MI patient group. MI: minimally invasive.

Reasons for implant removal in the NI patient group. NI: non-invasive.
Infection
There were 13 MI prosthetic infections compared to 4 NI infections although not all required revision and 7 were successfully treated with antibiotics. Infection, however, was the major cause of implant failure in the MI patient group. In the MI group, five cases of infection occurred prior to any implant lengthening procedures. Of the remaining eight infections reported, four occurred after one lengthening procedure, two after two lengthening procedures and one after three lengthening procedures. In the remaining infected case, the time of the reported infection had not been recorded. Of these infections, nine MI (35%) implants were revised due to septic loosening (two cemented and seven uncemented implants), whereas only one (11%) NI implant was revised due to infection. Of the nine MI implants revised, eight of these implants had been lengthened and consisted of one cemented proximal tibial, one uncemented proximal humeral, one uncemented proximal femoral and four uncemented and one cemented distal femoral replacement implants. The uncemented proximal tibial NI implant was revised due to infection following three lengthening procedures. Failed two-stage revision surgery was carried out on the infected NI prosthesis and two of the infected MI prostheses and all eventually resulted in amputation. The mean time until infection was 15.5 months in the NI group and 19.2 months in the MI group with no significant difference found between the two sets of data.
Aseptic loosening
None of the NI implants failed due to aseptic loosening; however, six (23%) MI implants were revised for aseptic loosening of the intramedullary stem (three were cemented and three uncemented stems). These six revision surgeries occurred at 14-, 19-, 22-, 28-, 39- and 47-month post-limb salvage. Four patients received a distal femoral replacement, one a proximal tibial replacement and one a proximal humeral replacement. Two of the four distal femoral replacements failed due to loosening of the tibial component where one was cemented and the other uncemented. The remaining two distal femoral prostheses failed due to loosening of the uncemented femoral intramedullary stem. Both the proximal humeral and proximal tibial replacements failed due to loosening of the cemented stem.
Full extension
Four (15%) MI implants were revised due to full extension where further growth of the limb was required. However, five (56%) of the failed NI implants were revised due to full extension.
Lengthening failure
Mean implant lengthening in the MI group was 37 mm (range, 10–130 mm), which required a mean of three lengthening procedures (range, 1–9). In the NI patient group, implants were lengthened to a mean of 21 mm (range, 0–88), which required a mean of four lengthening procedures (range, 1–10). The mean length achieved during each lengthening episode in the MI group was 14 mm (range, 8–21 mm) and 5 mm (range, 1–11 mm) in the NI patient group. Twenty-six MI and 22 NI prostheses were not lengthened with the main reasons being poor patient condition, early death or amputation. One implant in the MI group (11%) and three (33%) in the NI group were revised following failure of the gearbox. The failures in the NI group occurred soon after the introduction of the device and manufacturing and testing protocols were then put in place, which resulted in no further failure. Four (15%) MI implants were revised due to prosthetic collapse.
Amputation and nerve palsy
Two patients (3.2%) in the MI group underwent amputation due to tumour recurrence and irreversible ischemia where both resulted in an above the knee amputation. Five patients with distal femoral prostheses (four MI and one NI) demonstrated poor range of knee motion that was made worse after implant extension and resulted in fixed flexion deformities. A patient implanted with an MI prosthesis suffered a common peroneal nerve palsy after a lengthening episode (15 mm); however, this patient recovered to full function after 13 months. No patients with NI endoprostheses reported nerve palsies.
Implant fracture
One MI proximal tibial prosthesis fractured 15-month post implantation following a fall. This prosthesis was revised to another MI prosthesis.
Survival analysis
Kaplan–Meier analysis showed the probability of an MI bone tumour implant surviving with respect to implant revision due to implant failure for any cause and at a mean follow-up of 49 months was 58.8%. The survival of an NI implant at a mean of 22 months was 78.6%. No significant difference in overall survivorship between these two patient groups was found (Figure 3). Implant survival in the NI patient group at 1-year post operation was 97.1 ± 2.8% compared with 96.7 ± 2.3% in MI patients. At 7-year post-surgery implant, survivorship had decreased to 40.4 ± 14.4% in the NI group and 45.0 ± 7.9% in the MI patient group. If full extension was removed from the data as a form of implant failure, survivorship analysis demonstrated that at 7-year post operatively, NI prostheses had a survival rate of 76.3% and MI prostheses a survival of 49.0%.
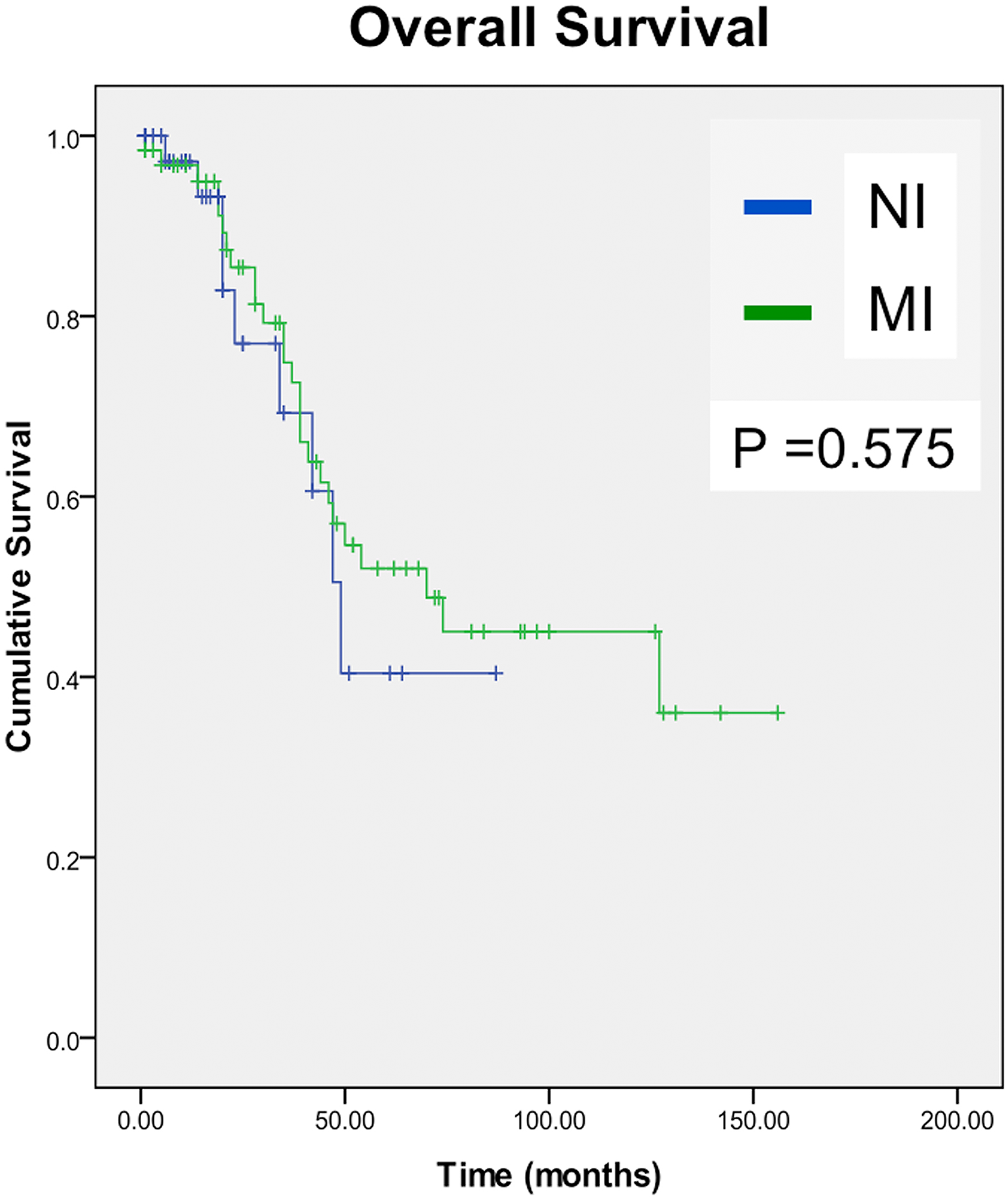
Kaplan–Meier survival analysis with respect to implant revision due to implant failure for any cause.
Implant survivorship analysis with infection as the endpoint showed a significant difference between groups (p = 0.042; Figure 4). Only one NI implant failed due to infection at 20-month post-surgery giving a survival of 94.4% ± 5.4% over the study period of 7 years. The probability of failure due to infection in the MI patient group decreased from 98.3 ± 1.7% at 1-year post-surgery to 76.2 ± 8.3% at 7-year post-surgery.

Kaplan–Meier survival analysis with respect to implant revision due to infection.
Full extension accounted for 56% of NI prosthetic failures and 15% of MI implant failures (p = 0.005). Kaplan–Meier analysis of implant survivorship with full extension as the endpoint showed that at 1-year post-surgery, implant survival was 96.7 ± 3.3% in the NI patient group and 94.8 ± 2.9% for MI prostheses. At 7-year post operation, MI implants demonstrated a survival rate of 76.3 ± 11.1% and NI implants 49.5 ± 7.9% (Figure 5).

Kaplan–Meier survival analysis with respect to implant revision due to full extension.
Discussion
Earlier designs of extendible prostheses were modular, where the midsection of the implant was exchanged for progressively longer sections. These designs required large surgical incisions to exchange the extension parts. Therefore, implants were superseded by MI designs, which required a small incision under anaesthesia to expand the prostheses. Expansion of these implants increased the risk of anaesthetic complications and infection and NI designs were introduced in the 1990s. Our study investigated survival of the Stanmore MI and NI extendible prostheses over a period of 16 years. Patient survival compared favourably with other studies that have investigated the use of extendible endoprostheses 2,3,5,10 and our results found no statistically significant difference in overall implant survival when the two groups were compared. The commonest reason for failure of MI endoprostheses was peri-implant infection, whereas full extension was the main reason for NI implant revision surgery.
Deep infection after endoprosthetic replacement of a bone tumour is a major complication associated with significant morbidity, increased number of surgical procedures, prolonged rehabilitation, pain, worse functional outcome and revision surgery, where failure of revision can result in amputation. Factors that increase infection include radiation therapy, ‘maintenance surgery’ (e.g. bushing replacement), patellar procedures and anatomic site (particularly involvement of the tibia). 11 Infection has also been associated with difficulty in obtaining soft tissue coverage of the prostheses following limb reconstruction, which is more problematic in proximal tibial replacements. 12 These factors combined with the size of the implant, the peri-operative time and immunosuppression associated with chemotherapy 6 may explain why six patients (five MI and one NI) developed an infection within 7 months of surgery and before any invasive limb lengthening procedures had taken place. This study identified an infection rate of 9.52% in the NI implant group and 20.97% in the MI patient group, which is similar to previous studies where infection rates were measured ranging from 4% 13 up to 40%. 3 In our study, 8 of the 13 reported MI infections occurred after the lengthening procedures had begun and all 8 of these implants were revised. Jeys et al. 11 reported an increased infection risk of 0–5% with each MI lengthening. Grimer et al. 14 reported 5 lengthening-associated infections in a study of 20 patients with extendable tibial prostheses, while studies by Ayoub et al. 15 and Eckardt et al. 16 noted no lengthening-related infections. In our study, most infections appeared after one lengthening procedure with fewer infections noted after three lengthening procedures. However, a study by Hantes et al. 17 reported an increased incidence and severity of complications (including infection) with increases in lengthening and a retrospective study by Eckardt et al. 16 demonstrated significant complications in 56% of patients with extendible prostheses, although this study also showed that the lengthening procedures themselves did not cause any infections. The NI implants investigated in this study were inserted more recently (2002–2010) when compared with MI implants and it is possible that the difference in infection rates may also in part be due to the benefits from recent advances in hospital infection control and patient management. It may also be due to the relatively recent use of a gastrocnemius flap during surgery, which has been shown to decrease the rate of infection in limb salvage procedures. 12 However, in our study, gastrocnemius flaps were used in every case. Silver-coated implants have demonstrated good antimicrobial activity and have been introduced into oncological musculoskeletal surgery with success 18 ; however, in this study, none of the NI or MI implants investigated were silver-coated.
Full extension where growth of the limb was still required was the main long-term complication resulting in revision of NI implants. These findings are similar to those reported by Sewell et al. 8 who also found that full extension was a major reason for revision surgery. This may be due to the NI prostheses having a lower lengthening capacity compared with MI prostheses, which is due to the extra size associated with the magnet and gearbox. As full extension is not necessarily ‘implant failure’, when these results were excluded, survivorship analysis demonstrated that at 7-year post operatively, NI prostheses had a higher survival rate of 76.3% when compared with MI prostheses (49.0%). Complications that may interrupt long-term success due to early revision of an NI implant following full extension are unknown. Optimal fixation of the implant within bone is essential and, therefore, if both bone quality and quantity are sufficient, then it is possible that implant success would not be further compromised. A recent study investigated the use of NI implants for the revision of previous endoprostheses and reported it to be a successful option in the mid-term with a revision-free implant survival of 75% at 2 years reducing to 55% at 5 years. 19 Nevertheless, further investigation is required to establish factors that affect the long-term survival of these implants following both primary and revision surgery.
Aseptic loosening of extendible massive bone tumour endoprostheses is also a major complication causing implant failure. Increased bone resection levels following distal femoral and proximal tibial implant surgery are associated with increased rates of aseptic loosening 20 and results from our study found a 23% MI loosening rate with no NI failures, despite NI patients having a significantly larger mean bony resection level. Prosthetic aseptic loosening is a mid-term complication and has been reported to occur within 3–9 years after primary surgery. 21,22 Therefore, in our study, it is possible that aseptic loosening of MI prostheses may be increased when compared with NI prostheses due to the longer follow-up period.
Lengthening procedures confer a significant improvement in the functional score of growing patients. 10 In our study, some implants were not lengthened (48/105), with the main reasons being poor general condition, early death or amputation. Fifty-four percent of implants were lengthened and this is similar to lengthening rates reported in the literature (50–75%). 16,23 Gearbox failure or a collapsed lengthening mechanism resulted in failure in both groups. Early physiotherapy may prevent extensive tissue scarring which may reduce the force exerted on the gearbox during lengthening. The results reported in this study are relatively short-term but show that NI implants may reduce the incidence of decreased ROM and nerve palsies as shorter lengthening episodes can occur more often.
A limitation of this study is the relatively small number of patients in each of the surgical reconstruction groups as only 50 paediatric patients are treated for sarcoma with limb salvaging techniques per year in the United Kingdom. 24 A second limitation is that this study was carried out retrospectively with analysis of patients over a relatively short postoperative follow-up period. A recent study by Gilg et al. 25 investigated a similar number of NI extendible implants but at a longer mean follow-up time of 64 months. This study reported a higher implant infection rate (19.6%) and it is conceivable that this difference in outcome may in part be due to our shorter post-surgical follow-up window. In this study, variation was minimized as all implants were made by a single manufacturer. Surgical techniques and patient care were also consistent as all patients were treated at a single institution. MI prostheses are infrequently used at our hospital and results showed that infection (35%) was significantly higher when compared with NI patients (11%). However, at the follow-up period investigated in this study and when all reasons for failure were taken into account, overall implant survival was relatively low in both groups and it is important to consider that rates of implant infection are expected to further increase in both patient cohorts following revision surgery. 26 Lengthening of NI prostheses is painless, can be carried out in the clinic and in cases where multiple lengthening procedures are required, it may be more cost-effective as unlike MI lengthening, it does not require hospitalization, a general anaesthetic and additional surgery. However, to accommodate an NI implant, the amount of bone resected during primary surgery may be increased and further work is required to improve the amount of growth potential available in these implants.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.