
Abstract
Background:
The clinical indications for elbow arthroscopic procedures have expanded through last decades. The aim of the study was to assess the functional results and patient satisfaction after arthroscopic treatment of various elbow conditions after a minimum 5-year follow-up.
Methods:
We conducted a retrospective study of a consecutive patient cohort who had undergone unilateral elbow arthroscopy between 2008 and 2010. The main outcomes were Disabilities of the Arm, Shoulder and Hand (DASH) score and a specific patient-reported outcome measure questionnaire after a minimum 5-year follow-up.
Results:
In total, there were 93 patients in the cohort with different diagnoses. Majority of patients were suffering from elbow osteoarthrosis. After the average follow-up of 72 months (range 60–96 months), the response rate was 67%. Eighty two percent of patients were satisfied with the pain relief and locking of the elbow was relieved in 70% of patients. Elbow range of motion (ROM) improved in 80% of the 55 patients who had a limited ROM before the operation. The overall patient satisfaction after elbow arthroscopic treatment was good. There were no differences in median DASH score between patients with or without post-traumatic condition, but the median DASH score for patients who had severe (grade 3) osteoarthrosis before the operation was significantly worse. There were no major complications reported in this cohort.
Conclusions:
Arthroscopic treatment of various elbow conditions was associated with good patient satisfaction and reduced symptoms without major complications.
Keywords
Introduction
The typical indications for elbow arthroscopic procedures include decreased range of motion (ROM) or pain of the elbow joint caused by osteoarthrosis, loose bodies, post-traumatic arthrofibrosis, osteochondritis dissecans, synovitis, septic arthritis, and rheumatoid arthritis. 1 In addition, arthroscopy can be utilized in the diagnosis and assessment of the severity of many elbow conditions and in the operative treatment of posterolateral rotatory instability, posteromedial impingement, and plica in the elbow joint, fractures of the capitellum, coronoid and radial head, and lateral epicondylitis. 2,3
Previous studies have suggested that arthroscopic debridement may be an effective treatment for elbow osteoarthrosis if nonoperative treatment fails. However, according to Yeoh et al., there is still a lack of evidence to support the use of elbow arthroscopy in the treatment of primary osteoarthrosis. 3 Arthroscopic elbow surgery may relieve the mechanical symptoms of locking or catching by the removal of intra-articular loose bodies. 3,4 Kim and Shin reported clinical improvement in elbow ROM in 92% of patients (from 79° to 121°) after arthroscopic treatment of arthritic elbows with limited ROM in a retrospective cohort of 63 elbows. Furthermore, no difference between patients with degenerative versus post-traumatic etiology was found. 5 According to the literature, patients with rheumatoid arthritis of the elbow joint achieve improvement in pain, joint motion, and upper-limb function after arthroscopic synovectomy. 6
The popularity of elbow arthroscopy operations 7 and the number of published studies on the procedure have increased exponentially over time.8 There is, however, a paucity of studies with long-time follow-up which report patient satisfaction after elbow arthroscopy. Moreover, there have been no prospective randomized controlled studies. 3 The majority of the published studies on elbow arthroscopy have not reported the surgical results according to standardized patient-reported outcome measures (PROMs), which makes comparison between the studies difficult. 8,7
The aim of the study was to assess the functional results and patient satisfaction after arthroscopic treatment of various elbow conditions with a minimum 5-year follow-up. The hypothesis was that the arthroscopic treatment is associated with reduced symptoms and good patient satisfaction.
Materials and methods
The patient cohort was identified from the electronic medical records of Tampere University Hospital (Tampere, Finland). All patients who underwent unilateral elbow arthroscopy from 2008 through 2010 were included. The surgical procedures were classified according to the Nordic Classification of Surgical Procedures (NCSP codes NCA30, NCE10, NCE25, NCF15, and NCF25). Our search strategy for procedures and the corresponding NCSP codes for the elbow included the terms diagnostic arthroscopy, debridement, capsulectomy, and synovectomy. The minimum follow-up period was 5 years. The final study cohort comprised 93 patients. The preoperative patient data and symptoms were identified from the medical records in order to minimize patients’ recall bias. The follow-up PROMs were specific questionnaires.
The primary outcome in this study was the Finnish version of the Disabilities of the Arm, Shoulder and Hand (DASH) questionnaire. The other outcomes were patient self-evaluation questions about pain relief, locking of elbow, ROM, and patient satisfaction after the procedure. The questions included assessment of pre- and postoperative symptoms and whether patients would choose to undergo the procedure again in future if needed.
Patients were retrospectively reviewed for age, sex, underlying diagnoses associated with the elbow arthroscopy, prior elbow trauma or surgery, the presence of mechanical locking, instability, pain, and limited ROM of the elbow. The surgical records were used to confirm the side of operation (left/right), the portals used and performed procedures, and all complications. For further analysis, those patients who had primary or post-traumatic arthrosis were grouped into three categories, based on preoperative X-rays and surgical reports. The categories were according to the Broberg and Morrey classification system: slight (grade 1), moderate (grade 2), and severe (grade 3). 9 Patients who had osteoarthrosis (n = 55) were analyzed also as a subgroup. Preoperative radiographs of the involved elbow were available for inspection for 31 patients.
Statistical analysis
Descriptive data were presented with median values because the distribution was skewed. The statistical analysis was performed by Kruskal–Wallis test because normal distribution could not be assumed. Differences were considered statistically significant when p < 0.05. All calculations were performed with SPSS 22.0 (IBM, NY, USA).
Results
The study cohort comprised of 22 women and 71 men and the mean age at the time of the first arthroscopic procedure was 44.6 years (range 12–82 years). Seventy-four patients had the procedure performed once and 19 patients had two or more elbow arthroscopies. The right elbow was operated in 58 patients and the left in 35 patients. The most common preoperative diagnosis was primary osteoarthrosis of the elbow for 43 (46%) patients (Table 1). Post-traumatic condition was found from 25 (27%) patients and of those post-traumatic osteoarthrosis was found for 13 patients (14% of total 93 patients). A total of 10 patients (11%) had an arthroscopy performed due to osteochondritis dissecans and 15 patients (16%) due to either rheumatic arthritis or other arthritis (e.g. haemophilia and meloreostosis). Preoperative elbow pain was described for 80 patients (86%) and 32 patients (34%) reported locking symptoms of the elbow joint. Elbow instability was recorded for seven patients. Preoperative ROM was considered limited for 74 patients (80%) and the average preoperative ROM was 93° (range 50°–145°).
Diagnostic groups and DASH scores of the patients.
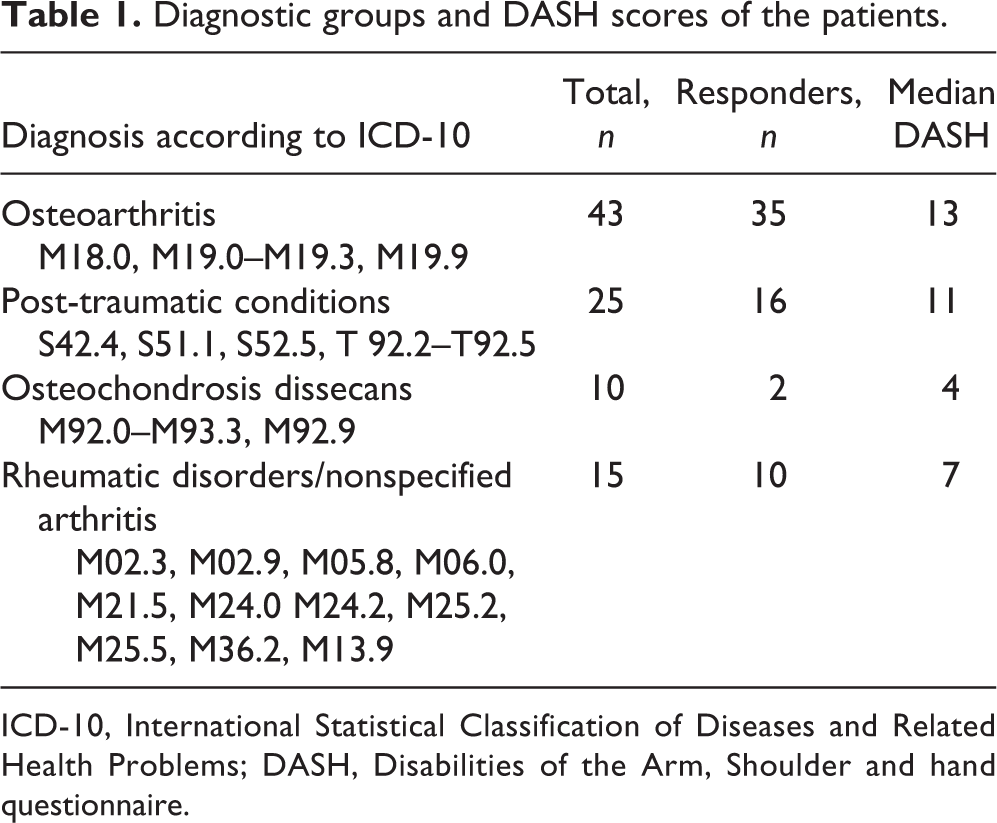
ICD-10, International Statistical Classification of Diseases and Related Health Problems; DASH, Disabilities of the Arm, Shoulder and hand questionnaire.
There were 46 men and 17 women among the patients who responded to the follow-up questionnaire. The average follow-up period was 72 months (range 60–96 months) and the overall response rate was 69% (64 of the 93 identified patients). Sixty-one patients returned a completed DASH questionnaire and the median post-operative DASH score was 11.5 points.
Results of the follow-up questionnaire are summarized in Table 2. Fifty-three of the 64 patients who completed the questionnaire (83%) were satisfied with the pain relief and similarly—but not exactly the same—52 patients (81%) were satisfied with the overall results of the treatment. Nine patients (14%) reported insufficient relief of pain. Locking of the elbow was relieved in 13 of the 27 patients (48%) who had locking before the operation, but five patients, who did not have elbow locking before the operation reported locking after the operation. However, all of those five patients reported overall satisfaction with the results of the operation. Elbow ROM improved in 44 (80%) of the 55 patients who reported a limited ROM before the operation. All but three patients reported that they would choose to undergo the operation again if needed.
Results of the questionnaire after the postoperative follow-up.

ROM: range of motion.
The median DASH scores were also calculated for subgroups based on different diagnosis (Table 1) or for subgroups with based on the osteoarthrosis grade regardless of the primary diagnosis at the time of the operation. The severity of osteoarthrosis was categorized as mild (grade 1) in 26 patients (46%), moderate (grade 2) in 24 patients (46%), and severe (grade 3) in 5 patients (8%). After the follow-up, the median DASH score was similar between the different diagnosis groups but higher (p = 0.015) in patients with severe osteoarthrosis (Table 3). The DASH scores were also calculated for the patients with trauma history regardless of primary diagnosis or osteoarthrosis. The median DASH scores after the follow-up for patients with no trauma history (N = 36) or with previous trauma (N = 24) were 10 and 13, respectively.
Subgroup of patients with osteoarthrosis.

IQR: interquartile range.
A repeated arthroscopy was performed for 19 patients during the follow-up and the questionnaire was received from 15 of these patients. The reasons for re-arthroscopy were persistence of symptoms or reappearance of symptoms after a symptomless period. The median DASH score of patients with repeated elbow arthroscopy (14 patients) was 26.5 points.
No major nerve damage, joint infections, or other complications were described in this cohort. Two patients had persistent pain and one of them was not satisfied with the results of the operation.
Discussion
The main findings of our study were the good functional results and the overall subjective satisfaction after elbow arthroscopic surgery. The advantages of the study include a long follow-up period, comprehensive and consecutive cohort of 93 patients, and sufficient response rate (69%). We reported a specific questionnaire and DASH score as a standardized PROM.
After the follow-up, the DASH scores for patients with repeated arthroscopy and severe osteoarthrosis were worse. It has been shown previously that arthroscopic treatment seems to provide better results if osteoarthrosis is treated earlier and joint congruence is still preserved. 10,11 This finding is comparable with our results. Studies of healthy general populations have reported an average DASH scores ranging from 10.1 to 14.7 12,13 and in our cohort DASH scores for patients who have had elbow arthroscopy did not differ from the normal population. Regarding the trauma history, there was no difference in postoperative DASH scores after the follow-up.
Osteoarthrosis was the most common indication for arthroscopic treatment in our cohort. Primary osteoarthrosis is a relatively rare condition that comprises only 1–2% of patients of elbow arthritis. 11,14,15 According to the literature, elbow osteoarthrosis results often from trauma to the elbow 11,14 –17 and radiographic osteoarthrosis is a common sequela of elbow trauma. 18 Also osteochondritis dissecans or synovial osteochondromatosis increase the risk for osteoarthrosis. 19 In our study, most of the patients who were treated with arthroscopic procedures had some cartilage damage identified both radiologically and during the arthroscopic evaluation. Chondral or osteochondral lesions, post-traumatic contracture, and loose bodies of the elbow are often associated with chronic pain, stiffness, and joint blockages. 20 These were the main indications for arthroscopy also in our cohort.
Symptomatic elbow osteoarthrosis is less prevalent than the presence of radiological degenerative changes in the joint. 21 Multiple factors may play a role in the development of osteoarthrosis of the elbow, but there is a correlation between the injury pattern and the amount of energy absorbed within the joint in the development of post-traumatic osteoarthrosis. 21,14 Nonetheless, the natural course of cartilage defects is not completely understood. The symptoms of the patients in the study cohort were predominantly pain and/or stiffness or limitation in ROM of the elbow joint, which is in agreement with the previous reports. 14,22
Eighty-one percent of patients were satisfied with the results of elbow arthroscopic treatment. However, patient satisfaction is a biased outcome measure of surgery. 15 It has been shown that in shoulder and elbow surgery, patient satisfaction is not always associated with measures of function, physical impairment, or expert assessment. 15,23 In our study, patients filled the questionnaires at home and the study participation provided no benefits to the patients. Although still susceptible to bias, patient satisfaction should be included in the evaluation of elective surgery. In the study cohort, all but three patients responded that they would choose to undergo elbow arthroscopic surgery again in the future if needed. Even though the median DASH score was significantly higher for patients who had repeated elbow arthroscopic procedures, they were still contented with the treatment and reported satisfactory pain relief and improvement of elbow function without any complications. However, there were five patients who reported locking of the elbow which occurred only after the operation, but it has been noted that the definition of joint locking is not always self-evident to the patients. Accordingly, the definition of locking should therefore be better specified in future studies.
There were no reports of nerve damage in the study cohort. In the previous studies, the overall complication rate is 6% to 15% and half of those complications were nerve lesions. 24,25 It is possible that temporary nerve paresthesias were not recorded, but there was no indication of any major nerve damage or other complications.
In the study cohort, the patients commonly had limited motion of the elbow joint, with or without locking, and pain which caused difficulties in daily activities. Our results are in agreement with the previous studies in which elbow arthroscopic techniques have been shown to be effective and safe procedures 15,24,26 and the reported outcomes of elbow arthroscopy include improvements in ROM, pain, and functional scores. 3,8,27 These may be considered as the clinically important symptoms which assist in the clinical decision-making and in the evaluation of the treatment outcome. In retrospective studies, inconsistency of measurements is an inherent problem and we decided that the unreliable data about changes in ROM are secondary to patient-reported outcome regarding symptoms. Self-assessment is a patient important outcome, although it can’t be interpreted in a similar manner with absolute changes in numerical ROM.
Previous studies which have reported changes in the range of movement and pain relief of the pain 10,28 are in accordance with our results. Cohen et al. 28 reported a prospective cohort study that compared open and arthroscopic elbow debridement in patients with primary osteoarthrosis or post-traumatic osteoarthrosis. The data suggested that the arthroscopic procedure provided greater pain relief but the open procedure resulted in a better ROM. 28 A systematic review of the outcomes of arthroscopic debridement for the treatment of primary osteoarthrosis of the elbow 29 identified two studies with visual analog scale (VAS) score for pain as one of the outcomes and both of them reported significant improvement after the operation. Lim et al. reported improvement in pain VAS (0–10) from 4.5 to 2.2 points after the procedure with mean 38 months follow-up. 30 Similarly, Galle et al. reported improvement in pain VAS from 6.6 to 1.6 points after surgery. 31 Merolla et al. have reported a retrospective cohort of 48 patients with either primary or post-traumatic osteoarthrosis treated with arthroscopic joint debridement and assessed pain VAS at the final follow-up visit at 44 months. Pain VAS improved from 7.2 to 4.3. 11 Similarly, MacLean et al. have evaluated a retrospective cohort of 20 patients with osteoarthrosis of the elbow who had underwent arthroscopic debridement and capsulectomy. After the procedure, Mayo and DASH scores were improved and they further suggest that arthroscopic debridement may work as a partial neurectomy to denervate pain sensation in the joint. 32
There are some limitations in the study. The main weakness of our study is its retrospective nature. The study cohort included all consecutive elbow arthroscopic surgery patients regardless of the diagnosis or indication for the operation. This dilutes the applicability of the results in a specific condition, but often the actual indication for the arthroscopic elbow procedures is based more on the symptoms and clinical findings than on the diagnosis of the condition. Another limitation is that the change in ROM of the elbow was not uniformly applicable because many exact values of preoperative or postoperative measurement of ROM were missing.
As a conclusion, the present study demonstrates that arthroscopic treatment provides for beneficial outcomes in terms of patient satisfaction, function, and pain relief without complications in an unselected study population. But there is need for prospective randomized trials using valid outcomes including patient reported outcome measures.
Footnotes
Authors’ note
Mr Mika Helminen, University of Tampere, provided statistical assistance in the preparation of the manuscript.
Author contributions
All authors were involved in the design of the study. MK conducted the survey and collected the study data. All authors contributed to the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.