
Abstract
Background:
Reconstruction of Myerson type III (defect size more than 5 cm) chronic Achilles tendon ruptures (CATRs) is a surgical challenge due to its large Achilles tendon defect. This study aims to describe our operative technique for Myerson type III CATR and its clinical outcomes.
Patients and Methods:
From May 2012 to April 2015, we treated seven patients (6 males, 1 female) with Myerson type III CATR using semitendinosus tendon and gracilis tendon autograft. The mean age was 47.3 years (range: 37–56). Patients were followed for a mean time of 31.3 months. All patients’ defect size between Achilles ends after debridement was more than 5 cm and hence classified as Myerson type III. The clinical outcomes were evaluated by visual analog scale (VAS) for pain, American Orthopaedic Foot and Ankle Society (AOFAS) ankle and hindfoot score, Achilles tendon total rupture score (ATRS), and the Short Form 36 (SF-36).
Results:
All patients reported good postoperative clinical outcomes. The average AOFAS score increased from 54.29 points (range: 46–65 points) preoperatively to 97.57 points (range: 90–100 points) at last follow-up. The average ATRS increased from 51.43 points (range: 40–61 points) preoperatively to 92.71 points (range: 83–100 points) at last follow-up. And the average VAS for pain was 0 at the last follow-up. The mean value of SF-36 physical increased from 32.14 points (range: 25–35 points) to 90 points (range: 80–95 points). And the mean value of SF-36 mental was improved from 37.14 points (range: 32–40 points) to 90.86 points (range: 84–96 points).
Conclusions:
Semitendinosus tendon combined gracilis tendon autograft is a safe and effective technique in the reconstruction of Myerson type III CATR.
Introduction
Achilles tendon is the strongest tendon in the human body, but the most easily ruptured tendon in the lower limb. 1 Achilles tendon rupture often occurs in young athletes and middle-aged men who occasionally participate in sports. 2 Chronic Achilles tendon ruptures (CATRs) are usually defined as a rupture which had not been treated for 4–6 weeks. 3 The incidence rate of CATR is low in modern medical conditions. 2,3 Misdiagnose, neglect, or unrecognized acute rupture often leads to CATR. 4 Surgery was usually offered to patients with CATR who failed to improve with conservative treatment measures or wish to participate in activities in the past. 3 However, some recent studies 5,6 have shown we can directly to surgery if gap is more and MRI shown unhealthy tendon tissue. According to the defect size of Achilles tendon, Myerson 7 (Table 1) described a classification system and surgical treatment principles for CATR. There are some surgical options to treat Myerson type III CATR, such as allografts, xenografts, synthetic grafts, V-Y tendon plasty combined with fascia turndown, 8 flexor hallucis longus (FHL), 9 semitendinosus, 4 flexor digitorum longus (FDL), 10 or peroneus brevis 11 tendon transfer. However, the specific choice of surgical methods is still controversial. The purpose of this retrospective study is to report our surgical technique using semitendinosus tendon and gracilis tendon autograft in the repair of CATR and its clinical outcomes.
Scheme for the surgical treatment of chronic Achilles tendon ruptures on the basis of gap size.a

aFrom Myerson. 5
Patients and methods
After approval by the institutional review board, we performed a retrospective clinical study.
The inclusion criteria were CATR for more than 6 weeks and patients classified as Myerson type III (defect size more than 5 cm) indicative to this surgery. The exclusion criteria were Achilles tendon re-rupture, CATR caused by local steroid injection, steroid taken for other disease, posterior foot infection, prior foot surgery, diabetes mellitus, peripheral arterial disease, and the length of distal residues of the Achilles tendon less than 2.5 cm.
Seven patients (6 males, 1 female) who underwent semitendinosus tendon and gracilis tendon autograft for Myerson type III CATR between May 2012 and April 2015 were included in this retrospective study (Table 2). All seven patients were examined by ultrasound or MRI scan and they all had unilateral CATR (4 left, 3 right). In addition, the diagnosis of CATR also combined injury history and physical examination such as the Calf Squeeze Test, the Knee Flexion Test, and Single Leg Heel Rise Test. The injury mechanism in this study involved two ankle sprains, three sports injuries, and two slipped. The follow-up of this study was until January 2018, with an average follow-up duration of 31.3 months (range: 26–36).
Patients.
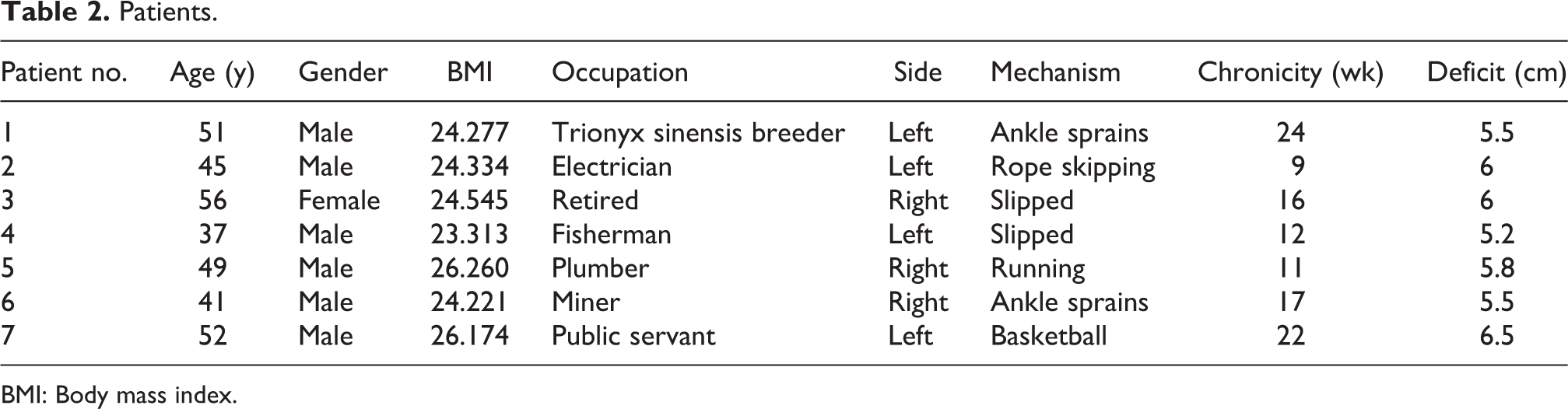
BMI: Body mass index.
We evaluated the outcomes with physical examination, radiography (mainly MRI), visual analog scale (VAS) for pain (of 0–10), American Orthopaedic Foot and Ankle Society (AOFAS) ankle and hindfoot score, Achilles tendon total rupture score (ATRS), 12 and the Short Form 36 (SF-36). 13
Surgical technique
All the procedures were performed by our corresponding author. Patients were operated under lumbar plexus + sciatic nerve block anesthesia and in the prone position with a thigh pneumatic tourniquet inflated to 350 mmHg. A posterior internal incision was performed to expose ruptured Achilles tendon. Then we took a thorough debridement by debriding the dystrophic tendon ends but preserving the vascular fibrous stumps and then measured the defect size between Achilles ends by keeping the knee in the straightened position and the ankle in the neutral position. All patients’ defect size between Achilles ends was more than 5 (range: 5.2–6.5) cm and hence all classified as Myerson type III. The mean length of the distal residues of the Achilles tendon was 3.8 (range: 3.0–5.5) cm. Patients whose defect size was more than 5 cm were selected for reconstruction using semitendinosus tendon and gracilis tendon autograft. With the knee flexed in 90°, a 3- to 4-cm vertical incision was performed at the pes anserinus and then semitendinosus tendon and gracilis tendon were both harvested. The muscular part of the tendon was shaved off, and the tendon was prepared for autograft. A scalpel was used to create a tunnel at the coronal plane of two residues part of Achilles tendon and this tunnel was ≥2 cm from the Achilles ends. Semitendinosus tendon and gracilis tendon were used to bridge suture the defect between Achilles ends (i.e. semitendinosus tendon using Kessler suture and gracilis tendon using surround suture, all using number 2 ETHIBOND® sutures). Then the semitendinosus tendon and gracilis tendon were sutured together using 4-0 ETHICON® sutures. The remains of the autograft tendon were split by a scalpel and then fan-shaped spread sutured using 4-0 PROLENE® sutures to prevent adhesion. After that, a 4-0 PROLENE suture was used to close the paratenon as a separate layer, and the skin was closed with 3-0 STRATAFIX™ knotless tissue control device (see Figures 1 and 2). A below-the-knee cast was applied immediately after surgery with the ankle in 30° plantar flexion. Postoperative follow-up visits were conducted in our outpatient clinic at week 2, week 4, week 6, month 3, month 6, month 9, year 1, and then once every 6 months. The physical examination and clinical outcome were evaluated by an independent orthopedic surgeon.

Drawing of operative techniques.

(a) A posterior internal incision was performed to expose ruptured Achilles tendon. (b) Semitendinosus tendon and gracilis tendon were prepared by shaving off the muscular part of the tendon. (c) Semitendinosus tendon using Kessler suture and gracilis tendon using surround suture. (d) and (e) Paratenon was closed with 4-0 PROLENE® sutures as a separate layer. (f) Skin was closed with 3-0 STRATAFIX™ knotless tissue control device.
Patients were maintained in a non-weight-bearing position in the plaster cast for 6 weeks. The plaster cast was removed 6 weeks postoperatively and then patients started partial weight-bearing with two crutches and wore a 1-cm heel-raised footwear in the involved foot. Meanwhile, patients started physiotherapy in our rehabilitation center. The full weight-bearing was started after 3 months. We suggested patients avoiding vigorous activity for 6 months postoperatively.
Results
The results of the surgical treatment are listed in Table 3. The average follow-up (routine office visits) duration was 31.3 months (range: 26–36). None of the patients exhibited any difficulty in walking or climbing stairs. All the patients returned to daily activity, and three of them returned to sports. All of them were able to do a sustained single stance heel raise. The average AOFAS score increased from 54.29 points (range: 46–65 points) preoperatively to 97.57 points (range: 90–100 points) at last follow-up. The average ATRS increased from 51.43 points (range: 40–61 points) preoperatively to 92.71 points (range: 83–100 points) at last follow-up. And the average VAS for pain was 0 at the last follow-up. The mean value of SF-36 physical increased from 32.14 points (range: 25–35 points) to 90 points (range: 80–95 points). The mean value of SF-36 mental was improved from 37.14 points (range: 32–40 points) to 90.86 points (range: 84–96 points). At the last follow-up, the size of the involved side’s calf circumference (mean value 35.6 cm) was close to the contralateral side (mean value 36.5 cm). We measured the ankle circumference at 7.5 cm above the calcaneal tuberosity, because it is near the defect of Achilles tendon in our seven cases. The mean value in the involved side was 21.8 cm at last follow-up, approximately equal to the contralateral side with 21.4 cm (Figures 3 and 4). There were no reported re-ruptures, deep infection, numbness, deep venous thrombosis, or peripheral nerve lesion during hospital stay and later follow-up.
Functional outcome.

AOFAS: American Orthopaedic Foot and Ankle Society; ATRS: Achilles tendon total rupture score; VAS: visual analog scale; SF-36: Short Form 36; post-op: postoperative; pre-op: preoperative.
aLast follow-up.
bAnkle circumference at 7.5 cm above the calcaneal tuberosity.

Postoperative T2-weighted MR images of patients no. 1 at last follow-up.

Clinical photographs showing the functional outcome after Achilles tendon reconstruction with semitendinosus tendon and gracilis tendon autograft.
Discussion
Due to the retraction of tendon edge and local vascular damage, CATR is difficult to manage and may have poor outcomes. Therefore, the treatment of CATR remains a surgical challenge. 3,14 According to the treatment principles of CATR from Myerson, 7 defects greater than 5 cm were repaired using tendon transfer alone or in combination with V-Y advancement or turndown. Kraeutler et al. 14 summarized evidence-based recommendations for treatment options for CATR. Autograft reconstruction belongs to grade B recommendation (treatment options are supported by fair evidence; i.e. consistent with level III or IV studies) and V-Y tendon plasty and turndown flap belongs to grade C recommendation (treatment options are supported by either conflicting or poor-quality evidence; i.e. level IV studies). Autograft reconstruction mainly includes FHL, semitendinosus, gracilis, FDL, and peroneus brevis tendon transfer. 14 However, some complications of autograft reconstruction have also been reported, such as a decrease in range of movement and muscle strength in the donor site and affected joints. 7,15
Hamstring tendon autografts were used to reconstruct the anterior cruciate ligament for its sufficient strength and favorable harvest. 16 In recent years, it has been used in the reconstruction of CATR. 4,17 –21 Some previous studies used the semitendinosus tendon or gracilis tendon alone to reconstruct CATR, 4,17 –21 which have achieved satisfactory clinical outcomes. We think that using semitendinosus tendon combined gracilis tendon autograft will be more stronger and stiffer. Our opinion was supported by the study of Hamner et al., 22 which has shown four combined strands (two gracilis strands and two semitendinosus strands); maximum load was 4090 ± 295 N/mm and stiffness was 776 ± 204 N/mm, which were much stronger and stiffer than two semitendinosus strands or two gracilis strands. And harvesting the gracilis in addition to semitendinosus does not appear to affect the graft-related complication. 23 Four combined strands (two gracilis strands and two semitendinosus strands) are significantly stronger to reconstruct the Achilles tendon, and it is different from previous studies which used semitendinosus tendon or gracilis tendon autograft alone. 4,17 –21 Based on these advantages, we used semitendinosus tendon and gracilis tendon autograft to reconstruct Myerson type III CATR.
In our study, after mean follow-up of 31.3 months, all patients returned to daily activity and were able to do a sustained single stance heel raise, and three patients returned to sports. The average score on the VAS for pain was 0 at the last follow-up, and no patients had heel pain. The postoperative mean scores were 97.6 points for the AOFAS score and 92.7 points for the ATRS, both of which were greater than previously reported scores for CATR, which ranged from 87 to 95 points for the AOFAS and 86 to 92.1 points for the ATRS. 8,24 –26 The average SF-36 physical and mental values were significantly improved.
Additionally, the diameter of four combined strands (two gracilis strands and two semitendinosus strands) was 7.8 ± 1.2 mm, 27 approaching to the mean diameter of adults’ Achilles tendon (7 mm). 28 In our study, the size of the involved side’s ankle circumference at 7.5 cm above the calcaneal tuberosity was approximately equal to the contralateral side at the last follow-up (21.8 vs. 21.4 cm). It suggests that our reconstruction method will help to restore the original shape of Achilles tendon. Our suture method (semitendinosus tendon using Kessler suture and gracilis tendon using surround suture) was also beneficial to reshape the Achilles tendon, making it close to the normal anatomy shape of Achilles tendon. We closed the skin using 3-0 STRATAFIX knotless tissue control device. In that way, the incision scar will be very thin and inconspicuous. This suture method can provide a better cosmetic effect and shorter hospital stays (there is no need to remove stitches).
This study had some limitations. First, the sample size is not large enough; there are just seven patients in the study. Under the current medical condition in China, CATR is relatively rare. Second, only a 31.3-month clinical follow-up was performed. A longer follow-up period would be more valuable for evaluation of potential further complications.
In summary, using semitendinosus tendon combined gracilis tendon autograft to reconstruct Myerson type III CATR is a safe and effective method with less complications and low economic burdens.
Footnotes
Authors’ note
Xian-Jun Jiang and Jian-Jian Shen are co-first authors.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.