
Abstract
Objectives:
Earlier reports describe forearm flexor muscles as active stabilizers of the elbow to valgus stress during throwing motion. Given high school pitchers’ history of elbow symptoms, this study assesses its relation to elbow valgus joint instability and forearm flexor muscle strength.
Methods:
Ultrasound examination was made for 132 high school baseball pitchers with and without valgus stress of the medial aspect of the bilateral elbows. They had completed a self-administered questionnaire related to self-satisfaction score (0–100) for pitching performance and throwing-related elbow joint pain sustained during the prior year. Using a digital manual muscle strength meter, we examined the grip strength and muscle strength of the flexor carpi ulnaris (FCU). For participants with and without a history of elbow symptom, we compared differences of ulnohumeral joint space width with and without valgus stress and grip and FCU muscle strength.
Results:
For ulnohumeral joint width difference with and without valgus stress, pitchers with an elbow symptom and those without elbow symptom history on the throwing side were not significantly different. No difference was found in the grip strength or FCU muscle strength of the throwing side for each group. Positive significant association was found between FCU muscle strength on the pitching side and the self-evaluation score for pitching performance (r = 0.27, p = 0.002). However, no association was found between the elbow valgus instability and the forearm flexor muscle strength.
Conclusion:
FCU muscle strength might influence high school baseball pitching performance.
Keywords
Introduction
The ulnar collateral ligament (UCL) is the primary stabilizer of elbow joint to valgus stress. 1,2 Tremendous repetitive valgus stress to the elbow often injures a UCL, especially during the late cocking and acceleration phases of throwing. 3 These valgus torques can be as high as 120 Nm during pitching phases in the elbow during baseball pitches. 4 Active constraints of the flexor–pronator muscles contribute to the dynamic valgus stability at the elbow. 5 –12 Earlier anatomical studies have demonstrated that flexor–pronator muscles and the common tendon assist the anterior bundle of the UCL by sharing static and dynamic forces related to the medial elbow joint. 5 An electromyographic study has shown that pitchers with symptomatic valgus instability have decreased flexor–pronator muscle activity during pitching motion. 8 The flexor–pronator muscle dysfunction and static muscle strength weakness might be associated with clinical symptoms of instability and pain in baseball pitchers experiencing repetitive elbow valgus stress. Nevertheless, no report of the relevant literature has described the relation between prior subjective elbow symptom in baseball pitchers and either flexor muscle static strength or elbow valgus instability. This study used stress ultrasonography (US) technique to evaluate the association between prior subjective elbow symptoms and elbow joint instability of the throwing side and each of static grip strength and flexor carpi ulnaris (FCU) muscle strength. 13,14 This study also elucidated correlation between the self-satisfaction scores of pitching performance in high school pitchers and each of the degree of static flexor muscle strength and elbow joint instability of the throwing side.
Materials and methods
This retrospective case-control study of high school pitchers was designed to use US to elucidate the relation between UCL instability and the strength of grip and FCU and elbow pain history. To assess the pitchers’ physical condition during the winter off-season, we examined 132 local high school baseball pitchers aged 15–17 years (mean 16.5 years, all male). The participants, who had played baseball for an average of 8.18 years (range 2–12 years), underwent physical examination of bilateral elbows. Each participant also completed a self-administered questionnaire with items related to the throwing side, years of playing baseball, and history of throwing-related elbow joint pain sustained during the calendar year preceding the questionnaire. Each marked his self-satisfaction score for throwing. The score reflects his ball control, ball speed, and throwing condition. Elbow joint pain was defined for this study as a condition caused directly by throwing and resulting in participation loss. Elbow measurements were recorded during winter-training medical check-ups (in preseason). The elbow range of motion (ROM) was measured by the participant in a seated position. The shoulder was elevated 90° with the elbow in full extension and flexion, with the wrist in full supination. The fulcrum of the goniometer was placed over the lateral epicondyle of the humerus. We positioned one arm of the device in the center of the humerus to the tip of the acromion process and the other arm in the center of the radius to the radial styloid process. We earlier established the intra-rater validity and reliability of the goniometer. 15
Grip strength test
A digital dynamometer (Takei Scientific Instruments Co., Tokyo, Japan) was used to measure the grip strength. Grip testing was done using a standardized position recommended by the American Society of Hand Therapists. Each participant was seated with the shoulder in adduction and neutral rotation, elbow flexed at 90°, forearm in a neutral position, with the wrist between 0° and 30° of extension and 0° and 15° of ulnar deviation.
FCU muscle strength measurement
A digital handheld dynamometer (Hoggan Health Industries Inc., Salt Lake City, Utah, USA) was used to measure FCU strength. Each participant was seated with the supinated hand in the extended position. The practitioner pressed against the hypothenar eminences in the direction of flattening the hand and against the hand in the direction of wrist extension. Then the participant was requested to abduct the little finger strongly against the practitioner of resistance. 16
Ultrasonographic technique
With participants in a supine position, we performed US of the elbow, scanning the elbow at 30° of flexion. Gravity stress was applied to the forearm straining the UCL. We obtained images of UCLs with and without gravity stress on the bilateral side each time. US imaging was conducted using a multifrequency 12 MHz linear-array transducer (LOGIQe; GE Healthcare, Chicago, Illinois, USA). We used conventional 30° elbow flexion for US evaluation of the anterior band of the UCL by easy and verifiable gravity valgus stress method. An orthopedic surgeon with 15 years of experience in musculoskeletal US, who was blinded to other items in the evaluation, performed the evaluation. Using electronic calipers, the ulnohumeral joint width at the level of the anterior band was measured without gravity valgus stress on the bilateral side (Figure 1). We defined the ulnohumeral joint space as the distance from the edge of the trochlea of the humerus to the edge of the coronoid process of the ulna. The difference between the width of the ulnohumeral joint with and without valgus stress on the bilateral side was calculated. We earlier established the intra-rater validity and reliability of measuring the ulnohumeral joint space using electronic calipers. 17

The ulnohumeral joint width at the level of the anterior band with and without valgus stress on the bilateral side was measured. The ulnohumeral joint space as the distance from the edge of trochlea of the humerus to the edge of the coronoid process of the ulna was defined. MFH: medial epicondyle of the humerus; TH: trochlea of the humerus; CU: coronoid process of the ulna; CFT: common flexor tendon.
After data collection was completed, we classified participants according to their history of elbow pain: 60 reported a history of elbow pain and 72 reported no history of elbow pain. We compared the bilateral ROM of extension and flexion and forearm muscle strength and the width of ulnohumeral joint space with and without gravity valgus stress of the bilateral side. In addition, we compared the self-satisfaction score for pitching performance between the two groups and each of bilateral difference between the width of ulnohumeral joint with and without valgus stress. All participants and their parents gave informed consent to participation in this study, which was approved by our institutional review board.
Statistical analysis
Data of the dominant and nondominant sides were compared using paired t-tests. Groups (the elbow pain group and the no elbow pain group) were compared using either the Mann–Whitney U test or an independent t-test for continuous variables: grip strength, FCU muscle strength, and the difference between the width of the ulnohumeral joint with and without valgus stress in the throwing side and pitching assessment score. Spearman rank correlation coefficients were used to elucidate the relation between years of playing baseball and grip strength and FCU muscle strength and the difference between the width of the ulnohumeral joint with and without valgus stress in the throwing side and the pitching performance score. Data are presented as means and standard deviations (SDs): p values <0.05 were inferred as statistically significant.
Results
For all participants, the dominant side exhibited significantly smaller ROM of elbow extension and flexion than the nondominant side. The dominant side FCU strength was greater than that of the nondominant side. The dominant side of all participants exhibited significantly greater width of the ulnohumeral joint space with gravity valgus stress and greater difference between the ulnohumeral joint width with and without valgus stress (Table 1). Results of intergroup comparison (elbow pain vs. no elbow pain) are presented in Table 2.
Forearm flexor muscle strength and elbow US findings related with dominant and nondominant side in all participants.a

US: ultrasound.
aValues are represented as means ± standard deviations.
bStatistically significant: p < 0.05.
Physical characteristics of participants with and without elbow pain.a
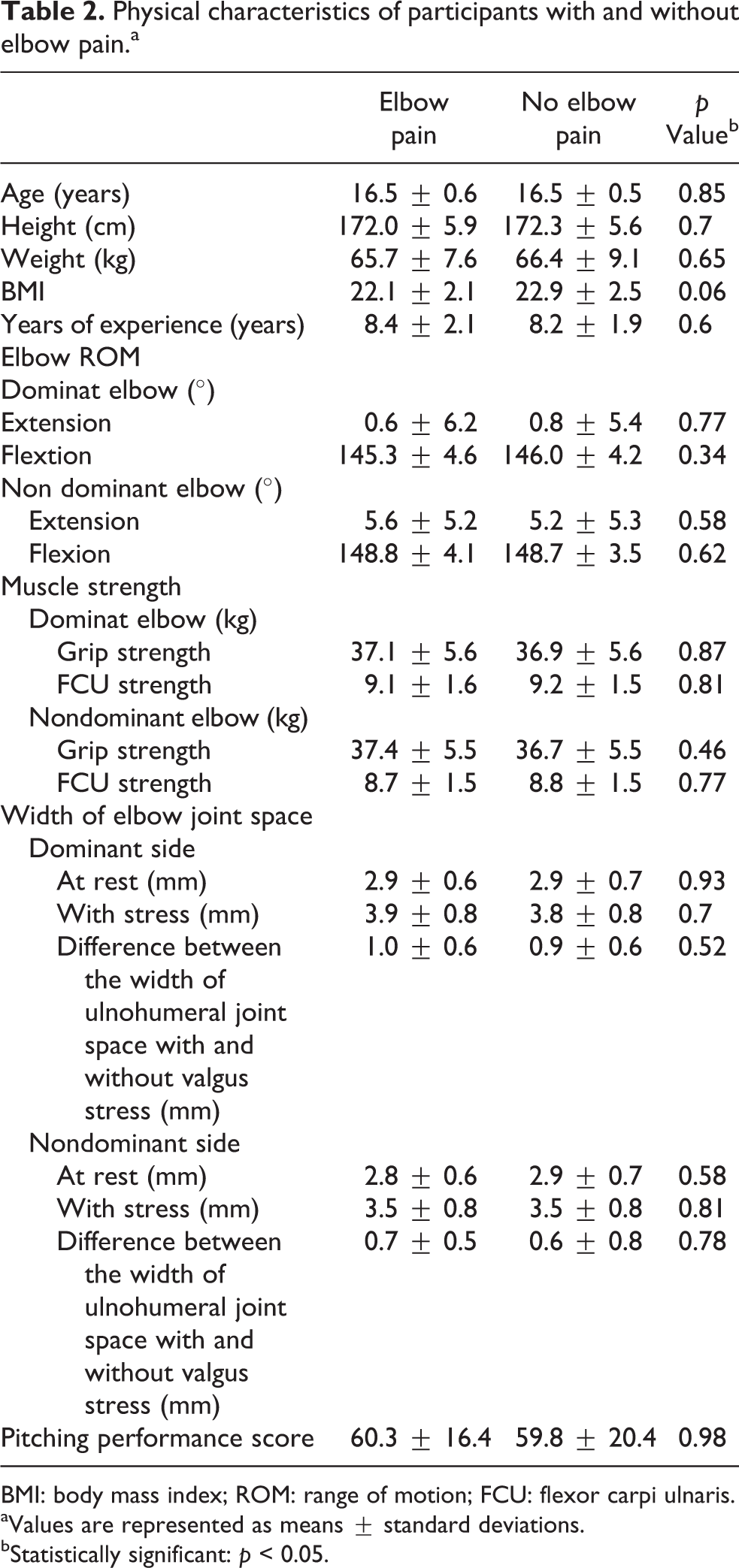
BMI: body mass index; ROM: range of motion; FCU: flexor carpi ulnaris.
aValues are represented as means ± standard deviations.
bStatistically significant: p < 0.05.
No difference between ulnohumeral joint width with and without valgus stress was found between pitchers with an elbow symptom and those with no elbow symptom history on the throwing side. Moreover, no difference was found in the grip strength and the FCU muscle strength of the throwing side for each group.
For all participants, positive association was found between FCU muscle strength and the self-satisfaction score for throwing (p = 0.0018, r = 0.27) and grip strength (p = 0.0032, r = 0.25). Positive significant association was found between the baseball playing career duration and grip strength (p = 0.023, r = 0.20). However, no association was found between the baseball playing career duration and FCU muscle strength (p = 0.31, r = 0.09; Table 3)
Correlation between the duration of playing baseball and pitching performance score and forearm muscle strengths and the degree of valgus elbow instability in the dominant side.

*p < 0.05: statistically significant.
† p < 0.01: statistically significant.
Discussion
The anterior band of the UCL is the primary elbow stabilizer of valgus stress during pitching motion. 1,2 The flexor–pronator muscles were put forward as secondary valgus support. 5 –12 From results of electromyographic analysis, Digiovine et al. reported that flexor–pronator muscles demonstrated high activity during the acceleration phase in uninjured and skilled pitchers who were playing at the college or professional level. 6 This result suggests that flexor–pronator muscles added a dynamic component to elbow stability. We evaluated the static flexor digitorum superficialis (FDS) and FCU muscle strength as the assessment of muscle function and investigated the degree of the medial elbow valgus instability by dynamic valgus stress US method in high school baseball pitchers. Moreover, we classified participants according to their history of elbow pain or lack thereof in the year immediately preceding the date of the questionnaire survey (the elbow pain group and the no elbow pain group) and compared to the grip strength and FCU muscle strength and the degree of medial elbow valgus instability on the throwing side. Our earlier study revealed an association with the elbow valgus instability and the subjective elbow pain in high school baseball pitchers. 18 We hypothesized that the grip strength and FCU strength of the pitchers with elbow pain in the past might be less than those of the pitchers without past elbow pain.
Our study found no differences in grip strength or FCU muscle strength and the degree of the medial elbow valgus instability among the two groups. We did not assess the forearm flexor muscle strength during the pitching motion of each pitcher. It is apparently reasonable to measure the quantitative value of flexor–pronator muscle strength during the dynamic pitching motion. However, we measured grip strength and FCU muscle strength in a static position. These points might influence our results.
An earlier report of a biomechanical study described that FDS contributed most to valgus torque compared to the FCU and pronator teres (PT). In a cadaveric study, An et al. investigated the potential moment contribution of each muscle at the elbow joint, as estimated by multiplying the moment arm (cm) of the muscle by its physiological cross-sectional area (cm2). 19 They demonstrated that the potential moment contribution to flexion–extension and varus–valgus rotation of the FDS provided the greatest in the elbow extended and flexed position with neutral forearm rotation. In biomechanical models of the cadaveric elbow simulated under three conditions of the UCL (intact, stretched, cut), Udall et al. investigated the relative contribution of flexor–pronator muscles to valgus stability of the elbow. Their results demonstrated that the FDS was the major muscular contributor among the FCU and pronator teres. 11 To assess the FDS muscle function, we measured the grip strength, which is generated through FDS and flexor digitorum profundus and intrinsic muscle actuation. The study results demonstrated that no difference exists in the grip strength of the throwing side between pitchers with an elbow symptom history and those with no elbow symptom history. Moreover, no association was found between the value of grip strength and difference between the width of ulnohumeral joint space with and without valgus stress on the throwing side. These results might be reflected by not-isolated FDS muscle strength measurements. A cadaveric and anatomical study by Davidson et al. revealed that the FCU was optimally positioned directly over the medial collateral ligament at 30°, 90°, and 120° of elbow flexion with the FDS, in an adjuvant location, with specific muscles best suited to provide medial elbow support. 20 Park et al. investigated the contribution of the flexor–pronator mass to valgus stability in UCL-deficient elbows of cadavers. 10,13 They loaded the FCU, FDS, and pronator teres with 15 N and found that FCU provided the greatest reduction of the valgus angle. We measured the static FCU strength and assessed the degree of valgus instability in high school baseball pitchers. Results show no difference in the FCU muscle strength of the throwing side between pitchers with an elbow symptom and those with no elbow symptom history on the throwing side. Moreover, no association was found between the value of FCU strength and difference between the width of ulnohumeral joint space with and without valgus stress in dominant side. However, the FCU muscle strength was positively associated with the self-satisfaction score for their throwing. This finding might be related with the results of studies reported by Davidson et al. and Park et al. The greater FCU muscle strength might stabilize more valgus torque during the pitching motion.
A few reports have described in vivo investigations of the contributions of flexor–pronator muscle contractions. 21,22 Otoshi et al. investigated 12 healthy adult men to ascertain whether active contraction of flexor–pronator muscles stabilizes the medial elbow joint against manual valgus load. That study measured the medial elbow joint space using US. The results demonstrated that pronator teres and flexor carpi radialis function as dynamic stabilizers against valgus load more than either FDS or FCU. 21
Pexa et al. used US to examine 22 elbows of healthy men, evaluating the contribution of the flexor–pronator muscle contractions to valgus elbow stability. They measured the medial elbow joint space at rest, under valgus stress, and under valgus stress with finger and forearm flexor contraction. They reported that wrist and finger flexor muscle contraction decreased the medial elbow joint space under a valgus load. 22 However, the subjects of their studies were not baseball players, but healthy volunteers. Further studies must be conducted to assess the action as the stabilizer against the elbow valgus load during baseball players’ pitching motion.
Our study has several limitations. First, this study was cross-sectional. Second, we defined the elbow symptoms of participants as a condition caused directly by throwing and which caused participation loss during the year preceding this study. Nevertheless, we did not specify the terms of participation loss. Third, the elbow symptom severity was not assessed. Fourth, we were unable to measure the pronator teres muscle strength using a digital handheld dynamometer because of its low reliability and reproducibility. Further studies of baseball pitchers should be undertaken to assess the elbow valgus instability and pronator teres muscle strength.
Conclusion
We measured the width of the ulnohumeral joint space with and without gravity stress in 60 high school pitchers with a history of elbow symptoms and 72 high school pitchers with no history of elbow symptoms. No difference between the width of ulnohumeral joint with and without valgus stress was found between pitchers with an elbow symptom and those with no elbow symptom history on the throwing side. Between groups, no difference was found in either the grip or the FCU muscle strength of the throwing side. Positive significant association was found for all participants between FCU muscle strength on the pitching side and the self-evaluation score for pitching performance. The FCU muscle strength might reflect the prior pitching condition of high school baseball pitchers.
Footnotes
Acknowledgements
For their cooperation and support in this research, we would like to thank the young baseball players, their parents, coaches, and staff members of the regional baseball association.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.