
Abstract
Aim:
To evaluate the outcome of a fibular nail in the treatment of open and closed unstable ankle fractures in a non-designer centre.
Methods:
In a retrospective cohort study, a total of 39 ankle fractures (14 open and 25 closed) treated with a locking fibular nail were evaluated between 2012 and 2015 in a non-designer level I major trauma centre. Post-operative radiographs were analysed to assess the quality of reduction (McLennan and Ungersma marking system), fracture union and complications. Three patient reported outcome scores (Olerud and Molander score (OMAS), American Association of Orthopaedic Surgeons (AAOS) foot and ankle score and 12-Item Short Form Survey (SF-12)) were collected to obtain an overall measure of the patient’s physical and mental outcome.
Results:
The adequacy of reduction data was available for 38 of 39 cases; 33 (87%) achieved good, 3 (8%) fair and 2 (5%) poor ratings, based on the McLennan and Ungersma marking system. Thirty-five (12 open and 23 closed) patients were available for initial follow-up. Five (14.3%) of 35 had documented complications (2 of 12 in the open cohort and 3 of 23 in the closed cohort). All fibular fractures treated with the fibular nail went on to unite. Twenty-three (66%) of 35 patients were available at 1-year follow-up for measurement of objective outcome. The combined mean OMAS for both groups was 53.7 (0–85) with statistically better results (59.5 (25–85) vs. 37.3 (0–75)) in favour of the closed versus open injuries, respectively. The mean AAOS score was also statistically better for the closed group than the open, 70.3 (30–95) versus 46.6 (20–77), respectively. The mean SF-12 score (physical component) was 40 (21.6–52.4) in the closed group versus 36.1 (19.4–51.5) in the open group; the mean mental component was 42.5 (26.6–54.3) in the closed group versus 38.8 (28.4–60.5) in the open group, these however were not statistically different.
Conclusion:
Fibular nails are an effective alternative for the treatment for both closed and open unstable ankle fractures with soft tissue compromise.
Introduction
Ankle fractures account for approximately 10% of all fractures in the human skeleton. 1 –3 They are the third most common adult fracture presenting to the emergency department with incidence reported to be as high as 187 per 100,000 people per year. 3,4 Epidemiological studies report a bimodal distribution, with high-energy injuries in the young and low-energy fragility injuries in the elderly. 3,5,6 Consequently, both bring a challenge with the management of the soft tissue envelope, as the young are associated with an overlying direct high-energy trauma 5 and the elderly have comorbidities such as malnutrition, obesity, diabetes and vascular disease. 7
Ankle fractures that require fixation are most often managed using AO principles of open reduction and internal fixation (ORIF) with lag screw and neutralization plate 8 or bridging plate in the case of multifragmentary fractures. Recently, more modern technologies such as locking plates have been utilized for the increasing number of fragility fractures which have osteoporotic bone with comminution. 9 Despite having strong theoretical background, both fixation techniques have a complication rate of up to 30% 10 with wound complications being the most common, which is attributed to a long incision (>8 cm) and dissection often required in an already injured area with limited soft tissue cover. Furthermore, industrialization and urbanization have led to a steady number of open ankle fractures which generally have a large zone of injury that requires plastic surgery coverage. 11 While antibiotics and soft tissue grafts have improved outcomes, the morbidity is still high. 12
The locking fibular nail has come as an attractive option as it requires smaller incisions (1 cm), less soft tissue dissection and reduces the second hit to the bone biology which in theory would overcome the complication profile seen previously. It could also potentially avoid the symptoms of prominent metal work, which has been reported as high as 50% in some series with extra-medullary fixation. 13 Its philosophy relies on achieving approximate reduction with appropriate length and rotation unlike traditional ORIF with anatomical reduction. Designer centres have reported good radiological and functional outcomes with minimal complications in closed fractures even when compared to traditional ORIF. 14,15 However, it is well recognized that designer centres of implants have enjoyed better than normal results, which may not be representative of the wider surgical community. The role of fibular nails in open ankle fracture fixation has not been made clear and is of interest if it can have a positive impact on an injury which already has a less than satisfactory outcome.
The aim of this study was to (1) evaluate the use of fibular nails for open ankle fractures and (2) compare those results against closed unstable ankle fractures in a non-designer level I major trauma centre setting. The null hypothesis was that no clinical advantage compared to ORIF historically would be seen.
Patient and methods
A retrospective analysis was conducted on patients who had sustained an ankle fracture that was treated with the Acumed Fibula Rod System (FRS; Hillsboro, Oregon, USA) during the period from March 2012 to February 2015. The study was conducted in the setting of a level I major trauma centre that treats open and closed ankle fractures routinely. The decision to treat patients with the FRS was made by the consultants at the trauma meeting on the day of surgery. They were treated solely or combined with other methods of fixation. There were no mandated indications, other than surgeon discretion.
Patient electronic notes were examined for demographical data, medical comorbidities and occurrence of complications.
Preoperative imaging studies were reviewed to assess the fracture configuration. Danis–Weber classification 16,17 was used including the total number of malleoli involved. Following fixation, post-operative plain radiographs were reviewed to assess fixation type, quality of reduction, fixation complications and fracture union. Anatomical markers were used to define reduction success using a previously published measuring system by McLennan and Ungersma. 18 All imaging results were interpreted by the senior surgeon. A good reduction was defined as the fibula being out to normal ankle length, <2 mm posterior displacement and <1 mm increase in medial clear space. A fair reduction was defined as fibular shortening of <2 mm, 2- to 4-mm posterior displacement and 2-mm medial clear space widening. A poor reduction was defined as fibular shortening >2 mm, >4 mm posterior displacement and >3 mm medial joint space widening.
The Gustillo–Anderson classification was used intra-operatively to categorize open fractures based on the extent of soft tissue injury. 19
Surgical technique
Fluoroscopic guidance was used throughout surgery in all cases. Patient was positioned supine with sandbag underneath the ipsilateral buttock to achieve adequate internal rotation of the affected lower limb. After fracture reduction with appropriate traction manoeuvres, a 1-cm incision was made distal to the tip of the fibula. A 1.6-mm guide wire was inserted to guide the entry point in the distal fragment of the lateral malleolus. In case of failed traction manoeuvres for reduction, percutaneous incisions were made to allow a small pointed forceps clamp to achieve adequate reduction. Fluoroscopy was then used to confirm the correct entry point, ensuring the guide wire was marginally medial to the apex to avoid lateral wall blowout and was central at the tip of the fibula in the lateral view. A 6.1-mm cannulated reamer on a drill was subsequently used to prepare the distal metaphyseal canal over the guide wire. Serial reaming was then used for the proximal diaphyseal canal using 3.1-mm or 3.7-mm hand reamers. The nail was then assembled on its jig and inserted through the prepared canal keeping the ankle in a mild external rotation to allow a subsequent internal rotation manoeuvre to reduce fracture before locking. Despite availability of multiple lengths of the nail, the 110-mm nail was used in all cases with either a 3.1-mm or 3.7-mm diameter. Stab incisions were used to insert the two anteroposterior (AP) locking screws distally. Lateral view fluoroscopic images were obtained during AP locking to ensure the correct length of the distal screws, to prevent peroneal tendon irritation. The fibular length was then restored using traction, and slight internal rotation was provided on the jig to allow the fracture to reduce into position. One or two syndesmotic screws were then inserted, depending on the level at which the distal syndesmotic screw hole was positioned, to ensure axial and rotational stability of the construct. If the distal syndesmotic screw hole was at or below the level of the joint, then only the proximal screw was inserted, otherwise both screws were used, once again using stab incisions. The procedures were performed by either a consultant or a trainee under direct supervision by a consultant. Posterior and medial malleolar fractures were treated under the surgeon’s discretion.
Patient reported outcome measures
Three validated outcome scores were collected to give a broad overview of the patient’s physical and mental function. The Olerud and Molander score (OMAS) is a functional rating score, out of 100, comprising nine parameters. A score of 100 represents a normal ankle with 0 being the worst and representing a painful, stiff and dysfunctional ankle with severe disability.
20
The 12-Item Short Form Survey (SF-12) is a validated outcome tool to assess a patient’s view on health. It assesses the physical and mental components of a patient’s chronic condition compared to the general population.
21
A mean score for the British population is 50. The American Association of Orthopaedic Surgeons (AAOS) foot and ankle score is a 25-item survey which measures functional and footwear activity. It is a computer-generated percentage, the best being 100 and the worst 0.
22
Ethical statement
Ethical approval was not sought nor required as it was part of a service evaluation project for the Trauma and Orthopaedic Department.
Statistical analysis
Normality was assessed using the Shapiro–Wilk test so for continuous, parametric variables between the ankle patient reported outcome measures (PROMs), an independent two-tailed t test was applied. A significance level of α = 0.05 was employed.
Results
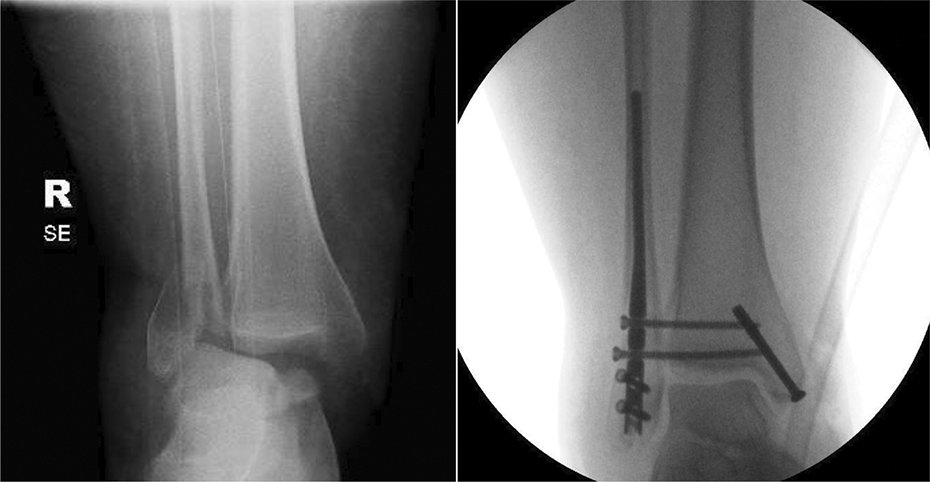
During the 3-year study period, a total of 39 patients with ankle fractures (open = 14 and closed = 25) had fixation with the FRS. Of the 14 open fractures (Table 1), the majority (n = 8) were a Gustillo type 2, followed by type 3a/b (n = 5) and type 1 (n = 1). The wounds for all of the open injuries were on the medial side. The most common fracture configuration for both open (Figure 1) and closed patients (Figure 2) was a bimalleolar (medial and lateral malleolus) fracture which accounted for 69% of cases (Table 2). According to the Weber classification, 31 cases had a type B and 8 had a type C fracture.
Gustillo and Anderson open fracture classification system.


Open ankle fracture with a medial tear with significant displacement that had fixation with a fibular nail.
A closed unstable ankle fracture in an obese patient that had FRS fixation.
Fracture type.

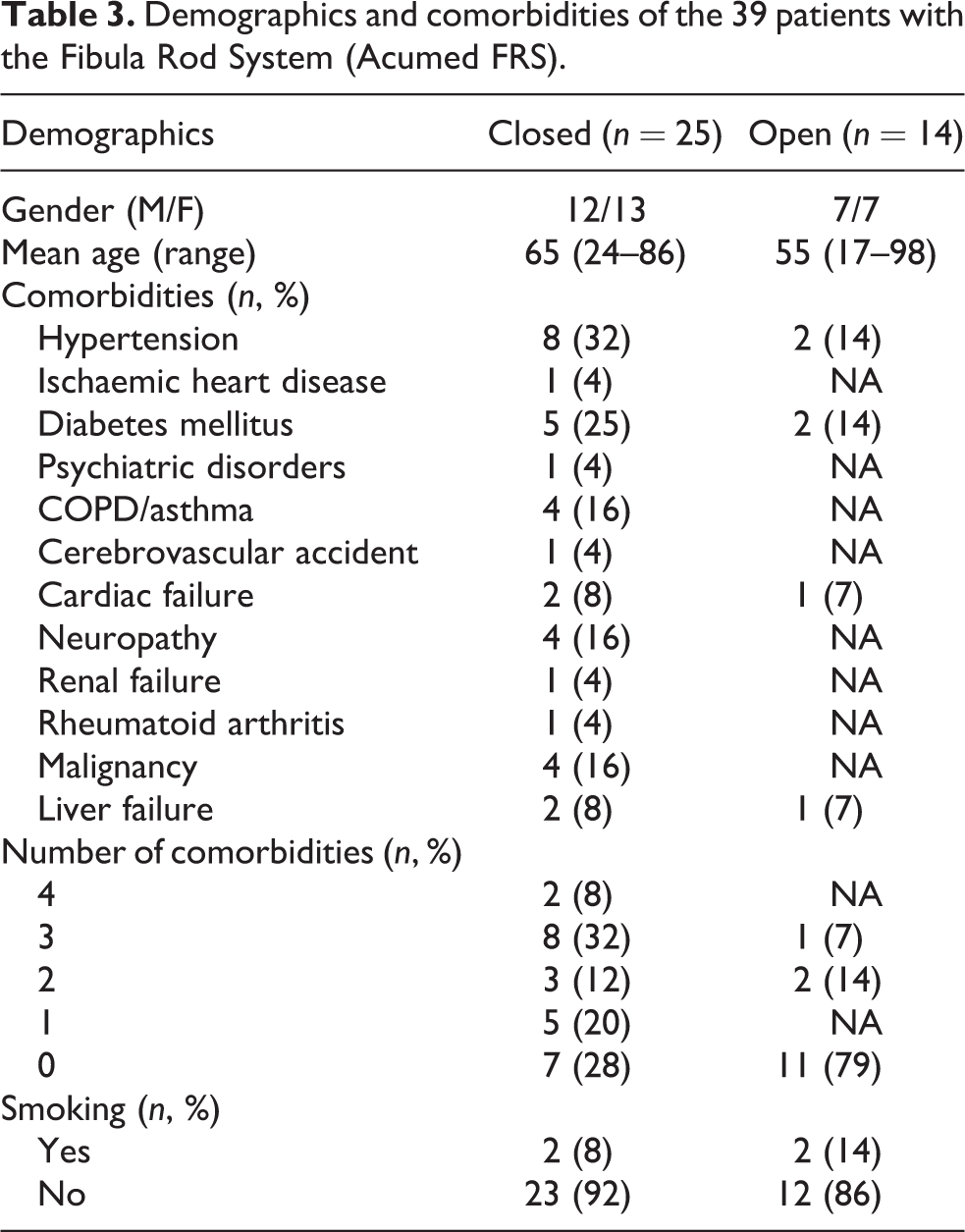
The mean age of all patients was 62 years (range 17–98) with near identical distribution for gender, 19 males and 20 females, respectively (Table 3). The mean age for open fractures was younger (55 years) than the closed fractures (65 years). In total, 78% of the open cohort patients had no significant past medical history, while the closed cohort patients had only 28%. Additionally, the closed group had on average two comorbidities, with 32% having three comorbidities. The median date to operation was 4 days, with the mean being on day 6.
Demographics and comorbidities of the 39 patients with the Fibula Rod System (Acumed FRS).
The most common additional fixation method was partially threaded cancellous screws for an associated medial malleolus fracture which used a mini-incision open technique to remove soft tissue interposition on closed injuries. The open ankle fractures by mechanism all had an open wound window for fixation after debridement. There were two posterior malleolar fractures that utilized a closed technique using anteroposterior screws. The adequacy of reduction from departmental post-operative plain radiographs were available for 38 cases, 33 (87%) achieved good, 3 (8%) fair and 2 (5%) poor, based on the McLennan and Ungersma marking system.
In total, four cases were lost to follow-up as three had travelled abroad and one open fracture patient succumbed to another life-threatening injury soon after surgery. Of the available 35 patients who had regular outpatient clinic follow-up, 12 had an open injury and 23 had a closed injury. The mean hospital follow-up period from operation to last clinical encounter for discharge was 4.1 months (1.5–16.0 months).
Of the cohort, five patients had documented complications. One fibular nail in the open fracture cohort was removed 6 weeks after the index procedure due to a persistent lateral wound infection. There was one case of medial joint space widening for a poor reduction in the closed cohort which required syndesmosis fixation revision (Figure 3). There were three cases of medial malleolar non-unions, one in the closed fracture cohort and two for the open cohort, respectively. One non-union was seen in an open ankle fracture which required formal washout and antibiotics for septic arthritis from the medial wound. The patient consequently also developed ankle osteoarthritis. The final two medial malleolar non-unions were treated conservatively as they were asymptomatic. All remaining fractures went on to unite.

Poor reduction with resultant medial joint space widening and diastasis.
Patient reported outcome measures
Of the 35 patients who had regular follow-up after fixation, only 23 (66%) were contactable at 1 year for psychometric analysis. The mean scores are presented in Table 4 for both open and closed fractures. The overall mean OMAS was 54 (range 0–85). The mean score of the open ankle cohort was statistically worse (p = 0.04) than the closed cohort, 37 versus 60, respectively. The mean AAOS ankle score was 64 (range 20–95), with again a statistically (p = 0.02) worse outcome for the open fractures compared to the closed fracture group (70 vs. 47). SF-12 physical component had a mean score of 39 (range 19–52), while the mean mental component score was 42 (range 27–61) with lower scores found in both for the open cohort but this did not reach statistical significance. As predicted, the outcome scores were worse for the open injuries as the majority by mechanism had an element of articular damage and other life- or limb-threatening conditions.
Patient reported outcome measures.

OMAS: Olerud and Molander ankle score; AAOS: American Association of Orthopaedic Surgeons.
aSignificant difference between open and closed ankle groups (p < 0.05).
Discussion
The use of modern fibular locking nails for unstable ankle fractures is gaining popularity due to its load sharing and rotationally stable properties. 23 –26 In the past decade, there is a growing body of evidence to support its use, particularly in elderly patients who have a compromised soft tissue envelope that may be at risk with traditional fixation. 26 –29 This study reviewed the outcome following ankle fracture treatment with the FRS in a non-designer level I major trauma setting. Of interest, we wanted to determine its role specifically in open fractures.
In our small series, we found that a high proportion (18 of 39) of patients having this type of fixation were greater than 65years. In fact, there were seven patients over our national life expectancy age of 81years and only seven patients younger than 50 years. The great majority of patients having the FRS in the closed cohort had multiple comorbidities and were of low demand, which may be a factor for the implant choice with a conceded flaw of approximate reduction. The open fracture cohort conversely was generally healthy people with significant soft tissue compromise. Irrespective of age and cohort, the FRS was able to achieve a good reduction in 87% of fibular fracture cases which is not as good as the designer centre which achieved 96%. 14 Despite not achieving anatomical reduction, we found that all fibular fractures united after having the FRS which is in accordance with other similar studies. 14,28,29 Furthermore, our complication rate was low with the majority stemming from open fractures that affected the medial malleolus. The 3% wound complication rate found from one lateral wound infection is consistent with previous studies and more favourable than lateral plating techniques. 27,28
Yet, the most encouraging finding in this study was its results for open fractures. Despite having two complications requiring two reoperations, its resultant 17% complication rate is similar or better than recent articles investigating open fractures treated with ORIF or external fixation. 12,30 Furthermore, a small case series of four patients found similar success using the same device which gives an unproven but promising trend for its use for open fractures. 26
Our PROMs, on the contrary, did not fare as well as the initial retrospective designer study, 14 with our results 10–15% worse. However, the most recent randomized prospective study from the designer centre found that the FRS achieved an OMAS score of 62.5 versus 58.9 in the ORIF group. 15 This is similar to our closed ankle fracture result which was 59.5, which suggests that there may be generalizability in the more recent and better evidence level 1 study. Furthermore, the low complication rate for the fibular nail in our study and the previous studies as compared to the ORIF demonstrates the advantage of using a minimally invasive technique, particularly in the elderly with multiple comorbidities and in cases with compromised soft tissue. The fundamental limitation of this study is the retrospective design, which has documented intrinsic deficiencies which can lend itself to bias. Incomplete follow-up was our biggest problem, as evidenced by the 67% response rate on the PROMs partly inevitable due to the elderly patient group and the transient visiting population of London. Also there is no long-term clinical follow-up beyond 16 months to examine the risk of additional surgeries for problematic metalwork, particularly as hardware irritation has been cited to be as high as 50% for ORIF. Lastly, given the limited available literature on open ankle fracture outcomes, it is difficult to compare our results to other series or forms of fixation to give a recommendation so caution must be taken with these results.
In conclusion, ankle fracture fixation with a locking intra-medullary fibular nail appears to be a safe and effective treatment option in both closed and open fracture settings including elderly patients with comorbidities and poor soft tissues. It gives a predictably low complication rate, even with devastating open injuries. This method of fixation should be considered in patients who have compromised soft tissue that would benefit with closed reduction techniques. Its use in open fractures should be considered, but further prospective investigations with larger numbers should prove its place before routine use can be recommended in clinical practice.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.