
Abstract
Background:
A gold standard procedure has not been established for recurrent patellar dislocation because of multifactorial etiologies. We have been performing crosse de hockey procedure, which is a combination of medial and anterior transfer of the tibial tuberosity, in our institution since 1993. This study aimed to investigate the long-term clinical results of this procedure.
Materials and Methods:
A total of 19 patients (21 knees) underwent the crosse de hockey procedure for recurrent patellar dislocation. Of these patients, four were lost to follow-up. The remaining 17 knees in 15 patients (5 male and 10 female) were included in this study. The mean follow-up period was 13.2 years (range: 5–22.6 years). Clinical evaluation was performed using the Kujala score. Radiographic indicators, such as modified Insall–Salvati ratio, sulcus angle, congruence angle, tilting angle, lateral shift ratio, and the progression of patellofemoral osteoarthritis (OA), were measured.
Results:
Positive apprehension sign and redislocation were not observed in any of the patients. The mean Kujala score was significantly improved from 36.5 ± 18.0 preoperatively to 92.6 ± 9.9 at the final follow-up. Definite OA (a grade 2 or more using the Iwano grading system) was not observed in the patellofemoral joint at the final follow-up.
Conclusions:
The crosse de hockey procedure showed satisfactory long-term clinical results for recurrent patellar dislocation. This procedure could prevent the progression of patellofemoral OA because of the unloading effect of the patellofemoral joint by anteromedial transfer of the tibial tuberosity.
Keywords
Introduction
Recurrent patellar dislocation possesses multifactorial etiologies. 1,2 Patellar stability depends on the limb alignment, the osseous architecture of the patella and the trochlea, the integrity of the soft-tissue constraints, and the interplay of the surrounding muscles. Over the past century, more than 100 different surgical techniques have been proposed. 3 –8 However, the gold standard treatment for recurrent patellar dislocation has not yet been established. 9
We have been performing the crosse de hockey procedure 10 for recurrent patellar dislocations since 1993 in our institution. This distal realignment surgery was introduced by Lord in 1977. The tibial tuberosity is osteotomized in a hockey-stick shape. It is transferred anteromedially to medialize the patellar tendon insertion and to decrease the patellofemoral contact pressure (Figure. 1). The Fulkerson procedure, which is a representative surgery of anteromedial tibial tubercle transfer, has biomechanical superiority as it decreases the patellofemoral contact pressure. 11 This procedure yields satisfactory long-term clinical results. 12 However, to the best of our knowledge, the long-term clinical results of the crosse de hockey procedure have not been reported in English literature. In this study, we aimed to investigate the long-term clinical results of the crosse de hockey procedure for recurrent patellar dislocation. We hypothesized that this procedure shows satisfactory long-term clinical results for recurrent patellar dislocations. Moreover, this procedure could prevent the progression of patellofemoral osteoarthritis (OA) because of the unloading effect on the patellofemoral joint through anteromedial tibial tubercle transfer.
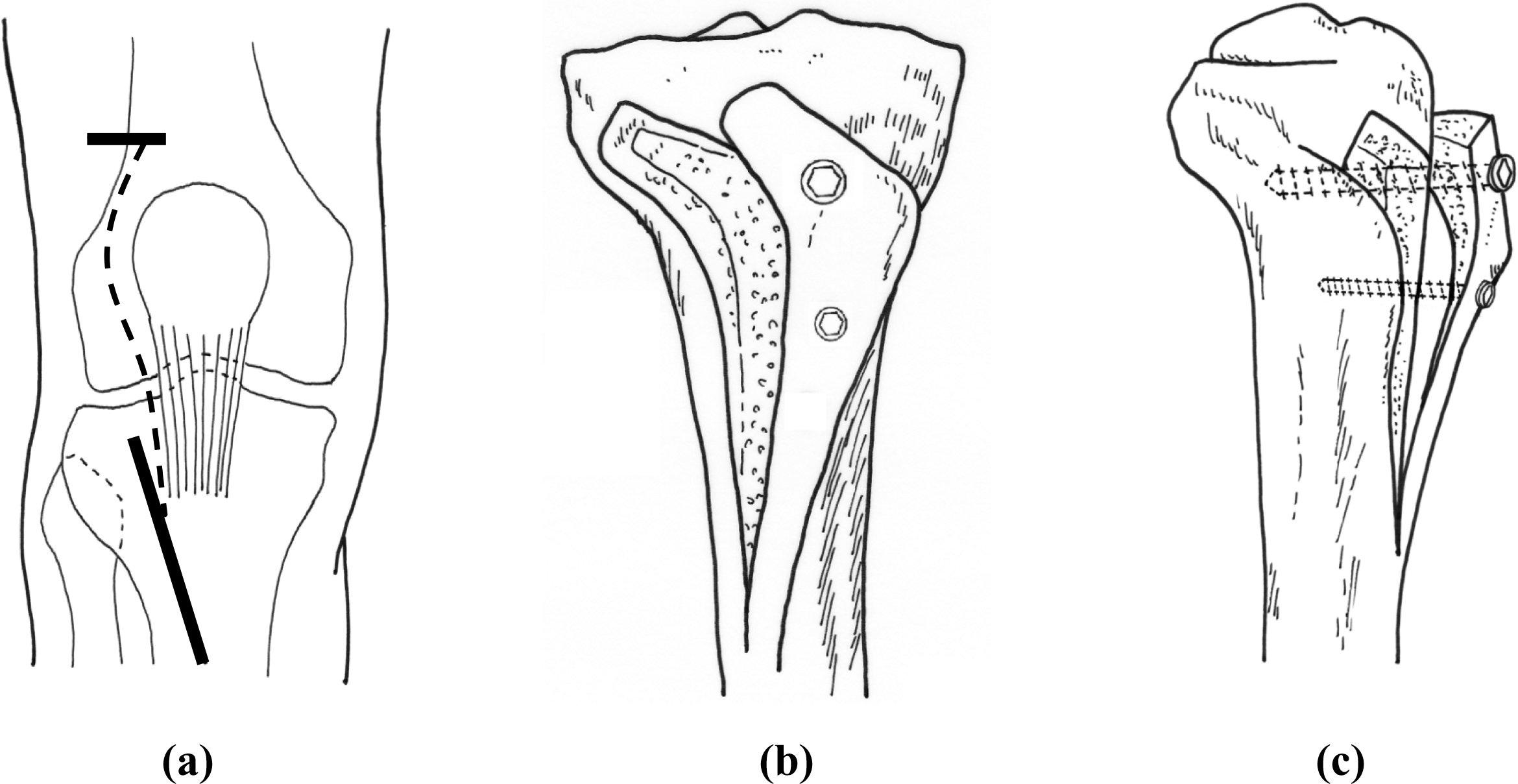
(a) Crosse de hockey procedure. (b) Skin incision of the crosse de hockey procedure. (c) Schematic view of the crosse de hockey procedure.
Materials and methods
Nineteen patients (21 knees) with recurrent patellar dislocation who underwent the crosse de hockey procedure between 1993 and 2012 were enrolled in this retrospective study. Of these patients, four were excluded due to lost to follow-up. The remaining 17 knees in 15 patients (5 male, 10 female) were included in the final analysis. All patients had recurrent patellar dislocation, which is defined as a dislocation occurring more than twice. The mean age at the time of operation was 26.9 ± 9.4 years (range: 15–44 years), and the mean follow-up period was 13.2 0 ±6.8 years (range: 5.0–22.6 years). This study was approved by the Ethics Committee of our institution (IRB No. 2015-27), and informed consent was obtained from all patients.
The criteria for the inclusion of patients for the crosse de hockey procedure were as follows: (1) a history of patellar subluxation or dislocations under low energy more than 2 times; (2) positive apprehension sign; (3) lateral shift and tilt of the patella demonstrated on Merchant axial radiographs; (4) lateral malposition of the tibial tuberosity with more than 15 mm of tibial tuberosity–trochlear groove (TT–TG) distance in CT images; and (5) skeletal maturation with physeal closure of the proximal tibia. Patients with a history of surgery for recurrent patellar dislocation and congenital patellar dislocation were excluded from this study.
All patients were evaluated for range of motion, apprehension test, and the Kujala score 13 preoperatively and at the final follow-up. Radiological examination consisted of the anterior–posterior, lateral, and Merchant axial views. The radiographs were evaluated preoperatively, postoperatively, and at the final follow-up. In the lateral view, the modified Insall–Salvati ratio 14 was used to assess patellar height. In the Merchant’s view, sulcus angle (SA), congruence angle (CA), tilting angle (TA), and lateral shift ratio (LSR) were measured for the congruency of patellofemoral joint. Trochlear evaluation was made according to the criteria defined by Dejour and Le Coultre 4 using preoperative lateral radiograph and CT images. The TT–TG distance was also assessed on preoperative CT images to detect lateral malposition of the tibial tuberosity. Patellofemoral OA was evaluated with the Iwano grading system 15 preoperatively and at the final follow-up to assess the progression of patellofemoral OA. All radiographic measurements were performed twice by a single observer with a 2-week interval between analyses. To ensure accuracy, the intra-observer variance was assessed using paired t-tests, and no significant differences were found (p > 0.05).
Surgical procedure
The patient was placed in the supine position with the knee extended. A 2-cm horizontal skin incision was made on the superolateral side of the patella. After the superior lateral genicular artery was coagulated, subcutaneous lateral release was performed through the skin incision (Figure 1(a)). An oblique skin incision of approximately 8 cm was made on the lateral side of the tibial tuberosity. The tibialis anterior muscle was then partially detached. Subsequently, the tibial tuberosity was osteotomized in a hockey-stick shape using a bone saw, and the osteotomy was extended distally for 7 cm (Figure 2(a)). The thickness of the proximal part was approximately 10–12 mm. The tibial tuberosity was then elevated and mobilized anteromedially, leaving the medial periosteum intact to maintain the blood supply to the osteotomized fragment to enhance bone healing (Figure 2(b)). The proximal part of the osteotomized fragment was laid on the proximal tibia where the periosteum was stripped off. The new location of the tibial tuberosity was determined based on the intraoperative patella tracking tests. The tibial tuberosity was temporarily fixed with a K-wire during the patellar tracking test. The tibial tuberosity was transferred medially to a point where no patellar subluxation was observed. After the new location of the tibial tuberosity was determined, the tibial tuberosity was fixed with a 6.5-mm cancellous screw and one or two 4.0-mm cancellous screws (Figure 2(c)). The osteotomy gap was then filled with β-tricalcium phosphate with 75% porosity (Osferion 75®; Olympus Terumo Biomaterial, Tokyo, Japan) (Figure 2(d)). The mean medialization of the tibial tuberosity in this study was 11.7 ± 2.3 mm (range: 10.0–18.0 mm), and the mean ventralization was 9.8 ± 1.6 mm (range: 8.0–14.0 mm).

Intraoperative images. (a) Osteotomy in the shape of a hockey stick. (b) Anteromedial transfer of the tibial tuberosity. (c) Screw fixation. (d) Artificial bone graft (Osferion®).
Postoperative rehabilitation
The range-of-motion exercise with a continuous passive motion machine and isometric quadriceps exercise were started on the third postoperative day. Partial weight-bearing gait with a knee extension brace was allowed 1 week after surgery, and full weight-bearing gait was permitted after 3 weeks. Running and full sports activities were permitted after 3 and 6 months, respectively.
Statistical analysis
JMP (version 11; SAS Institute Inc., North Carolina, USA) was used to manage and analyze data. The data were presented as the mean and standard deviations. A paired t-test was conducted to analyze differences between preperative and postoperative values. One-way analysis of variance was used to evaluate statistical differences or correlations among the preoperative, postoperative, and final follow-up values. A p value <0.05 was considered statistically significant.
Results
Positive apprehension sign and redislocation were not observed in all patients during the follow-up. The Kujala score significantly improved from 36.5 ± 18.0 preoperatively to 92.6 ± 9.9 at the final follow-up (p < 0.05).
In radiological findings, the modified Insall–Salvati ratio (1.85 ± 0.17 preoperatively, 1.81 ± 0.16 postoperatively, and 1.81 ± 0.17 at the final follow-up) and the SA (143.7 ± 8.8° preoperatively, 142.7 ± 9.4° postoperatively, and 143.7 ± 8.9° at the final follow-up) did not change after surgery (Figure 3(a) and (b)). With regard to the congruency of the patellofemoral joint, all indicators (CA, TA, and LSR) significantly improved after surgery. The mean CA improved from 28.3.5 ± 11.4° to −0.4 ± 13.2°, the TA from 27.7 ± 10.8° to 15.3 ± 4.3°, and the LSR from 39.4 ± 18.5° to 15.8 ± 6.4°. The alignment was maintained at the final follow-up (Figure 3(c) to (e)). Trochlear dysplasia was observed in four cases in our series. The mean preoperative TT–TG was 20.0 ± 2.5 mm (range: 17.0–26.0 mm). According to the Iwano grading system, a slight patellofemoral OA progression was noted from grade 0 to grade 1 in only two knees. The definite OA (a grade 2 or more using the Iwano grading system) was not observed in the patellofemoral joint at the final follow-up (Figure 4).

Radiological results. (a) Modified Insall–Salvati ratio. (b) SA. (c) CA. (d) (TA). (e) LSR. SA: sulcus angle; CA: congruence angle; TA: tilting angle; LSR: lateral shift ratio.

Sample case. A 16-year-old male patient had left patellar dislocation while playing soccer. The crosse de hockey procedure was performed, and osteochondral fragment was fixed with Herbert screws. Twelve years after surgery, patellar alignment was maintained and no patellofemoral osteoarthritis was found. He was able to play soccer without limitation at the final follow-up. (a) and (b) Preoperative radiograph. Osteochondral fragment (black arrow). (c) and (d) Postoperative radiograph. Osteochondral fragment was fixed with Herbert screws. Patella alignment was improved after surgery. (e) and (f) Radiograph at 12 years after surgery. Patella alignment was maintained, and no patellofemoral osteoarthritis was found.
Four knees experienced some discomfort associated with the screws, which were removed in all these cases. The removal of screws resulted in complete disappearance of the symptom. No other surgical complications, such as delayed wound healing, nonunion of the osteotomy site, infection, neurovascular injury, and deep venous thrombosis, were observed.
Discussion
The most important finding of this study was that the crosse de hockey procedure showed satisfactory long-term clinical results for recurrent patellar dislocation. This procedure could prevent the progression of patellofemoral OA because of the unloading effect of the patellofemoral joint by ventralization of the tibial tuberosity.
Recurrent patellar dislocation commonly occurs in patients with various combinations of predisposing factors, such as general joint laxity, a laterally located tibial tubercle, abnormal patellar morphology, femoral trochlear aplasia, and patella alta. 1,2 More than 100 different surgical procedures have been described, and they can be divided into proximal procedures, distal procedures, trochleoplasties, or a combination of these techniques. However, no gold standard treatment for recurrent patellar dislocation exists. 9
With regard to distal realignment, several types of tibial tubercle transfer have been described. The Hauser procedure, which is the medial and distal transfer of the tibial tuberosity, has an advantage of correcting the patellar height. 6 However, this procedure has a high incidence of patellofemoral OA caused by simultaneous posterior transfer. 16 The Elmslie–Trillat procedure is a pure medial transfer of the tibial tubercle. It is a well-established procedure for management of recurrent patellar dislocation. 8,17,18 However, patellofemoral arthritic change develops during long-term follow-up. 19 The Fulkerson procedure is a combination of medial and anterior transfer and has a biomechanical superiority of decreasing the patellofemoral contact pressure. 11 This procedure has achieved satisfactory results in patients with severe patellofemoral OA. 20,21 Tsuda et al. reported that the mean Kujala score was 92.0 at the final follow-up, and no patellofemoral OA progression was found during an average follow-up period of 9.6 years (Table 1). 12 The crosse de hockey procedure is also an anteromedial tibial tubercle transfer, which is the same as the Fulkerson procedure. In the present study, this procedure showed satisfactory long-term clinical results (mean Kujala score: 92.6) and no redislocation occurred. In addition, definite OA (a grade 2 or more using the Iwano grading system) was not observed in the patellofemoral joint at the final follow-up.
Long-term clinical outcomes of other procedures compared with the current study.
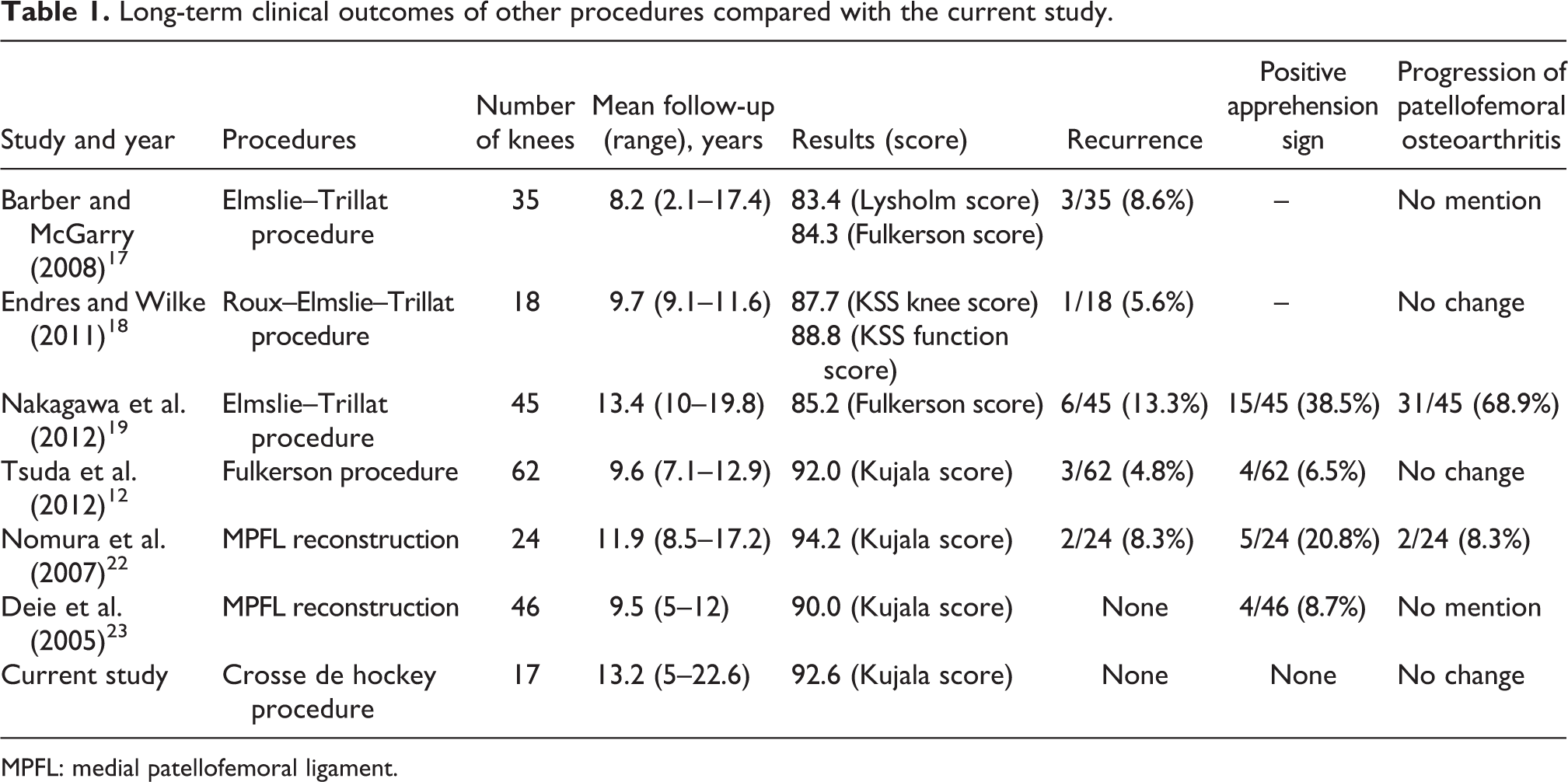
MPFL: medial patellofemoral ligament.
The Fulkerson procedure is a well-established procedure, but some complications, such as nonunion and tibial fractures, have been reported. 24,25 This sliding osteotomy suffers the inability to adjust each of the single planes. In addition, the contact area of the osteotomy site is determined based on the osteotomy angle. The advantage of the crosse de hockey procedure is that it can fine-tune the amount of the medialization and ventralization of the tibial tubercle. Medial transfer of the tibial tubercle is adjusted by the intraoperative patellar tracking test. An anterior transfer is determined by the thickness of the proximal part of the tibial tubercle. In case of large thickness, the volume can be adjusted by trimming. In this study, delayed union or nonunion was not observed in any of the cases. We considered that the proximal contact area of the osteotomy site was sufficient for bone healing in this procedure, and β-TCP, which filled the osteotomy gap, contributed to bone healing.
The anterior transfer of tibial tubercle increases the lever arm of the extensor mechanism and reduces the forces acting across the patellofemoral joint. 26 Biomechanical studies showed that an elevation of 10–15 mm is the optimal advancement to reduce the patellofemoral contact pressures. 27 Overventralization of the tibial tubercle has been reported to have problems with delayed wound healing and nonunion at the osteotomy sites. 28 In the present study, the mean anterior transfer of tibial tubercle was 9.8 ± 1.6 mm, which could prevent patellofemoral OA during long-term follow-up. This mean anterior transfer could also avoid complications, such as delayed wound healing and nonunion at the osteotomy sites. However, 24% of the patients (4 knees of 17 knees) experienced significant screw irritation and required screw removal. Screw irritation is one of the disadvantages in this procedure in the same way as the Fulkerson procedure. 21,29 We think that anterior transfer of tibial tubercle contributed to this phenomenon. Preoperative counseling regarding the possible need for screw removal is essential.
Medial patellofemoral ligament (MPFL) reconstruction is the most well-known procedure for the treatment of recurrent patellar dislocation; it can reproduce the primary restraints against lateral patellar displacement. 1,30 With regard to the long-term results of this procedure, Nomura et al. reported that only 2 of 24 MPFL-reconstructed knees experienced postoperative redislocation or subluxation in the long-term follow-up, and the progression of patellofemoral arthritis in two knees (8.3%). 22 Deie et al. stated that MPFL reconstruction provides a significant improvement in Kujala scores, with no recurrent dislocation in 46 knees followed up for a mean of 9.5 years. The progression of patellofemoral OA was not mentioned in their report (Table 1). 23 The long-term clinical outcome of MPFL reconstruction shows satisfactory results in terms of preventing subluxation or dislocation, but the progression of patellofemoral OA remains unclear. MPFL reconstruction does not address potential osseous problems and can also result in overload of the medial patellofemoral cartilage, particularly in case of large TT–TG distance. In the present study, the mean TT-TG distance was 20.0 ± 2.5 mm, which is a good indication for distal realignment, leading to satisfactory clinical results.
There were some limitations in this study worth noting. First, this study is a retrospective case series, which was not compared with a control group. Comparisons with other follow-up studies are difficult because a significant heterogeneity in the inclusion criteria was found for the studies and the surgical technique. Second, the minimum follow-up of 5 years was not sufficient for accurately evaluating OA progression. Third, four cases were lost to follow-up in our study, raising the possibility of some bias. Finally, the sample size is small. Other long-term follow-up studies for the treatment of recurrent patella dislocation have larger cohorts. Further study of a larger number of cases with long-term follow-up is necessary. Despite these limitations, this is the first reported study that investigated the long-term results of the crosse de hockey procedure for the treatment of recurrent patellar dislocation.
Conclusions
This study demonstrated that the crosse de hockey procedure showed satisfactory long-term clinical results for recurrent patellar dislocation. The procedure could prevent the progression of patellofemoral OA because of the unloading effect of the patellofemoral joint by anteromedial transfer of the tibial tuberosity.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.