
Abstract
Purpose:
Fingertip replantation is a challenging and technically demanding procedure. A variety of venous drainage techniques have been attempted for successful fingertip replantation. We present a new venous drainage technique, known as serial multifocal incision for fingertip replantation.
Methods:
Between 2006 and 2014, we performed 94 fingertip replantations without vein anastomosis. Eighty of the patients were male, and 14 were female, with an overall mean age of 42 years (range: 8–67 years). All patients suffered amputations distal to the distal phalanx joint (Ishikawa subzone I, II, or III). We performed only artery anastomosis. To relieve venous congestion, we incised the fingertip 2–3 mm using a number 11 scalpel blade and allowed the vein to drain naturally. We made small serial incisions every 2–3 days for 1 week.
Results:
The overall success rate for this procedure was 90%, with 85 surviving digits. Two patients with partial necrosis and nine patients with complete loss needed a second operation. Two patients received blood transfusions with an average of 1.5 units, but both had an accompanying injury at another site. No one complained of nail deformity or wound infection.
Conclusions:
Various external bleeding techniques have been reported to yield good results. The serial stab incision venous drainage technique is a modified fish-mouth external bleeding technique that overcomes the disadvantages of published methods. This technique is simple, allows for easy control of venous drainage, and reduces the need for blood transfusions compared to other venous drainage techniques that cause large amounts of bleeding. We propose a new method, the serial stab incision venous drainage technique, which is effective and associated with high rates of survival.
Introduction
Successful fingertip replantation involves the provision of good soft tissue coverage, preservation of the nail, and retention of original digital length. 1,2 Currently, replantation is the preferred approach for amputated fingertips, even though it is a challenging and technically demanding procedure.
Adequate venous drainage is the key to successful replantation. Because it is technically difficult to locate suitable veins in the fingertip, micro-surgeons treat “artery-only” finger replantations with a variety of venous drainage techniques. Representative external bleeding techniques, such as the fishmouth method (transverse tip incision), 3 medical leeching, 4 and chemical leeching, 5 have been reported to yield good results. However, such methods also introduce complications, such as increased infection risk and a greater likelihood of blood transfusion due to uncontrolled bleeding. 6,7 After performing many fingertip replantation procedures, we have gained extensive knowledge regarding the inconvenience of managing replantation wounds.
In this study, we present a simple new technique, referred to as serial stab incision for venous drainage in fingertip replantation. Herein, we report results from 94 artery-only fingertip replantations using the serial stab incision method.
Methods
This study was approved by the Institutional Review Board (IRB) of Busan National Hospital. We retrospectively examined 94 fingertip replantation surgeries performed between 2006 and 2014 that used the artery-only technique. Patients who underwent fingertip replantation with vein repair during this period were excluded. Patients who had another injury in the same finger, such as bone, tendon, or soft tissue defect or who had multiple level amputations in the same finger were excluded. Eighty of the patients included in the study sample were male, and 14 were female, with an overall mean age of 42 years (8–67 years). All fingers were amputated distal to the distal phalanx joint: 22 digits at Ishikawa subzone I, 62 digits at Ishikawa subzone II, and 10 digits at Ishikawa subzone III. Among the injury types, 22 digits had clean-cut injury, 60 digits had a crush-cut injury, and 12 digits had a crush-avulsion injury. The involved digits comprised 17 thumbs, 21 index fingers, 31 middle fingers, 17 ring fingers, and 8 little fingers.
We were performed “artery-only” finger replantations under general or regional anesthesia. After fingertip replantation, we made a 2–3-mm small incision using a number 11 blade scalpel on the fingertip at the far end from the anastomosed artery (Figure 1). We formed a cotton bud with a heparinized saline solution (25,000 IU heparin in 1000 mL physiologic saline). 7 Caregivers of replantation patients were instructed to swab the incision site with a heparin-wetted cotton bud if the bleeding stopped at the incision site. On the second or third postoperative day, we made a second small incision on the opposite side of the finger from the first incision. On the fourth or fifth postoperative day, if there was remaining venous congestion, we made a third incision on the top of the fingertip (Figure 2). We did not use other external bleeding techniques, such as heparin dropping, medical leeching, or local heparin injections during this procedure. All patients received continuous intravenous 500 mL/day dextran 40 and 10 mcg Alprostadil (PEG1) for 5 days and low-dose aspirin (3 mg/kg) for 2 weeks. In our experience, venous drainage for 1 week was sufficient to restore venous flow naturally. None of our cases required further venous bleeding after 1 week (Figure 3).

Schematics of the “Serial Stab Incision Venous Drainage Technique.”
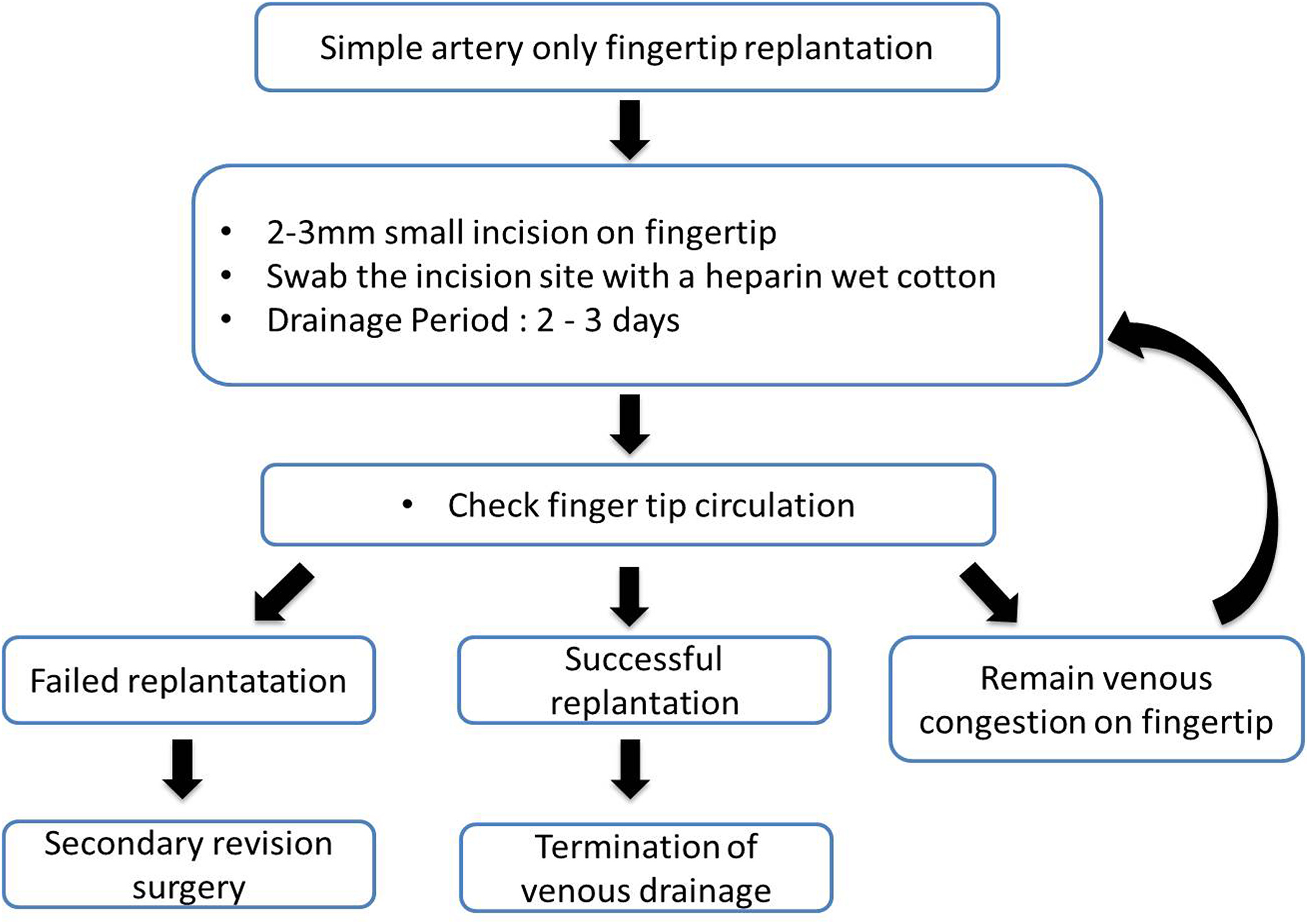
The “Serial Stab Incision Venous Drainage Technique” protocol for simple artery-only fingertip replantation.

Thirty-six old male patient were amputated at the right fourth fingertip. (Ishikawa II). We performed the serial incision technique after artery-only fingertip replantation. After successful replantation, a good fingertip figure was obtained 6 months later..
Results
The overall success rate for this procedure was 90%, with 85 surviving digits. Two patients with partial necrosis at Ishikawa subzone II or III healed naturally without a second operation. Nine digits were lost completely: two digits at Ishikawa subzone I, five digits at Ishikawa subzone II, and two digits at Ishikawa subzone III (Table 1). The nine digits that were completely lost underwent a second operation: three digits received a V–Y advanced flap, two digits received a thenar flap, three digits received a reverse island flap, and one digit underwent stump revision. There were no cases of wound infection in any of the patients (Table 2). A total of 54 cases (57%) had 2 stab incisions, and 40 cases (43%) had 3 stab incisions. All failed cases required 3 stab incisions for success. Five digits demonstrated pulp atrophy at the final follow-up and had received three stab incisions in postoperative management. Three patients complained of deformity in the injured nail bed, but those injuries did not result from the serial stab incisions. Only two patients received a blood transfusion: one patient who had a radial artery injury received two units of blood, and another patient who had a deep muscle rupture in the lower leg received one unit of blood.
Failure cases by type of injury and level of injury.

Summary of secondary revision surgeries.

Discussion
Fingertip replantation is currently the most useful procedure for amputated fingers, despite its technical difficulties. Highly developed microsurgical skills and instruments are required for fingertip replantation. Early reported success rates for fingertip replantation in which an artery and vein can be repaired were 70–90%. 8 Recent outcomes from artery-only fingertip replantation feature high success rates ranging from 64–100%. 2,9,10 Fingertip survival after replantation is influenced by patient age, injury type, smoking history, ischemic time, and amputation level. 11 While some publications have reported that the relationship between survival rate and venous repair is unknown, 12,13 we generally accept that venous drainage after fingertip replantation works to relieve postoperative venous congestion and increase replantation success rates. 2,8,11
A variety of methods of venous drainage have been published: fish-mouth incision or paraungal incision with or without anticoagulant medication, 3,7 medical leeching, 4 arteriovenous shunt, 14 and venocutaneous fistula. 15 Several studies have reported high success rates for fingertip replantation using these techniques. 7,16,17 In particular, external bleeding techniques, including medical leeching and chemical leeching, are widely used because of their ease. The simplicity of external bleeding techniques reduces operation time and microsurgeon burden. However, the external bleeding technique is also accompanied by some risk, as the amount of postoperative bleeding is unpredictable. Close monitoring is necessary and patients often require blood transfusions. Medical leeching increases infection risk as well as risks for osteomyelitis and septicemia. Because it is difficult to position medical leeches on the fingertip, some researchers have reported losing leeches into the body cavity. 6 Consequently, some hospitals have disallowed medical leeching.
Chemical leeching, which involves topical heparin application, is another traditional method. It has a low infection risk and is more widely available at hospitals than medical leeching. 7,16,17 This technique is more useful when performed with partial nail removal 18 or with a fish-mouth incision. 3 However, unpredictable bleeding is the main problem associated with this method. 12 Han et al. reported that most patients (88%) required blood transfusion after chemical leeching. 7 In our experience, continuous heparin application allows maceration of the wound and interferes with assessment of fingertip congestion. The attending surgeons and nurses must perform several dressing changes. Multiple scratches on a fish-mouth incision increase wound size and can cause scar pain.
In our opinion, an ideal external venous drainage technique for fingertip replantation must have several characteristics: it should be simple, have the ability to maintain continuous drainage and prevent coagulation, minimize stump injury, and cause few cosmetic problems. It should be easy to control the drainage amount and the drainage period of venous bleeding. Based on our criteria, the external bleeding techniques mentioned above are unlikely to fully meet these conditions.
In this study, we performed a serial stab incision technique as an alternative to external bleeding methods. Our method is straightforward and safe and can achieve sufficient bleeding by swabbing the wound with a heparinized cotton bud. Thus, most patients did not require a blood transfusion. Two patients who received blood transfusions had another vessel injury or deep muscle laceration. We achieved adequate venous drainage without blood transfusion and achieved a high success rate with our serial stab incision technique. Small incisions leave a small scar and minimize scar pain and cosmetic problems. Therefore, the serial stab incision technique would be an appropriate alternative to external bleeding techniques.
Recent studies have reported high success rates for fingertip replantation at Tamai zone I using an external bleeding technique without vein repair. 12,19 Chen et al. 12 hypothesized that bone bleeding and wound-edge bleeding are sufficient for replanted fingertip survival. We propose that our high success rate might be due to similar causes. Therefore, we suggest that it is advantageous to use the artery-only fingertip replantation and serial stab incision technique for Ishikawa subzone I or II injury, because it is difficult to find veins in Ishikawa subzone I or II, and this technique reduces operation time. In Ishikawa subzone III or more proximal levels, surgeons should try to find an anastomosis-adequate vein, and the external bleeding technique should be a backup option.
The limitations of this study include the lack of comparisons between groups using previously published venous drainage procedures and groups using our method. However, our new method demonstrated a high success rate. Second, although the amount of blood transfused was small compared with transfusions associated with previously published external bleeding techniques, the actual amount of bleeding was not measured. In this study, we did not collect data for outcomes of sensory. Our institute previously performed neurorrhaphy but do not do so at the present time, because the protective sensory was obtained without neurorrhaphy and patients did not complain about sensory deficiencies
In conclusion, reestablishment of venous flow is the key to successful fingertip replantation. The serial stab incision technique is an easy and safe venous-drainage procedure. Thus, it is a simple method that effectively saves time and effort and has a high survival rate for artery-only fingertip replantation.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Medical Research Institute, Pusan National University Hospital.