
Abstract
The ‘all-inside’ meniscus repair is extremely useful technique in addressing tears at the far posterior horn of meniscus. However, this procedure may place the popliteal neurovascular bundle at risk of injury. The purpose of this study was to evaluate the risk of popliteal artery injury by the trajectory of anchor delivery instruments inserted through standard knee arthroscopic portals for the repair of the far posterior horn of meniscus tears. Standard arthroscopic portals were marked on five human cadaveric knees which were subsequently disarticulated. Axial photographs were taken after marking the 5 10, and 15 mm points from the meniscal root on the posterior horns of the menisci. The unsafe zones for meniscus repair at each of these points were identified on the photographs of knees by first drawing two lines from the edges of the popliteal artery and crossing at the respective points at the posterior horns. The points at which these lines meet a circular protractor applied to the center of each meniscus in the knee photograph were recorded as a range. The range signifies the unsafe zone for each respective point on the posterior horn of meniscus. The anterolateral arthroscopic portal fell within the unsafe zone of the 5 mm point on the posterior horn of lateral meniscus in three of the five knees and within the unsafe zone of the 10 mm point on the posterior horn of lateral meniscus in another two knees. A cautious approach should be practiced during the repair of tears located at these two points. None of the other points’ unsafe zones (lateral 15 mm, medial 5 mm, 10 mm and 15 mm points) coincided with the ipsilateral portal sites.
Introduction
The menisci, which were once assumed to be functionless vestigial structures, are now understood to be indispensable to the function of healthy knee joints. Total meniscectomies, which were the primary choice of treatment for meniscal injuries for the longest period of time, were recognized to significantly accelerate degenerative changes and induce early onset osteoarthritis. 1 –3 This has led to a shift of paradigm towards meniscal preservation procedures instead, with the ‘all-inside’ meniscal suture repair being the latest in the array of repair techniques.
The inception of the all-inside repair technique had imaginably resulted from the various pitfalls and limitations of its predecessors. Both the ‘inside-out’ and ‘outside-in’ methods were hardly useful in addressing far posterior meniscal tears; they require tunnelling of needles anteroposteriorly for suture anchorage of these lesions which would invariably necessitate additional incisions and essentially place the popliteal neurovascular structures at risk. The alternative to this predicament would be to instead aim the tunnelling needles medially or laterally, which may not necessarily be less laborious and may ultimately result in unsatisfactory non-anatomic reduction. The all-inside technique, on the other hand, allows these pesky lesions to be approached exclusively from the conventional anterior arthroscopic portals and the repair sutures to be placed perpendicular to tear patterns. 4
The all-inside repair devices are currently in its fourth incarnation. Despite the evolution in the design of the various available implants across its generations, the technique still is not free of the possibility of popliteal artery injury during posterior meniscal horn repair. Although (to the best of our knowledge) no accounts of this calamitous event had ever been documented in the literature, a laceration or puncture of the vessel by the inserter/delivery needle may theoretically occur in attempts to deploy the anchors outside the capsule.
We were only able to identify two separate reports assessing the relationship between the all-inside posterior meniscus repair and its risk of popliteal artery injury. One had found that none of the devices, when deployed in cadaveric knees, were within the proximity of the popliteal vessels 5 while another had found the inserter needle to be within a mean distance of 0.5 mm to the artery when measured on AP knee X-rays upon intravenous injection of contrast into the artery. 6
The purpose of this study was to evaluate the correlation of the risk of popliteal artery injury to the trajectory of anchor delivery instruments inserted through standard anterolateral and anteromedial arthroscopic portals, with regards to the anatomical locations of the far posterior meniscal tears. From this, we also aimed to identify the unsafe zones encountered in posterior meniscus repair, with respect to the danger of popliteal artery injury. Our hypothesis is, the more posterior the tear of the lateral meniscus, the more risk of developing arterial injury while using all-inside technique for meniscus repair.
Methodology
Five fresh frozen human cadaveric knee specimens were used from five different donors. The medical ethics committee approval was awarded from our institution for this project. The knees included 20 cm of femur and 15 cm of tibia with overlying soft tissue. They were kept frozen at −18 °C and have been thawed at a room temperature overnight for 12 h before use. The knees were mounted to a custom-made frame to hold the knees firmly in supine position and 90° flexion. Standard anterolateral and anteromedial arthroscopic portals have been established using size 11 blade and trocar. The portals located at the soft points 1 cm away from the patellar tendon at the joint level. A marker pen was used to identify these portal sites. The skin, subcutaneous tissue, muscles, and fibula were dissected and excised leaving the knee joint capsule and the popliteal fossa intact. Then, each knee was transected (disarticulated) at the knee joint level from anterior to posterior starting from the portal points through the patellar tendon and then posteriorly, with extra attention paid to preserve the menisci and meniscocapsular junctions. When the menisci exposed, the transection progressed posteriorly through the posterior joint capsule and the popliteal fossa neurovascular structures. The popliteal artery was transected level to the meniscocapsular junctions. After complete transection of the knees, the tibial part positioned vertically on the frame was the tibial articular surface and the menisci facing up. Points on both the posterior horns of the medial and lateral meniscus were marked at a distance of 5, 10, and 15 mm from the posterior meniscal roots, the points were measured with a ruler and marked with lines (Figure 1). The articular surface of the tibial portion of the knee joints was then photographed axially (from above) along the axis of the tibia. The photographs were uploaded onto a computer and measurements were made on a Keynote platform.

Using a ruler and a marker, the posterior horns of the cadaveric menisci were measured and marked as lines at points 5, 10 and 15 mm away from the roots of the menisci.
From each respective knee’s photograph, the arthroscopic portal sites, patella ligament, the outline of the popliteal artery, along with the midpoints of each of the 5, 10 and 15 mm lines, were identified and marked. A posterior referencing line was subsequently drawn from the posterior-most edge of both the medial and lateral meniscus to determine the coronal orientation of the knee (Figure 2).

Initial markings made on the axial photograph of a right knee. Area highlighted green: patella ligament; asterisks (*): arthroscopic portal sites; dots with red outline: midpoints of the 5, 10 and 15 mm lines on the posterior horns of the menisci; arrow: posterior referencing line across the posterior edge of both menisci; circle with dotted outline: outline of the popliteal artery (which can be seen here to be off-centre, and like in the rest of the samples, was related posteriorly to the posterior horn of the lateral meniscus).
To identify the unsafe zones for each of the 5, 10 and 15 mm points on the menisci, two lines (A and B) which meet and cut across one another at each single point (taking, for instance, the 5 mm point) were initially drawn, beginning at the edges of the outline of the popliteal artery. These lines were extended forward from the popliteal artery to the periphery of the knee (Figure 3). A circular protractor with points of increment of 0.5° was next applied onto the photograph, resized and positioned that its circumference coincides with the circumference of the corresponding meniscus, and its centre with the centre of the corresponding plateau. To standardize the procedure, the 0° reading of the protractor was always kept at the centre of the knee (medially), and its 90° reading placed anterior at the perpendicular line to the posterior referencing line which was initially made (Figure 4). The points where the above two (lines A and B) lines meet the circular protractor anteriorly were then recorded as a range; the reading was done in a clockwise manner for the lateral meniscus and in a counter-clockwise manner for the medial meniscus for the right knees (Figure 4), and vice versa for the left (Figure 5). The range (in degrees) signified the unsafe zones for each of the points on the posterior meniscus, where the insertion of a straight anchor delivery instrument along this trajectory will risk injuring the popliteal artery.

Unsafe zone measurement of the 5 mm point on the lateral meniscus of a right knee. Two lines (labelled A and B) were drawn, each starting from the edge of the popliteal artery outline (circle with dotted outline), meeting and crossing at the centre of the 5 mm point (dot with red outline) and ending anteriorly.
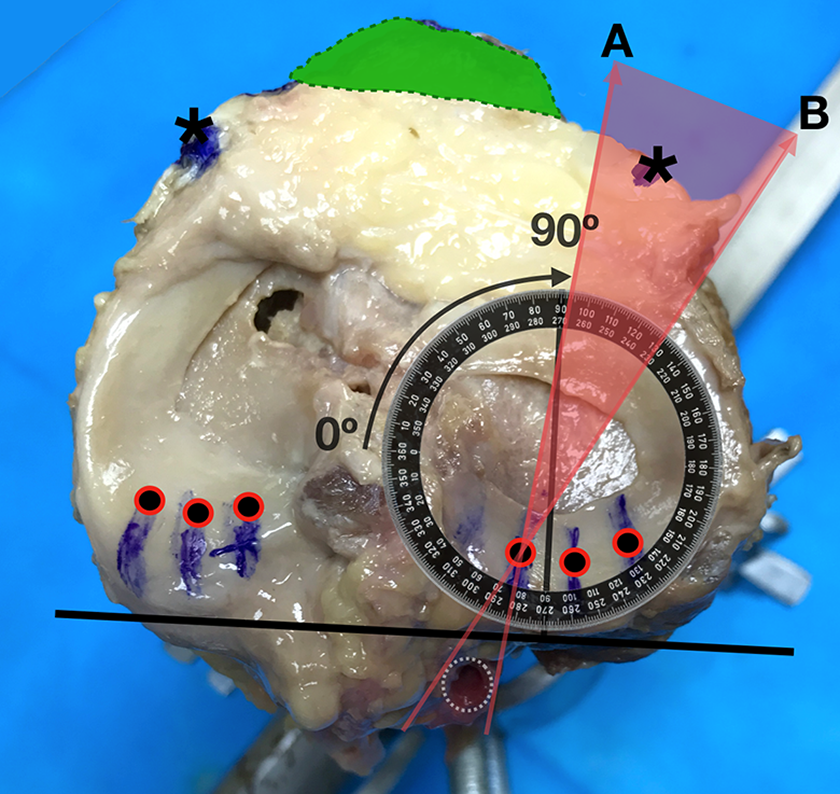
Unsafe zone measurement of the 5 mm point on the lateral meniscus of a right knee. A protractor was applied onto the photograph, resized, and positioned over the lateral plateau. Note the positions of the 0° (centre of the knee) and 90° (anterior, perpendicular to the posterior referencing line) of the protractor. Reading is performed clockwise (curved arrow).

Unsafe zone measurement of the 5 mm point on the lateral meniscus of a left knee. Note the position of the protractor. Reading was performed in an anticlockwise manner here (curved arrow).
The entire exercise was repeated for all six points on each knee, with a total of 60 readings (two readings per point; six points per knee; five knees). Statistical measures and analysis were obtained for all six points in five knees.
Results
Of the five knees, three originated from female donors and two were from male donors. The mean age was 70.33 years old, with a range of 51–87 years old. All were of Caucasian descendent. Three of the knees were right sided (knees number 1, 2 and 3), whereas the other two were left (knees number 4 and 5). In all five knees, the popliteal artery was found to be the deepest structure of the popliteal fossa neurovascular bundle and were all located slightly off centre, sitting closer to the posterior aspect of the posterior horn of the lateral rather than the medial meniscus. No anatomical variations of the artery (i.e. a high division of the anterior tibial artery) were seen in all five knees.
The anterolateral arthroscopic portal site fell within the unsafe zone of the 5 mm point on the lateral meniscus’ posterior horn in three of the five knees and within the unsafe zone of the 10 mm point on the lateral meniscus’s posterior horn in another 2. None of the other points’ unsafe zones (lateral 15 mm, medial 5 mm, 10 mm and 15 mm points) coincided with the ipsilateral portal sites; they were in fact observed to be quite a distance away (Figure 6).

The unsafe zones of knee number 2. The anterolateral portal site fell within the unsafe zone of the lateral meniscus 5 mm point. Also note how the unsafe zones of the medial side were a considerable distant away from the anteromedial portal; this finding was universal to all samples.
The unsafe zone data and derivative statistical measures (mean, standard deviation, median, minimum and maximum) are shown in Table 1. The mean unsafe zone for the repair of a lateral meniscal posterior horn tear 5, 10 and 15 mm from the root is approximately 80° to 120° (79.9° ± 12.4 to 117.1° ± 12.4 in actuality), 130–160° (125.2° ± 12.1 to 161° ± 17.1 in actuality) and 160–180° (159° ± 10.7 to 183.8° ± 12.9 in actuality), respectively. Comparatively, the mean unsafe zone for the repair of a medial meniscal posterior horn tear 5, 10 and 15 mm from the root is approximately 140–160° (135.2° ± 20.5 to 159.6° ± 14.6 in actuality), 160–180° (164° ± 14.8 to 183.9° ±12.6 in actuality) and 180–200° (184.4° ± 10.6 to 198.7° ± 12.1 in actuality), respectively.
Unsafe zone data and derivative statistical measures of the five knees.

Discussion
The menisci have crucial roles to play in the normal biomechanics of the knee joint. They contribute to the stability, lubrication, load transmission, shock absorption, nutrition and proprioception of the joint and also increase its congruity and reduce its contact stresses. 7 Meniscal injury may therefore lead to the attenuation of these functions and consequently induce early osteoarthritis. 8,9
Demographically, 87% of meniscus tears in knees without ligamentous injuries 10 and 94% of meniscus tears in anterior cruciate ligament deficient knees 11 involved the posterior horns of the meniscus. The prevalence of these posterior lesions is compounded by their comparatively lower healing rates, 12 and by the arduousness in older repair techniques.
The all-inside meniscal repair technique was first described in 1991 by Morgan et al. to specifically deal with posterior and posterocentral meniscal horn lesions which they had found difficult to address with the conventional ‘inside-out’ and ‘outside-in’ techniques. 13 The design of the technique and devices had come a long way since. The current devices are considerably easier to use and therefore reduces operative time and require neither an accessory incision nor an extra assistant. 4 Complications associated with the obligatory posterior incisions of the inside-out and outside-in techniques such as arthrofibrosis, knee effusion, infection, deep vein thrombosis, reflex sympathetic dystrophy and nerve injury 14,15 are also avoided. Moreover, biomechanical studies had found the all-inside suture technique to have comparable primary repair strength when pitted against the outside-in technique. 16
Although (as far as we’re concerned, up till the time of writing) no incidences of popliteal artery injury had been reported with the all-inside repair technique, the procedure may technically still place the artery at risk specifically when dealing with posterior meniscal lesions. This may inadvertently occur during passage of the anchor inserter needle anteroposteriorly, given the lack of intraarticular landmarks to determine the artery’s location and to guide its trajectory. An injury to the artery may lead to the development of pseudoaneurysms or arteriovenous fistulas 17 –19 which will most certainly require further surgery and hinder postoperative rehabilitation or much worse, may result in amputations when not detected early. 20
Two studies had previously assessed the risk of popliteal artery injury in the all-inside technique. Coen et al. in their study to determine the locations of the T-fix (Acufex Microsurgical, Mansfield, Massachusetts, USA) all-inside suture devices in relation to the capsule, neurovascular and musculotendinous structures of cadaveric knees, had found that none of the devices were within the proximity of the popliteal neurovascular structures despite setting application depth at a maximum 2 cm. They had further concluded that a buffer zone of 1.5 cm are present between the devices and the popliteal neurovascular bundle when repairing the posterior meniscus horns. 5 On the other hand, by examining the X-rays of cadaveric knees with contrast filled popliteal arteries and radio-opaque painted ‘all-inside’ inserter needle (The Smith & Nephew (Andover, Mass) FasT-Fix and Mitek (Raynham, Mass) RapidLoc) inserted into the posterior aspect of their lateral menisci, Cohen et al. had found that the mean distance between the needle and the artery to be 0.5 mm (lateral X-ray) and 6.0 mm (AP), respectively, for the FasT-Fix system and more than 20 mm (both lateral and AP X-rays) in the RapidLoc system. They had concluded that the latter was safer and had attributed it to the shorter inserter needle length. 6
In our study, instead of examining the safety profile of available devices which designs are ever changing, we evaluated the risk of popliteal artery injury with respect to the locations of the posterior meniscal tears which we believe to be more consistent. Affirming to most anatomical studies, the popliteal arteries in all our cadavers were lateral to midline and are related posteriorly to the posterior horn of lateral meniscus. 21,22 None had a high anterior tibial artery origin, which may pose as an additional danger during meniscal repair procedures as this branch, when present, will be directly related to the posterior tibial cortex. 23
Our results show that utilizing the conventional anterolateral portal to perform an all-inside repair of lateral meniscal posterior horn tears located 5–10 mm from the meniscal root puts the popliteal artery within the trajectory of instruments and thus at risk of injury, which correlates to the normal anatomical relationship between the two. A cautious approach to tears located here should therefore be exercised; measures to minimize the danger would include limiting inserter needle penetration depth, the use of a curved needle tip instead of a straight one and angulating the tip away from midline. An accessory portal away from midline may also be considered here.
We also found that utilizing the anteromedial portal to repair medial meniscal posterior horn tears will conversely be very safe, as the artery does not lie within the portal’s trajectory at all. The same can be said for tears located 15 mm on the lateral meniscus’ posterior horn.
Limitations
We note several limitations to our study. Most obviously, anatomical variations to the popliteal artery may be present and must be kept in mind. A high tibial artery origin may be present in up to 6% of the population. 23,24 Secondly, only five cadaveric knees were available for the study. Understandably, a higher number of samples, if available, will allow for a wider observation of variations. Also, as pointed out by several studies, the position of the popliteal vessel may vary with flexion, extension and even external rotation of the knee and also with distension of its joint space with fluid, as with during routine arthroscopy of the knee. We however believe our decision to omit these fastidious simulations from our study was justified, as we coincidentally found the range of distance between the posterior cruciate ligament insertion and the popliteal artery in our cadaveric knees to be between 3 and 19 mm, which was not far off from those reported in MRI studies simulating these conditions, 4–16 mm 25 and 3.33–16 mm 26 and would be unlikely to affect the findings.
Conclusion
Based on the results of our experiment, we conclude that performing the all-inside repair of the posterior horn of the lateral meniscus 5–10 mm away from the posterior root using the anterolateral arthroscopic portal places the popliteal artery at risk. This should be borne in mind especially in addressing acute meniscal injuries which more commonly involve the lateral meniscus, where precautionary measures should be employed as limiting inserter needle penetration depth and the use of a curved needle directed away from midline.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.