
Abstract
Background:
Wearing high heels for an extended period of time can cause several pathological conditions in women’s feet, one of such is the hallux valgus (HV), as shown by a number of cross-sectional studies. This study aims to evaluate the incidence of HV among sales promotion women and to know the association of the high heel shoes with the severity of HV in that population.
Method:
This study used comparative cross-sectional design between two groups, wearing high heel and flat shoes; sales promotion women who work for at least 1 year were recruited as subjects by means of purposive sampling and were given questionnaires, and then physical and radiological examination of the foot were performed to detect any HV and its severity.
Result:
Incidence of HV is 25.25% (25 of 99) among subjects who were wearing high heel shoes and 10.87% (10 of 92) for those who were wearing flat shoes. Subjects wearing high heel shoes are 2.77 times (95% confidence interval (CI): 1.25–6.15; p = 0.01) more at risk for developing HV than those who wore flat shoes. The incidence of HV increases with age (p < 0.05). Those who have been working for >4 years are 5.2 times (95% CI: 1.95–14.31) at more risk for developing HV than those who have been working for ≤4 years (p < 0.001). The duration of wearing shoes per day, the type of toe box, and body mass index are not statistically significant with HV (p > 0.05). The incidence of HV increased among overweight and obese subjects (p > 0.05). The severity of HV in subjects was mostly mild to moderate.
Conclusion:
The incidence of HV is higher among sales promotion women who wear high heel shoes than flat shoes. Age and working experience are also related to the development of HV. Factors that affect the severity of HV cannot be shown in this study.
Introduction
Hallux valgus (HV) is a chronic condition that is characterized by the presence of deformity in the first metatarsophalangeal joint, which is due to the lateral drift of the great toe 1 caused by joint subluxation 2 and which turns the toe out of the body axis midline. Clinical findings include an erythematous and swollen appearance of the great toe and surrounding areas and where pain is located on the inside of the foot. 3 A number of cross-sectional studies indicate that wearing high heels is strongly associated with HV 4 ; for example, Dufour et al. 5 conducted a foot study of older adults and reported that 44% of women had HV. History of wearing high heels as the main shoes at age 20–64 years increased the incidence risk of HV by 47% (p < 0.01). Another example was a scientific literature review by Barnish and Barnish 6 who reported four studies that assessed the relationship between high heels and HV. Among those, three studies found a significant association (75%).
HV occurs in 2–4% of the population, 7 especially in shoe-wearing populations. 8,9 Mann and Coughlin reported the incidence of HV in adult shoe-wearing populations by 33%. The number of HV varies greatly depending on the subject being investigated. 10 Most studies found that this condition appeared mostly in women, especially the ones who wore high heels shoes with a narrow toe box. 8,11
Wearing high-heeled shoes with a narrow toe box was a very important extrinsic factor in HV formation and has been proved to increase the severity. 8,12 Biomechanical studies showed that heel elevation on high heels increased pressure under the metatarsal head and limited the motion of the first metatarsophalangeal joints. Additionally, shoes with narrow toe box increased pressure on the medial aspect of the foot and between the toes. 4 Genetic factor, 7,12,13 age, ligament elasticity, first ray hypermobility, metatarsal morphology, 13 and pes planus 7,13 were intrinsic factors that also play a role in HV formation.
Sales promotion women in department stores are one among the population wearing high-heeled shoes in Indonesia; therefore, they have more risk to develop HV. The symptoms can affect daily activities if not treated promptly. Until now, to the best of our knowledge, study evaluating the relationship between wearing high heels and HV incidence in Indonesian has never been done; thus, this study aims to determine the number of HV incidence among sales promotion women in department stores as well as the factors that contribute to the development and severity of HV. Our hypothesis is that the incidence of HV in the subjects wearing high heel shoes is higher than subjects wearing flat shoes.
Materials and methods
This study used a comparative cross-sectional design to see the comparison of HV incidence among sales promotion woman wearing high heels when compared with flat shoes at a department store in Bekasi city, West Java, Indonesia. The subjects of this study were sales women who wear high heels or flat shoes with the sampling being taken with a purposive sample technique. The inclusion criteria are that all subjects have worked for at least 1 year as a sales promotion woman at the department store and willing to take part in this study. The exclusion criteria were also listed with the subjects who have any foot problem other than HV such as septic arthritis on the foot, having a history of gout or history of foot surgery and rheumatoid arthritis. Subjects with a family history of HV, history of HV before using high heels, who were pregnant, and not present at the time of the study were also excluded. The same goes with for those who did not follow the research procedure.
All subjects were given questionnaires containing the respondent’s identity and a list of questions that include job history (working experience, duration of wearing shoes per day while working), type of shoes for work (including type of toe box), having symptoms of HV, history of previous and current illness, and history of the same disease in the family. Objectively, height, weight, and body mass index (BMI) were recorded. Subjects’ foot condition was also examined, with subjects with great toe drift to the second toe 7,14,15 and those with increased size of medial aspect of first head of metatarsal 16 being referred to the radiology department for an X-ray. Criteria diagnosis of HV was based on the clinical condition of the foot, supported by foot radiology examination, which is done with a dorso-plantar view on the standing position. Radiographic evaluation was performed by measuring the HV angle (HVA). 9 HVA > 15° is defined as HV. Classification of HV severity is mild (HVA 15° to <20°), moderate (HVA 20°–40°), and severe (HVA > 40°). 7,14
HV, severity of HV, type of shoe, toe box, age, duration of work, duration of wearing shoes per day while working, and BMI were defined as analyzed variables, while the type of shoe is divided into high heels (≥5 cm in heel height) and flat shoes (<5 cm in heel height, including those without any heels). Toe box type is divided into narrow if the shape of the toe box is pointed and wide if the shape of the toe box is square or round. BMI category is based on BMI category for Asia Pacific Region and has been simplified for the purpose of this study by merging underweight and normal categories into “Normal,” “Overweight,” and merging Obesity I and II categories into “Obese.” Processing, analysis, and presentation of data were done using SPSS program version 20.0. Data were analyzed as univariate and bivariate, with χ2 or Fisher’s exact test. All procedures undertaken in this study were approved by our institutional ethical committee.
Results
This study was participated by 207 sales promotion women. Two being excluded because the subject was pregnant and having foot pain caused by high uric acid level consecutively. Fourteen subjects were dropped out because of the low compliance to the established research procedure, which leaves 191 subjects defined as the subject population for this research. These participants are further divided into two groups consisting of 99 subjects in the high heels group and 92 subjects in the flat shoes group (Table 1).
Distribution of variables according to type of shoes.

SD: standard deviation; BMI: body mass index.
Among the subjects, 18.32% (35 of 191) were clinically diagnosed with HV, with 25.25% (25 of 99) belonging to the high heels group and 10.87% (10 of 92) to the flat shoes group; 71.4% of subjects with HV wore high heels, while 28.6% wore flat shoes. The possibility of HV development in subjects wearing high heels was 2.77 times (95% confidence interval (CI): 1.25–6.15) higher when compared with subjects wearing flat shoes. There is a statistically significant relationship (p = 0.01) between wearing high heels with HV.
The possibility of subjects with high heels–narrow toe box developing HV compared with subjects wearing flat shoes–wide toe box was 2.63 times higher (95% CI: 1.00–6.90) and statistically significant (p = 0.046). Similarly, subjects wearing high heels with wide toe box were 2.7 times (95% CI: 1.01–7.23) more at risk for developing HV when compared with subjects wearing flat shoes–wide toe box (p = 0.043). In other words, subjects with high heels–wider toe box have a similar risk as subjects with high heels–narrow toe box to develop HV. On the contrary, there are no statistically significant differences in subjects with narrow toe box and those with wide toe box to develop HV in the flat shoe group (0.83 times (95% CI: 0.16–4.24; p = 1.00). Conclusively, narrow toe box has also a similar risk as wide toe box to develop HV on subjects wearing flat shoes (Table 2). Actually, the relationship between the type of toe box, itself, with HV was not statistically significant (p 0.532). The probability of a subject with a narrow toe box to develop HV is 1.27 times more than those with wide toe box (95% CI: 0.60–2.67; Table 3).
Hallux valgus according to type of shoes and toe box.

OR: odds ratio; CI: confidence interval.
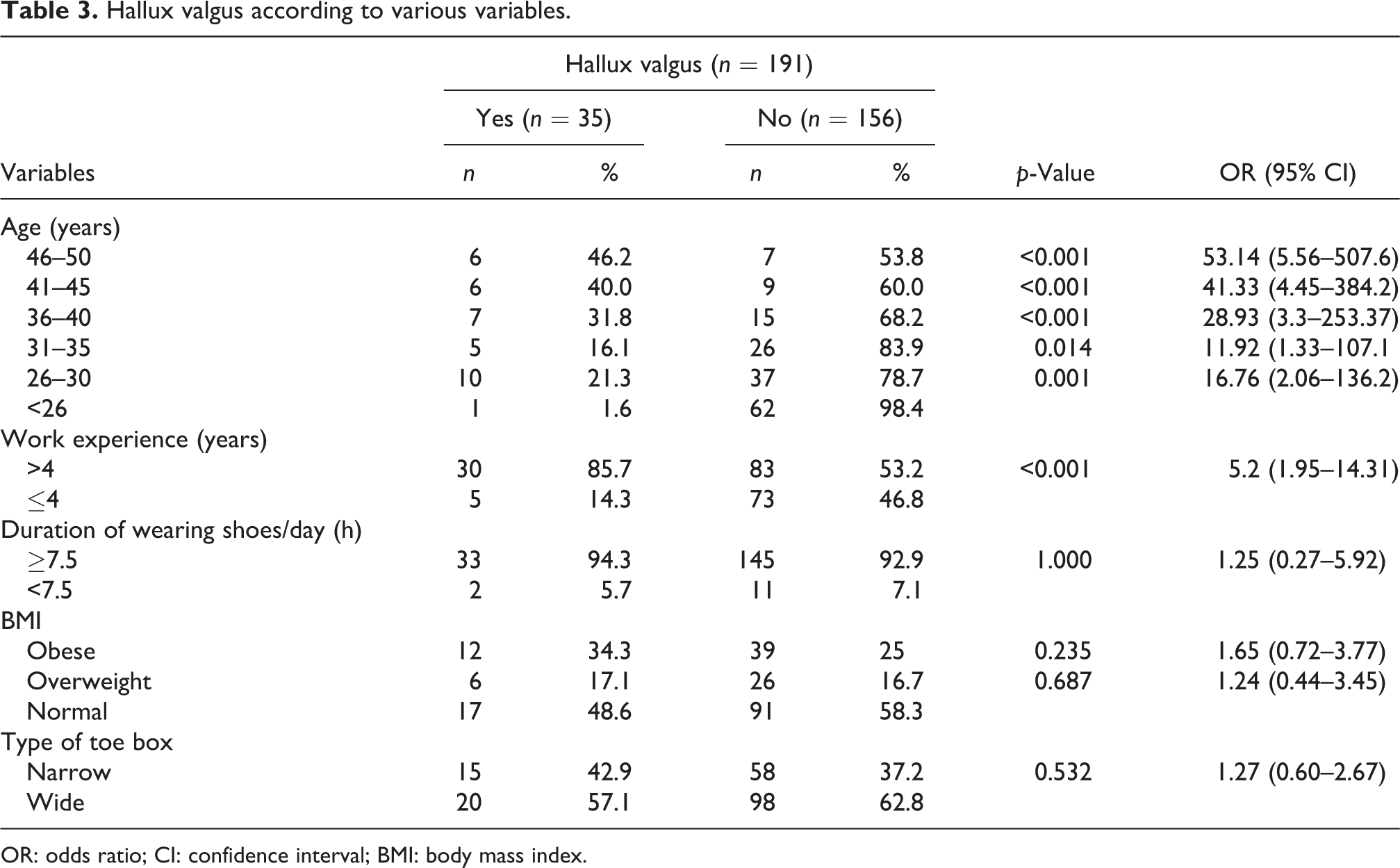
Hallux valgus according to various variables.
OR: odds ratio; CI: confidence interval; BMI: body mass index.
Incidence of HV has been proved to be increased in subjects with age 26–30 years (odds ratio (OR) 16.76; 95% CI 2.06–136.2), 31–35 years (11.92, 1.33–107.1), 36–40 years (28.93, 3.30–253.37), 41–45 years (41.33, 4.45–384.2), and 46–50 years (53.14, 5.56–507.6) when compared with subjects with the age of <26 years. There was a statistically significant relationship between age and HV incidence (p < 0.05).
HV occurred mostly in subjects with a duration of work of >4 years (85.7%). The possibility of subjects with the duration of work of >4 years to develop HV is 5.2 times more likely when compared with those who worked ≤4 years (95% CI 1.95–14.3; p < 0.001). There is no statistically significant relationship (p = 1.00) between the groups whose duration of wearing shoes/day is less or more than 7.5 h, although the number shows that 94.3% subjects with HV are members of the ≥7.5-h group.
Most subjects with HV had normal BMI (48.6%). The possibility of HV is increased in subjects who are overweight (OR 1.24; 95% CI 0.44–3.45) and obese (OR 1.65; 95% CI 0.72–3.77), although no statistical significance can be proved (p > 0.05).
The relationship between the type of toe box and HV was also not statistically significant (p = 0.532). The probability of a subject with a narrow toe box to develop HV is 1.27 times more than those with a wide toe box (95% CI 0.60–2.67; Table 3).
On analyzing the results, the severity of HV combines mild and moderate severity into mild-to-moderate category and severe severity as its own category. The severity of HV in most subjects was mild to moderate (33 of 35). There was no significant relationship (p > 0.05) between the variables with the HV severity (Table 4).
The severity of hallux valgus according to various variables.

OR: odds ratio; CI: confidence interval; BMI: body mass index.
aNot analyzed.
Discussion
A study that evaluated the incidence of HV on sales promotion women or those with similar occupation has never been done before in Indonesia. The incidence of HV in this study was 18.32% (35 of 191). The literature showed that the incidence rate of HV was highly diversified, ranging from 33% to 70%. 2 We believed that this variation has been dependent on the subject being investigated; subjects in this study were sales promotion women who were healthy, while in a previous study as carried out by Roddy et al., 17 the subjects were heterogeneous population with a large number of subjects being patients in midhealth-care conditions or unhealthy people in two primary care population. This study reported that a standardized prevalence of HV was 28.4%, but it was only people of the age bracket of 40 years and 80 years. It may be lower if younger people are included, as in this study. Another study was conducted by Wu and Louie 2 on Chinese women involving sales promotion women as subjects, but the number was very small, which may cause a different result as shown from this study. The important thing is that this is the first study that evaluates the prevalence of HV in a specific population, so that it may give a better understanding on the prevalence of HV and for determining the needs of study material in the future.
The relationship between high heels and HV has been widely studied. High heels have been proved to be one of the extrinsic factors that cause HV formation 7,13 as well as increasing its severity. 8,12 Wearing high heels elevates the pressure on the first metatarsal, which will eventually lead to HV formation, 13 which is an argument supported by Nguyen et al., 18 whose study reported that women wearing high heels 2 in. or more as the main shoes at the age of 20–64 years have 20% increased incidence of HV compared with those who do not.
Sales promotion women who wear high heels regularly are 2.77 times more likely to develop HV when compared with subjects wearing flat shoes. Pressure on the forefoot will increase with the heel height, which increases the load, and therefore the pressure on forefoot and between the toes. 19 Compared with flat shoes, forefoot pressure increases by 22% when wearing a 1-in. heel, 57% for 2 in.-heel, and 76% for 3 in.-heel. 1,3 Comparatively, Wu and Louie 2 stated that in their study of 1056 Chinese women, wearing high heels is not a predisposing factor for HV. Instead, this study stated that family history plays a more prominent role in the development of this condition. This difference may occur because of the different characteristics of respondents.
High heels are often combined with a narrow toe box, which has been statistically proved to increase the pressure on the medial aspect of the foot and between the toes. Over time, this condition can lead to foot deformities such as HV. This is agreed upon by Menz et al. 4 who studied the relationship between shoe characteristics and HV incidence in women and reported that the incidence of HV was increased in women who used large toe-box shoes (OR 1.96; 95% CI 953–1.03–3.71), narrow (2.39, 1.29–4.42), and very narrow (2.70, 1.46–5.00) between the ages of 20–29 years compared with women who wear shoes with a very wide toe box.
The results of this study were different from the one done by Menz et al. In this study, subjects with narrow toe boxes are 1.27 times more at risk than subjects with large toe box, but this was not statistically significant (p > 0.05). Subjects wearing high heels–narrow toe box and subjects wearing high heels–wide toe box are 2.63 and 2.7 times more likely to develop HV, consecutively, when compared with subjects wearing flat shoes with a wide toe box. This argument is supported by its statistical significance. This result is most likely due to the role of high heels itself as it has been established. While in the Menz’s study, heel height has no association with HV but the toe box.
This difference indicates that there is another factor that plays a role in the development of HV. The type of toe box may not be an important factor in comparison with the intrinsic factors. The toe box classification in Menz et al. 4 divides four types of toe boxes, which are very wide, wide, narrow, and very narrow in the age category of 20–29 years old. In this study, toe box type is only divided into two categories, narrow and wide, without age category. That category differences translate to different results. Furthermore, these categories are made because the toe box shape is always changing, following the fashion at the time.
Roddy et al. 17 and Nix et al. 20 showed that HV is strongly associated with age. In the study by Roddy et al., the risk increased every decade, 1.76 (95% CI 1.21–2.58) times at age 40–49 years, 3.50 (2.45–4.99) at 50–59 years, 5.95 (4.16–8.52) at 60–69 years, 7.55 (5.18–10.99) at 70–79 years, and 12.56 (7.89–20.0) at age ≥80 years compared with subjects of age 30–39 years. This study showed similar results with Roddy et al., although the range of the subject’s age was different. The risk and prevalence of HV increased with age. A biomechanical study on the elderly showed changes in posture, kinematic joints, and pressure on the plantar area being associated with HV. 13 This change makes an imbalance between the intrinsic and extrinsic muscles of the foot as well as the ligamentous structures involved, which are generally believed as the formation of HV process. 15 Different results were obtained from Nguyen et al. 18 and Cho et al., 21 with the prevalence of HV being unrelated to age. These different results may occur due to differences in age distribution across the studies.
Most sales promotion women wear shoes for ≥7.5 h per day while working. However, the relationship between the duration of wearing shoes per day with HV was not significant (p > 0.05). Meanwhile, the relationship between the duration of work with HV was statistically significant (p < 0.001). Subjects with the duration of work of more than 4 years are 5.2 times more at risk to develop HV than subjects with a working period of ≤4 years. HV develops slowly, indicating the cause to be repetitive trauma.
13
The
Menz et al. 4 evaluated the effects of cumulative exposure, that is, the number of decades of wearing high heels, with the incidence rate of HV and found no relationship. This is in line with the results of this study, which reveals that the duration of work and the duration of wearing shoes per day are proportional to the effects of cumulative exposure, although the duration of work in this study is related to HV.
Another factor that is related to increasing the metatarsal pressure and the formation of HV is the body weight. 13 HV increases in subjects who are overweight (1.24 times) and obese (1.65 times) compared with the normal BMI subject. This result is similar to Cho et al. 21 in Korea, although this result is not statistically significant (p > 0.05). In contrast, the results from Nguyen et al. 18 and Roddy et al. 17 reported that there was no relationship between BMI and HV. This insignificant BMI relationship may be due to the role of intrinsic factors present in the subject, making the subject more vulnerable to HV, although it is not discussed in this study. Factors that are affecting the severity of HV cannot be shown in this study because of the small number, and only 2 of 35 subjects had severe HV.
Conclusion
HV incidence is higher among sales promotion women wearing high heels than flat shoes and is statistically significant. Age and duration of work are also related to HV. The severity of HV is not affected by the type of shoes, duration of work, duration of wearing shoes per day, and BMI.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.