
Abstract
Objective:
The aim of the study is to investigate the long-term outcome of patients who received Lambrinudi arthrodesis for severe equinovarus deformities.
Methods:
This is a single-center, retrospective study of patients who received Lambrinudi triple arthrodesis of the foot. Both clinical and radiological information were analyzed.
Results:
We were able to review 10 patients suffering from severe equinus deformities mostly as a result of or in association with poliomyelitis (8 of 10) who received Lambrinudi arthrodesis. The majority (7 of 10) of our patients had fair to good outcome at an average follow-up of 37 years. Specifically, six of eight polio patients had fair to good outcome. Of the X-rays available for assessment, the majority of patients showed radiological signs of adjacent joint arthritis; however, the presence of such did not invariably lead to poor clinical outcome.
Conclusion:
Lambrinudi arthrodesis is a treatment option with favorable long-term outcome for patients with severe, fixed equinus deformities.
Introduction
Severe rigid drop foot deformity was a common sequela from poliomyelitis infection. This was due to the muscle imbalance between the ankle dorsiflexors and the plantar flexors. Many patients were left with such severe equinus that the foot formed a 180° angle with the longitudinal axis of the tibia. As a result, many patients required surgical correction of the severe equinus deformity in the teens or early 20 s. As the polio virus became eradicated from our locality, we are now left to look after a group of patients who have had surgical corrections of the post-poliomyelitis deformities many decades ago. These patients are now well into adulthood. The outcome of their past surgeries has a direct effect on their employment, their working ability, and their activities of daily living. The most common surgical procedure for severe rigid drop foot was an arthrodesis originally described by Lambrinudi in 1927 1 and subsequently modified by himself and others. 2,3 In cases of severe drop foot in which the ankle joint is in maximal equinus, a wedge of bone is removed from the plantar–distal surface of the talus. The resultant triangular beak at the distal end of the talus is wedged into a notch created in the navicular and the subtalar joint in a relatively calcaneus position. Finally, the calcaneocuboid joint is fused in the usual manner. This allows the ankle joint to remain in equinus while bringing the forefoot into a plantigrade position (Figure 1). 2 It is widely regarded as a variant of triple arthrodesis in the correction of equinus feet.

Technique for Lambrinudi arthrodesis. Source: by Lambrinudi. 2 [Adapted with permission from the publisher].
This study was conducted to review the long-term outcomes of patients who have had this type of triple arthrodesis in their teens and early 20s. Information gathered included the complaints reported by the patient, including symptoms from adjacent joints, their activities of daily living, and their working ability.
Materials and methods
We gathered, retrospectively, our records from 1970 to 1980 of all patients who had received a Lambrinudi arthrodesis in our center, the Duchess of Kent Children’s Hospital. A total of 16 records of patients with Lambrinudi arthrodesis was found. Of those, 10 patients, with a total of 11 feet, had sufficient long-term follow-up information to be analyzed. Four patients were called back to be assessed at our own clinic, while the other six patients had data documented by other orthopedic surgeons on the Clinical Management System of the Hospital Authority of Hong Kong for analysis. The outcome grading as described by MacKenzie 4 in his 1959 paper was used to gauge the long-term outcome of the patients (Table 1). 4 This outcome grading was used as it was widely published and utilized by other authors in previous published studies examining the same operation including Tang et al. 5 and Bernau 6 and allows for comparison to be made with these studies.
MacKenzie’s classification 1957.

Source: Mackenzie. 4
Results
Of the 10 patients, eight had deformities due to poliomyelitis (see Table 2, for summary of results). One patient had a diagnosis of Kugelberg Welander spinal muscular atrophy and one had recurrent clubfoot deformity associated with spina bifida. The patient with spinal muscular atrophy had Lambrinudi arthrodesis to both feet. The average follow-up was 36.6 years (27–41 years). Two patients were female; the remaining were male. The average age of the patients at the time of surgery was 15.5 years old (14–24 years old).
Summary of outcome.

Planned and staged procedures were performed in five patients. These included three patients who had tibial derotation osteotomies and two patients who had Anderson lengthening of the tibia for significant leg length discrepancy. The case of patient 2 is illustrated in Figure 2(a) to(f.) Three patients required unplanned remedial surgeries for residual deformities. Patient 1, with post-poliomyelitis deformity, had insufficient correction of the foot equinus after the Lambrinudi arthrodesis. He required further posterior ankle release and midfoot dorsal closing wedge osteotomy 2 months later. Patient 3, with sacral level spina bifida, had recurrent clubfoot deformity and hindfoot varus. She required lateral column shortening surgery 16 years after the Lambrinudi arthrodesis. She then received a redo of the subtalar fusion 3 years after the second surgery due to residual hindfoot varus. Patient 10 with spinal muscular atrophy had residual right hindfoot varus during swing phase of walking and received a tibialis posterior transfer 1 year after the Lambrinudi arthrodesis.

Patient 2 [with informed consent obtained]. (a) Preoperative clinical photo: left leg shortening and severe equinus posture of left foot. (b) left tibia derotation osteotomy and Achilles tenotomy. (c) Lambrinudi arthrodesis 1974. (d) Anderson lengthening 1975. (e) left foot standing X-ray 2013: plantigrade foot, adjacent ankle joint arthrosis, adjacent tarsal arthrosis with dorsal lipping at navicular-cuneiform joint, talar flattening and solid union. (f) lower limb clinical photo 2013.
As mentioned, the outcome grading as described by MacKenzie 4 was used to categorize our patients’ long-term outcome. The outcome parameters included the presence of pain, instability, limitation in activity, abnormal gait, need for special shoes, residual deformity, symptomatic callosities, and successful fusion of all joints. The outcomes were classified as “ideal,” “good,” “fair,” and “failed”.
There were four patients who had “good” outcome, three with “fair” outcome, and two with “failed” outcome. Overall, the failure rate was 2 of 10, while 7 of 10 patients achieved a good or fair outcome. The patient with spinal muscular atrophy had progressive lower limb weakness resulting in worsening gait and eventually became wheelchair-bound 15 years after the surgery; however, he did not complain of any pain or problems in his feet before he died of sepsis at the age of 49. Another patient died at the age of 53 of acute myocardial infarction, 33 years after the Lambrinudi arthrodesis, but had no pain or discomfort in the lower limb at the time of his death.
We investigated the radiological outcome of our patients (Table 3). We were unable to contact three of the patients and two passed away by the time of this study. All in all, we were able to review the follow up X-rays of 5 of the 10 patients taken within the last 5 years, representing X-rays taken ranging from 33 years to 41 years after the operation. None of our patients had pseudoarthrosis; X-rays of all five patients demonstrated solid union of subtalar, calcaneo-cuboid, and talo-navicular joints. All five patients showed signs of talar flattening, attributed by Ingram and Hundley 7 to possible avascular necrosis of the talus.
Summary of radiological findings.

Patient 8’s latest X-ray was not a standing lateral X-ray.
All of these five patients demonstrated radiological changes of ankle arthritis and tarsal arthritis. We define ankle arthritis based on the presence of subchondral sclerosis, subchondral cyst, joint space narrowing, and osteophyte formation. Similarly, tarsal arthritis is defined with attention paid to the presence of dorsal lipping, as described in MacKenzie’s paper. 4 Ankle arthritis was graded further based on Takakura staging. 8 Takakura et al. classified ankle osteoarthritis into four stages based on weight bearing X-rays of the ankle, where stage 1 means no joint space narrowing, early sclerosis and osteophyte formation; stage 2 means narrowing of medial joint space; stage 3 means obliteration of medial joint space and subchondral bone contact; and stage 4 means obliteration of the entire tibio-talar joint space. 8 In our series, one patient was Takakura stage I, three were Takakura stage III indicating advance arthritis, while the remaining one did not have a true anteroposterior view of the ankle for commenting on Takakura staging. Despite the presence of radiological arthritis, only two patients had clinical ankle pain. Similarly, despite the presence of tarsal arthritis in these five patients, there was no documentation of significant midfoot pain in any of them.
We attempted to objectively evaluate the correctional power of the arthrodesis by measuring the tibiometatarsal angle (TM angle) as described by Tang 5 ; this is the angle formed between the extrapolation of the axis of the first metatarsal and that of the tibia (see Figure 3). 5 In our series, the average correction in the TM angle was 69° (range 33°–100°). In three of the five patients, the latest TM angle measurements were noted to be similar or even less than the early postoperative X-rays, taking into account intra- and interobserver error. In two patients, a loss of correction was noted, but only one of them had a loss of correction of greater than 10°. This patient also had a poor outcome by MacKenzie’s classification. 4 Interestingly, one patient (patient 4) who had an 87° correction in TM angle and who maintained this correction in his latest X-ray had a poor overall outcome by MacKenzie’s classification. 4
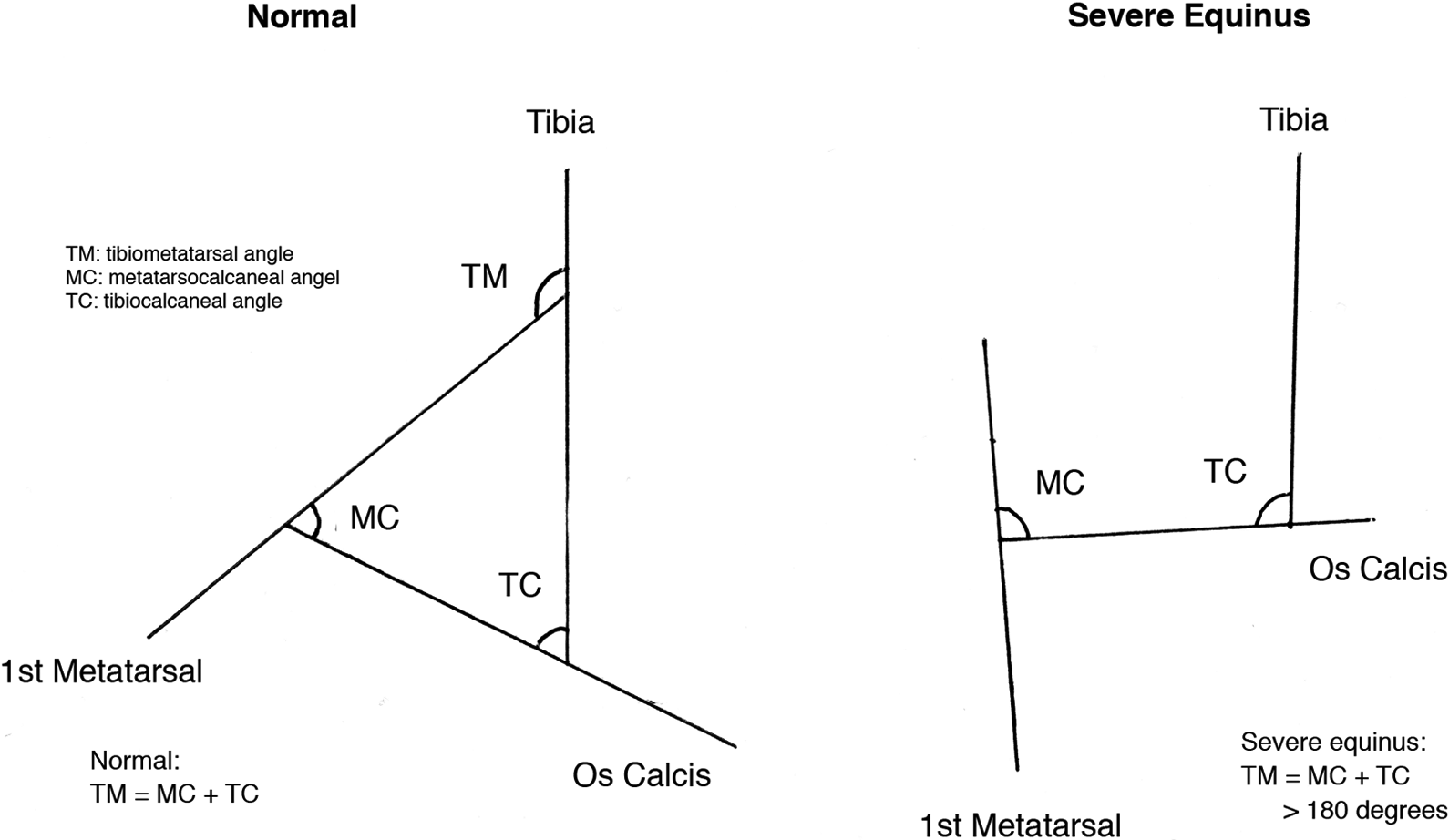
Measurement of TM angle. Source: Tang et al. 5 [Adapted with permission of the publisher].
Discussion
Our series, which had a substantially longer follow-up period than previously published results on Lambrinudi’s arthrodesis, showed that the results of the procedure were overall satisfactory. Seven of 10 of our patients maintained a fair to good outcome at an average follow-up period of close to 37 years. Most of the literature on Lambrinudi’s arthrodesis reported an average failure rate of 12.4% (range from 0% to 19%). 4,7 None of these studies have an average follow-up period of longer than 20 years. Our study demonstrated a failure rate that was not substantially higher than MacKenzie’s 4 (19%) or Bernau’s 6 (16%) results, both of which had relatively long follow-up periods. This suggests that even with the passage of time, the Lambrinudi arthrodesis can maintain fairly good results in the long run.
Lambrinudi’s original description of his triple arthrodesis was for rigid equinus deformity of the foot due to poliomyelitis. These deformities tend to do poorly with conventional triple arthrodesis surgeries historically. In a retrospective review of 80 feet with deformities by Angus and Cowell, 9 for which triple arthrodesis operations were performed using a variety of techniques (majority being Ryerson −61 of 80 and only five Lambrinudi), he found that of the 26 rigid equinovarus deformities, only nine had fair to good results. The majority (17 of 26, i.e. 65%) had poor results. Furthermore, 14 of 26 (56%) patients had problems with residual deformity. Although he did not specify the corrective power of each individual technique, the overwhelmingly poor results illustrate that patients with rigid equinovarus need a unique and dedicated technique rather than the conventional operative treatment for treatment of their condition.
In contrast, our present study demonstrated fair to good results in the majority of patients. Furthermore, while 4 of the 10 patients had residual clinical deformities, two of them still enjoyed a fair outcome. This may also suggest that having residual clinical deformity does not imply poor outcome.
When we look at patients with poliomyelitis as a group, the results were also satisfactory. Mackenzie looked at 61 patients, of which 80% had fair to good results. 4 Patterson et al. looked at 35 feet with poliomyelitis and 85% had fair to good results. 10 Our study showed that six of the eight polio patients had fair to good results. From both the literature and our own results, the Lambrinudi triple arthrodesis appears to be a reliable procedure in polio patients.
Rigid versus flexible deformity
The correctional power of Lambrinudi triple arthrodesis in fixed equinus deformity has been demonstrated in multiple previous studies. Patterson et al. 10 reviewed 55 cases of Lambrinudi arthrodesis, of which the most common deformity was fixed equinus and the majority of their patients had poliomyelitis. They found that 30 patients had good correction, 20 had partial correction, and only 5 (9%) had a poor correction. MacKenzie’s 4 analysis showed that patients with fixed equinus had very good results with 92% cases out of 51 fixed equinus feet having fair to good results. Bernau’s 6 study included 11 fixed equinus feet, where six cases had good outcome and one case had a fair outcome. Although the results in flexible drop foot have been mixed, the results in fixed equinus deformity have been in favor of Lambrinudi procedure.
Radiological outcome
Our study shows that the Lambrinudi arthrodesis has an excellent union rate. With regard to corrective power, a previous study by Tang et al. 5 already demonstrated that Lambrinudi triple arthrodesis gave remarkable corrective power of up to 47° in patients with very severe equinus deformities. The correction in TM angle in our series approaches an average of 69° in four patients. However, the clinical relevance of TM angle must be interpreted with caution. In our patients, the achievement or maintenance of correction of the TM angle did not necessarily correlate with clinical outcome. This is evidenced by the patient with a poor outcome despite excellent radiological improvement and the patient with a fair outcome despite loss of reduction. The measurement of TM angle is not without limitations as it requires a true standing lateral X-ray of the ankle. This would be difficult in the postoperative setting as patients would not be allowed to weight bear until the osteotomies have healed. Hence, the comparison of TM angles for assessment of correction achieved and maintenance is difficult to utilize in practical setting. That radiological deformities do not correlate with clinical deformity or outcome also cautions against overreliance on measuring the TM angle as an indicator of surgical success.
Predictors of poor outcome
Looking at the relationship between development of adjacent joint arthritis and clinical outcome, we observed that while both of the two failed cases had radiological adjacent joint arthritis, all three patients with “fair” outcome also had adjacent joint arthritis. With reference to studies of larger sample size, Bernau 6 ‘s study of 50 feet had 15 cases of ankle arthritis but only 3 had a failed result (20%). MacKenzie’s 4 review of 100 feet found only 7 cases of anterior tarsal joints arthritis and 15 cases of ankle arthritis (22% in total); 6 of these 22 patients had poor outcome (27%). This seems to suggest that having adjacent joint osteoarthritis alone does not invariably predict a poor outcome.
Other complications reported in the literature such as ankle instability, painful callosities are also observed in our study. However, the incidence of ankle instability is low (1 of 10) with reference to the existing literature (Bernau 6 14% and MacKenzie 4 24%). The most common complication is the development of painful callosities, which is present in 4 of 10 of our patients. This is comparable to a study of similar scale by Tang et al. 5 (50%) and a much larger study by MacKenzie 4 (45%). None of our patients with good outcome had painful callosities, but both patients with failed outcome did. This suggest that painful callosities may be a strong predictor of poorer outcome.
Do all the above results translate into patient satisfaction? The literature seems to suggest so. Patterson’s 55 feet series showed that patients’ own evaluation of the procedure was largely in favor of the procedure with 46 patients feeling pleased with the results (83%). 10 Similarly, Mackenzie’s study 4 found that patients’ own grading was not very different from surgeons’ grading of outcome, with fair to good results in as much as 81% cases. 4 Bernau’s study noted that patient’s grading was even more positive than that of surgeons. 6
There are several limitations to our study. We had a very small sample size of 10 patients and only 5 of 10 patients had updated and good quality X-rays for analysis. This was because two of the patients had died by the time the study was undertaken, and we were unable to get in touch with the remaining three patients due to missing contact information. This is a retrospective study over a long span of time and the assessment of precise range of motion and muscle power were not well-documented in medical records for analysis. Furthermore, we do not have a control group to compare with. In particular, it is not possible to establish a comparison with conventional techniques of triple arthrodesis for lack of a control group.
The strength of our study is the length of follow-up which averages 37 years. Patients who require Lambrinudi arthrodesis often received their surgery in their adolescent years and the outcome three decades later remains pertinent to their activities of daily living, occupation, and quality of life. The results of our study suggest that a favorable outcome is sustainable even after many years and thus is relevant to clinicians who are planning for surgical correction of severe, rigid equinovarus foot deformities in patients with neuromuscular disorders.
Conclusion
Poliomyelitis patients require surgery very early in their lives and subsequently have a very long follow-up. Most of them lead full and productive lives. Our findings demonstrate that after nearly 37 years, the outcome is still largely favorable. A review of the literature also shows Lambrinudi to be a reliable choice especially for polio patients with fixed equinus deformities both in terms of subjective evaluation of outcome and in terms of deformity correction. Although the incidence of severe equinus deformities typically due to poliomyelitis and neglected clubfeet is in the decline, we occasionally still see patients referred from developing areas with neglected deformities. We therefore recommend the Lambrinudi arthrodesis as a good option for the correction of such severe, fixed equinus deformities.
Footnotes
Acknowledgments
The authors would like to acknowledge Professor John Chi Yan Leong for inspiring and contributing to our study. Professor Leong was one of the co-authors of the article “Lambrinudi triple arthrodesis for correction of severe rigid drop-foot” published in 1984 [J Bone Joint Surg Br 1984; 66-B: 66-70], which examined patients who have received Lambrinudi triple arthrodesis from our center about 30 years ago.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.