
Abstract
Background:
The association between tuberosity cysts and rotator cuff tears (RCTs) and the nature of the major contributing factors to tuberosity cyst formation continue to be controversial. The purpose of our study was to evaluate the strength of associations of RCT and various factors involved in the chronicity of RCT with tuberosity cysts, using magnetic resonance imaging (MRI) and radiographs.
Methods:
We reviewed consecutive patients with various disease entities between August 2004 and July 2013. After excluding unsuitable patients, this study involved 1007 shoulders of 906 consecutive patients. Each tuberosity cyst was categorized as an anterior greater tuberosity (GT), posterior GT, lesser tuberosity, and bare-area cyst. The odds ratios (ORs) and 95% confidence intervals (CIs) between the tuberosity cysts and various factors were evaluated by logistic regression analyses; p-value was set below 0.05.
Results:
Anterior GT cysts and posterior GT cysts on MRI or anterior GT cysts on radiographs were significantly associated with supraspinatus tendon (SST) tears ( p ≤ 0.019) and infraspinatus tendon (IST) tears (p ≤ 0.004). Among the shoulder pathologies, RCTs only significantly associated with cyst formation (OR 4.23, 95% CI 3.17–5.65; p < 0.001). The retraction grade of Patte was significantly associated with anterior GT cyst (OR 3.65, 95% CI 2.42–5.48; p < 0.001).
Conclusion:
Detecting an anterior GT cyst in a radiograph, even a low prevalence, in a patient with symptomatic shoulder indicates a need to consider RCT, especially of the SST, IST, and a high possibility of a retracted tear.
Introduction
Humeral tuberosity cysts are a common finding known to be related to rotator cuff tear (RCT) or to aging, according to the location of the cyst. 1 –6 However, normal shoulders also have cysts in the humeral tuberosities. 3,5,7 Some studies have examined the relationship of the locations of these tuberosity cysts with RCT. 2,6,8,9 It has been suggested that the presence of cysts within the anterior aspect of the greater tuberosity (GT) and of the lesser tuberosity (LT) has a high specificity for, respectively, supraspinatus tendon (SST) tear and subscapularis tendon (SBT) tear. It has been reported that cysts within the posterior aspect of the GT are common in asymptomatic shoulders. 10 However, most studies evaluating tuberosity cysts are magnetic resonance imaging (MRI) studies. No study has suggested the significance of cyst using the strengths of associations between tuberosity cysts and RCT using the two different imaging modalities of MRI and radiograph.
The etiology of these cysts has not yet been completely determined. Microavulsive cuff tears may induce an inflammatory reaction, resulting in synovial fluid entering the cysts through small communicating pores on their surfaces. 1 These tears may be secondary to contact between the bone underlying the cuff tear and the coracoacromial arch. Alternatively, the developmental theory proposes that, because the incidence of tuberosity cysts in asymptomatic shoulders ranges from 15% to 45%, the occurrence of these cysts is unrelated to aging or to the underlying shoulder pathology. 1,6,10 No study has evaluated the risk factors contributing to the formation of tuberosity cysts, using various indexes involved in the chronicity of RCT.
The hypothesis of this study was that tuberosity cyst seen in radiograph can give some referral information to expect RCT. The primary purpose of the current study was to evaluate the strengths of associations of tuberosity cysts with RCT, using the two different imaging modalities of MRI and simple radiograph. The secondary purpose was to evaluate the strength of associations between the tuberosity cysts and shoulder pathologies, including the chronicity of RCT.
Materials and methods
We reviewed consecutive 1305 shoulders belonging to 1181 patients between August 2004 and July 2013 on outpatient clinic visitors who complained of shoulder problems including instability, limitation of motion, weakness, and intolerable pain. Enrolled patients were fulfilled with the series of radiograph and MRI of the shoulder, recorded medical history, and records of physical examination of the shoulder. For each shoulder, the MR images and radiographs were taken within 1 week from each other. Of those, 298 shoulder MR images were excluded for the following reasons: There was no accompanying full set of simple shoulder radiographs (123 shoulders); there was a history of prior shoulder surgery (68 shoulders) or previous trauma (37 shoulders), or there was a bony abnormality due to previous infection (15 shoulders), severe degenerative arthropathy (11 shoulders), malignant lesion (13 shoulders), or fracture (31 shoulders). This study evaluated the MR images and radiographs of the remaining 1007 symptomatic shoulders belonging to 906 consecutive patients with various disease entities. The overall mean age of the patients was 53.4 ± 11.3 years. The mean age of the 582 male patients (57.8%) was 53.2 ± 11.2 years; the mean age of the 425 female patients (42.2%) was 53.6 ± 11.4 years. This study was approved by the Institutional Review Board of the current authors’ hospital (GNUH 2013-06-001).
Each full set of simple shoulder radiographs included true anteroposterior view, supraspinatus outlet view, and shoulder axillary lateral view. The following MR images were taken for all patients: T1-weighted images (repetition time [TR]/echo time [TE] = 510/11 ms) and T2-weighted images (TR/TE = 3000/48 ms), both including axial, oblique coronal, and oblique sagittal views obtained at 3-mm-thick section (1.5-T MR imager, Avanto; Siemens, Erlangen, Germany). Cystic change on MR images was defined as a round or an oval lesion in tuberosities or in the bare area of the humerus, with a diameter of more than 2 mm, a low signal intensity on T1-weighted images, and a high signal intensity on T2-weighted images. 2 When such a round or an oval lesion was observed in at least two different angles of image, we accepted it as a cystic lesion. The cyst-like lesions that were connected to tubular structures on sequential images were recognized as vascular channels and, as such, were excluded from our study. 11 Cystic change on simple radiographs was defined as a round or an oval, discrete, radiolucent lesion with a well-defined margin larger than 3 mm and located in the subcortical or cortical area of the tuberosities and the bare area of the humerus (Figure 1). The tuberosity cysts were divided into three groups: GT, LT, and bare-area cysts. 6 The GT cysts were further divided into anterior and posterior tuberosity cysts, according to their locations relative to the midline of the GT. 2 In MR images, the cyst location was defined using axial, oblique coronal, and oblique sagittal T1- and T2-weighted images. In simple radiographs, locations of the cysts were determined using the sclerotic borders of tuberosities in true anteroposterior views, axillary lateral views, and supraspinatus outlet view. The presence and location of each cyst were determined by an orthopedic surgeon (JYG), and the integrity of RCT was evaluated by a musculoskeletal radiologist with 20 years of experience independently. Two examiners carried out the measurements independently three times, with 2-week intervals between the sessions. The κ statistic was used to analyze intraobserver and interobserver agreement of cysts. 12 Diagnosis of both partial- and full-thickness RCTs was determined using MRI findings. To differentiate SST and infraspinatus tendon (IST) on GT on MR images, we used an imaginary line drawn from the anterior margin of the infraspinatus muscle which links to the conjoined tendon on the GT in sequential sagittal images. This radiologist also diagnosed and evaluated various shoulder pathologies, including injuries of the labrum or of the biceps tendon, arthritides of the glenohumeral joint or of the acromioclavicular joint, and calcific tendinitis.

(a
We calculated the odds ratios (ORs) and 95% confidence intervals (CIs) to evaluate the strengths of associations between the presence of tuberosity cysts and various shoulder pathologies, including RCT. We also evaluated the strengths of associations between these cysts and various factors involved in the chronicity of RCT, including the fatty infiltration index, muscle atrophy indexes, the degree of tendon retraction, and tear length and width. A biostatistician, who did not participate in the image interpretation, performed the statistical analyses, using forward stepwise logistic regression analysis. First, we performed univariate logistic regression analyses for all variables; then, we performed a multivariable logistic regression analysis, using only the significant variables that had resulted from the univariate analyses. Multivariable logistic regression analysis was performed after the assessment of multicollinearity, using factors with a variance inflation factor (VIF) and a condition index. We considered both VIF and a condition index of less than 10 among the variables indicating the absence of multicollinearity. 13 Hosmer–Lemeshow test was used to determine the goodness of fit for the multivariable logistic regression model. The significance of the logistic analyses was set at p < 0.05, and the significance of the Hosmer–Lemeshow test was set at p > 0.05. Statistical analysis was processed using SPSS 20.0 for Windows (IBM Corp., Armonk, NY, USA).
Results
Tuberosity cysts were detected by MRI in 71.0% of our patient group and by radiograph in 4.2%. Of the tuberosity cysts detected by MRI, the highest prevalence was of bare-area cysts, followed by anterior GT cysts, LT cysts, and posterior GT cysts. Of the tuberosity cysts detected by radiograph, the highest prevalence was of anterior GT cysts, followed by LT cysts, posterior GT cysts, and bare-area cysts. Prevalence of tuberosity cysts by location are summarized in Table 1.
Prevalence of tuberosity cysts by location; strengths of associations between cyst locations and sex and between cyst locations and the affected side.

OR: odds ratio; CI: confidence interval; MRI: magnetic resonance imaging; GT: greater tuberosity; LT: lesser tuberosity.
aAdjustment was made using rotator cuff tear factor.
Intraobserver agreement for the detection of the locations of cysts was fair to good (κ values: 0.53–0.75), and interobserver agreement for the detection of the locations of cysts was fair to good (κ values: 0.58–0.65; Table 2).
Intraobserver and interobserver reliability in the detection of cysts.a

GT: greater tuberosity; LT: lesser tuberosity.
aA value of 0.40 or less was interpreted as poor; 0.41–0.59, fair; 0.60–0.74, good; and 0.75 or greater, excellent.
Gender and affected side were not statistically significantly associated, on either MRI (p ≥ 0.243) or on radiographs (p ≥ 0.127), with the cyst prevalence at any of the four different locations (Table 1). Our evaluation indicated a high strength of associations between age and the overall prevalence of RCT (OR 1.78; 95% CI 1.27–2.32; p < 0.001). We also found significant associations between age and each RCTs: SST (OR 2.23, 95% CI 1.21–3.47); IST (OR 1.91, 95% CI 1.13–2.81); and SBT (OR 1.07, 95% CI 1.04–1.11; p ≤ 0.018). Age was significantly associated with four different locations of cyst on MRI and anterior and posterior GT cysts on radiograph (p ≤ 0.025). We performed a multivariable analysis to adjust for a confounding factor, RCT, in relation to the age factor. In those adjusted multivariable analyses, LT cysts (p < 0.001) and bare-area cysts (p = 0.013) were significantly associated with age on MRI, whereas none of the tuberosity cysts at the four different locations were significantly associated with age on radiographs (p ≥ 0.056; Table 1).
Logistic regression for the association between RCT and cyst location showed significant results of anterior GT, posterior GT, and LT cyst on MR and anterior GT cyst on radiograph with SST (p ≤ 0.007); of anterior and posterior GT cyst on MRI and anterior GT cyst on radiograph with IST (p < 0.001); and of none of the cyst on MR and radiograph with SBT (p ≥ 0.151). We performed multivariable logistic regression analyses, which included age as a confounding factor, to evaluate the direct association between anterior and posterior GT cysts and posterosuperior cuff tear. After adjustment, SST showed a significant association with anterior and posterior GT cysts on MRI and anterior GT cyst on radiograph (p ≤ 0.019). IST showed a significant association with anterior and posterior GT cysts on MRI and anterior GT cyst on radiograph (p ≤ 0.004). None of the cysts on MRI or radiographs at any of the four locations were significantly associated with SBT. Strengths of associations between RCT and cyst locations as detected in MRI or radiograph are summarized in Table 3.
Strengths of associations between rotator cuff tendon tear and cyst location as detected in MRI or radiograph.

MRI: magnetic resonance imaging; CI: confidence interval; GT: greater tuberosity; LT: lesser tuberosity.
aAdjustment was performed using the age factor.
Of the studied shoulder pathologies, which were labral injury, acromioclavicular joint arthritis, biceps tendon injury, subacromial osteophyte, osteoarthritis of the glenohumeral joint, calcific tendinitis, and RCT, RCT showed the highest prevalence of cyst formation (82.8%). In univariate logistic regression analyses, only RCT (OR 4.23, 95% CI 3.17–5.65) showed a significant association with tuberosity cyst (p < 0.001; Table 4).
Strengths of associations between the cyst formation and various shoulder pathologies as found in MRI.

MRI: magnetic resonance imaging; CI: confidence interval.
The results for the evaluation of the strength of association between the anterior GT cysts on MR and various factors involving the chronicity of RCT were as follows. Patte grade, tear length, tear width, global fatty degeneration index, and occupational ratio’s grade were significantly associated with anterior GT cysts in a univariate analysis (p ≤ 0.017). However, only Patte grade (OR 3.65, 95% CI 2.42–5.48) was significantly associated with anterior GT cyst in a multivariable analysis (p < 0.001). This last result indicates that the more retracted the tears, the higher the association strength with anterior GT cysts. Strengths of associations between the factors for RCT chronicity and anterior GT cyst formation are summarized in Table 5.
Strengths of associations between factors for rotator cuff tear chronicity and anterior GT cyst formation.a
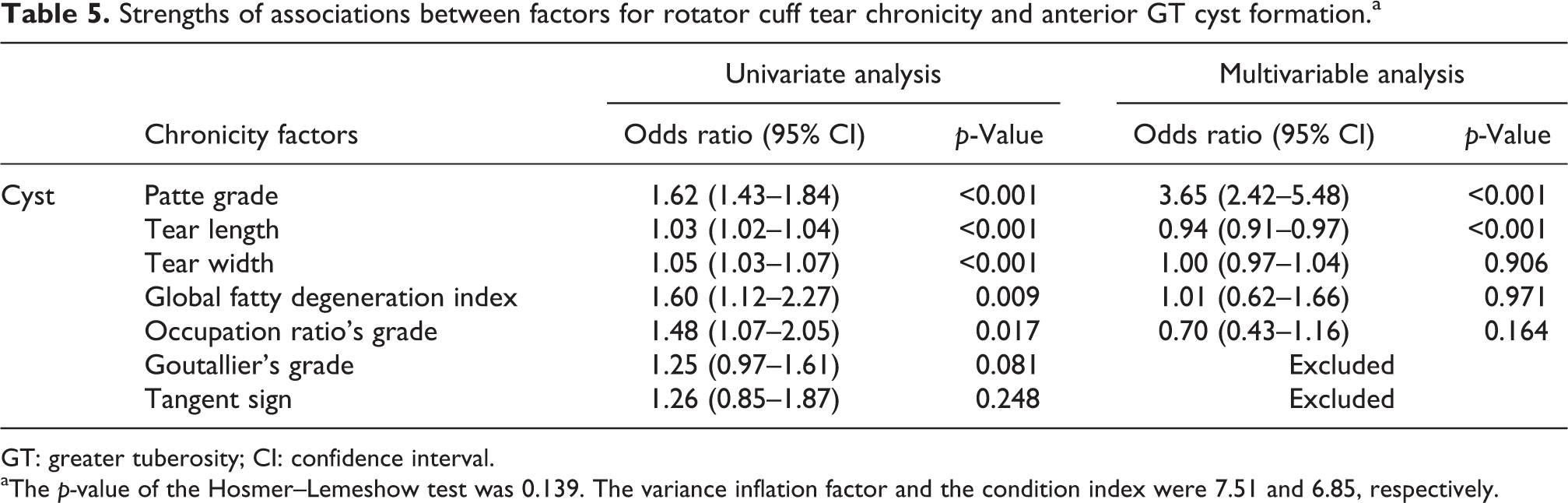
GT: greater tuberosity; CI: confidence interval.
aThe p-value of the Hosmer–Lemeshow test was 0.139. The variance inflation factor and the condition index were 7.51 and 6.85, respectively.
Discussion
The primary questions related to tuberosity cysts pertain to their associations with age and RCT and to their etiology. This study demonstrated that bare-area and LT cysts are significantly associated with age, and anterior GT cysts are significantly associated with SST or IST in symptomatic patients. Anterior GT cyst is significantly associated with the retraction degree of torn supraspinatus tendon.
In the current study, the incidence of tuberosity cysts was the highest in the bare area, followed by the anterior GT area. Most studies reported that cysts of the posterior GT are more common than those of the anterior aspect of GT. 2,6,9 The one exception, a study by Suluova et al., 14 reported that anterior GT cysts are the most common cysts. The current study’s results are similar to those of previous studies. Sano et al. 6 reported that the bare area was the most common of the four different tuberosity cyst locations, with which our findings agree. Williams et al. 9 and Fritz et al. 2 reported a higher incidence of posterior GT cysts than of anterior GT cysts. However, those two studies did not differentiate the posterior aspect GT cysts into posterior GT cysts and bare-area cysts.
This study demonstrated that the cysts detected on MRI in the four different locations were significantly associated with age in symptomatic patients. However, the anterior and posterior GT cysts were not associated with age after adjustment for the RCT factor; therefore, those cysts were secondarily associated with age through the RCT, the frequency of which increases with age. Sano et al. 6 reported, similarly to the current study, that the incidence of bare-area cysts increased with age more significantly than the incidence of cysts at other locations. RCT was significantly more common in the aged patients in this study and in the epidemiological studies. 15 –17 Therefore, RCTs were directly associated with anterior and posterior GT cysts. This inference is supported by the finding that age was not significantly associated with GT cysts after adjustment for the RCT factor. Several studies have reported that tuberosity cysts are not related to age. However, those studies did not evaluate the posterior aspects of cysts to differentiate posterior GT cysts from bare-area cysts. Therefore, the authors of the current study believe that the difference between the current study and those studies arises from the different classifications of the posterior aspects of GT cysts.
The most topical issue related to tuberosity cysts is their association with RCT. The current study demonstrated that anterior and posterior GT cysts on MRI and anterior GT cysts on radiographs have significant associations with SST and IST. Anterior GT cysts are significantly associated with SST and IST. The ORs of anterior GT cysts on radiograph for SST and for IST were 11.43 and 7.71, indicating the very high strength of associations, as compared to the known risk factors of other diseases. 18 –20 These results are similar to the findings of previous studies, 2,6,14 with one exception. 9 Williams et al. 9 reported no significant association between tuberosity cysts and RCT. That study clearly stated that posterior GT cysts were not related to RCT, but it did not exclude the possibility of a relationship between anterior GT cysts and RCT. That possibility, which did not reach statistical significance, interests us. We attribute the differences between the findings of the study by Williams et al. 9 and of the current study to differences in the classification of cyst locations and in the methods of statistical analysis. We found that anterior GT cysts on radiographs are a very useful sign to suspect SST or IST with patients who have shoulder pain. In actual clinical practice, our findings are more useful to a physician studying a radiograph than to a physician studying an MRI, although the ORs of anterior GT cysts are high with both tools. The diagnostic values of anterior GT cysts on radiograph are summarized in Table 6. Because of their high positive predictive value (95.0%), likelihood ratio (15.4), and posttest probability (82.9%), GT cysts on plane radiograph, in combination with shoulder pain, are a diagnostic finding that rules in RCT. 21
Diagnostic accuracy of anterior GT cyst for the detection of supraspinatus tendon tear.

GT: greater tuberosity; MRI: magnetic resonance imaging.
The current study could not demonstrate a significant association between LT cysts and SBT. Prior studies have reported different degrees of relationship between the two. 6,22 –24 Regardless of the findings reported by the prior studies, those studies differed in statistical design from the current study. Two prior studies compared the frequency of LT cysts in SBT groups and in normal SBT groups, using χ 2 tests. 6,9 In one of those studies, Sano et al. 6 reported that LT cysts were all related to massive RCT and, therefore, closely related to SBT. By contrast, in the other of those two studies, Williams et al. 9 reported no significant relationship between LT cysts and SBT. Studler et al. 22 analyzed the diagnostic accuracy of using LT cysts on MRI to detect SBT; that study reported that LT cysts on MRI are relatively specific for SBT. Wissman et al. 23 reported the fine distinction that SBTs were significantly more common in the group having cysts within the LT than in the group having cysts adjacent to the LT. However, none of these earlier studies evaluated the direct association between LT cysts and SBT. We believe that these differences arise from differences in study designs and applications of statistics.
The current study suggested that the grade of tendon retraction was significantly associated with anterior GT cyst. Of the several factors related to RCT chronicity on which we performed multivariable analysis, only Patte grade was significantly associated with the anterior GT cyst. Although tear length is a variable similar to Patte grade, it was not significantly associated with the anterior GT cyst in that analysis. Even though there was no multicollinearity between Patte grade and tear length (VIF = 5.86 and condition index = 2.79), the high correlation between those two factors (ρ = 0.952) did not allow us to rule out the possibility of a modified effect of the interaction between the two. 25 Receiver operating characteristic curves used to evaluate their accuracy in predicting the presence of anterior GT cysts showed an area under the curve of 0.70 for Patte grade and of 0.68 for tear length, indicating greater accuracy for Patte grade than for tear length (Figure 2). The difference in these similar areas arose from the characteristics of the two variables; one involved ordinal values and the other involved continuous values. Therefore, we concluded that the retraction grade of a torn supraspinatus tendon is a significant factor for anterior GT cyst formation.

ROC curves for both Patte grade and tear length were made to evaluate their accuracy in predicting the presence of anterior GT cysts. The area under the ROC curve for Patte grade was larger than that for tear length, indicating a greater accuracy for Patte grade. ROC: receiver operating characteristic; GT: greater tuberosity.
The first limitation of this study is that we did not use MR arthrography. Therefore, we could not determine whether the cysts communicate with joint space. The second limitation is that our study is a cross-sectional study, not a longitudinal study. Our data showed the association between tuberosity cyst and RCT. We could not explain whether tuberosity cyst is the cause or result of the RCT. The last limitation is that we did not include cyst of an asymptomatic shoulder. To find the association between the cyst and the RCT, we created a control group of patients with diagnoses other than RCT within our cohort.
Detecting an anterior GT cyst in a radiograph, even a low prevalence, in a patient with symptomatic shoulder indicates a need to consider RCT, especially of the SST, IST, and a high possibility of a retracted tear.
Footnotes
Acknowledgments
The authors express their gratitude to Hyun-Su Yang for the statistical aspects and Pil Yeob Choi and Jae-Boem Na for the radiological aspects of this project throughout the entire process.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.