
Abstract
Purpose:
The purpose of this study was to investigate the clinical results of arthroscopic rotator cuff repair in patients with anterior greater tubercle cyst in magnetic resonance imaging (MRI).
Methods:
The cyst-present group comprised 38 patients with anterior greater tubercle cyst in MRI, and age- and sex-matched 30 patients without cyst in humeral head were included in the control group. The cystic group was divided into two groups, smaller than 5 mm (21 patients) and larger than 5 mm (17 patients), according to the cyst size. A total of three groups were created. In the evaluation of clinical outcomes, modified University of California at Los Angeles (UCLA) and the Western Ontario Rotator Cuff Index (WORC) were used. The visual analog scale (VAS) was used to assess pain. One-way analysis of variance was used to compare VAS, UCLA, and WORC scores among the groups.
Results:
There was a statistically significant difference in the clinical results of VAS, UCLA, and WORC among the cystic and noncystic groups in the anterior greater tubercle (p < 0.05). There was also a statistically significant difference in the clinical results of UCLA, WORC, and VAS scores according to the cyst sizes in the anterior greater tubercle cyst group (p < 0.05).
Conclusion:
Anterior greater tubercle cysts have negative effects on rotator cuff repair results. If the anterior greater tubercle cyst size is greater than 5 mm, the negative effects of rotator cuff repair results are more pronounced. An understanding of anterior greater tubercle cysts has a critical importance for rotator cuff surgery planning.
Introduction
Humeral head cysts are common pathological changes that are being increasingly reported in the literature. 1 –5 It is unclear whether these cysts are age related, developmental, occur in asymptomatic patients, or are specific to rotator cuff pathology. A radiographic study of patients with symptomatic and surgically documented rotator cuff tears has shown a positive correlation with greater tubercle cysts. 5 In the studies reported, there was no cyst in the anterior greater tubercle in asymptomatic subjects without a rotator cuff tear. 5 –7
Humeral head cysts are classified as greater tubercle and lesser tubercle cysts. Cysts located in the lesser tubercle are rare and indicative of subscapularis and supraspinatus tendon abnormalities. 8 The greater tubercle cysts are categorized anteriorly and posteriorly in terms of their location in the tubercle. The posterior tubercle cysts are more common and associated with age and degeneration. 4,7,9 The anterior greater tubercle cysts are reported to be strongly associated with rotator cuff tears. 1,4,7 In the literature, there is a group of studies focusing on the relationship between humeral head cysts and rotator cuff tears. 1,4,5,7,8
In the diagnosis of humeral head cysts, radiological techniques such as magnetic resonance imaging (MRI), magnetic resonance arthrography, and larger cysts direct radiography are used. 1
Despite the progress of technology and surgical technique for rotator cuff repair, the desired level of success in rotator cuff repair results has not yet been achieved. 6,10 There are many factors that affect rotator cuff repair results. As far as we know, there is no study describing the relationship between anterior tubercle cysts and the results of rotator cuff repair in the past literature.
In this study, we aimed to investigate the clinical results of patients who underwent arthroscopic rotator cuff repair with the cysts in the anterior greater tubercle detected in MRI. The hypothesis is that the arthroscopic rotator cuff repair to the patients with anterior greater tubercle cysts will affect the results.
Materials and methods
Study population and inclusion criteria
Patients with prior diagnostic MRI examination and arthroscopic rotator cuff tendon repair who visited our clinic between January 2014 and June 2017 were reviewed in our study. A total of 68 sex- and age-matched patients were included in the study; among them, 38 patients complied with the criteria of our work cyst present in the anterior greater tubercle and 30 patients complied with the criteria of our work cyst absent in the humeral head. The cystic group was divided into two groups, smaller than 5 mm (21 patients) and larger than 5 mm (17 patients), according to the cyst size. A total of three groups were created. Arthroscopic and MRI findings and preoperative and postoperative clinical results were retrospectively reviewed in these patients. Rotator cuff repair: isolated supraspinatus tendon tear, partial subscapularis/infraspinatus tendon tears together with supraspinatus tendon tear, tears smaller than 3 cm, and patients with arthroscopic rotator cuff repair using two suture anchors were included in the study. Work level includes manual labor with less physical activity or sedentary physical activity. The level of sports activity was medium (static sports, such as yoga and jogging) or low (mild or no sports activities). 11 The study was a retrospective study and approved by the hospital Ethics Committee and was conducted according to the Helsinki Declaration (Kırıkkale University Faculty of Medicine; Ethics Committee Decision Number: 19/04, October 24, 2017).
Exclusion criteria
In the cystic group, patients with cysts on the humeral head except the anterior greater tubercle and patients with cysts larger than 20 mm were excluded from the study. In the noncystic group, patients with any cyst localization in the humeral head were also excluded from the study. Patients without clinical evaluation before and after the operation, supraspinatus muscle atrophy in advanced stage (the supraspinatus muscle occupation ratio <30%, described by Lim et al. 12 ), fatty degeneration (grades 3 and 4, described by Goutallier et al. 13 ), rotator cuff tendon repairs with osteoarthritis and recurrent tendon repair, and only subscapularis, infraspinatus, and teres minor tendon tears repair were not included in the study. Patients with unregulated diabetes mellitus (regulated diabetes mellitus; fasting blood glucose 80–130 mg/dl, HbA1C < 7), smokers who did not comply with the rehabilitation program, and patients with postoperative complication were excluded from the study in the postoperative period.
MRI examination and interpretation
MRI was performed with 1.5-tesla MRI device (Philips MRI Systems, Achieva Release 3.2 Level 2013-10-21; Philips Medical Systems Nederland B.V., Eindhoven, the Netherlands) using the surface shoulder coil. In the examination, T1-weighted, T1-turbo spin-echo (TSE) axial, T1-TSE oblique coronal (780/15; field of view [FOV] = 14 cm; cross-sectional thickness = 3.5 mm; intersection gap = 0.4 mm; matrix, 320 × 256) and T2-weighted, T2-fast-field echo axial, T2-TSE oblique sagittal, T2-weighted fat-suppressed, T2- spectral attenuated inversion recovery axial, and oblique coronal (3400/50; FOV = 14 cm; cross-sectional thickness = 3.5 cm; intersection gap = 0.4 mm; matrix, 256 × 256) images were obtained.
Cysts were defined as being round or oval with a low signal intensity on T1-weighted images and a high signal intensity on T2-weighted images. The cysts were examined in two different pulse sequences and two different image planes in a single center. Cyst size was measured from the image where the cyst was most prominent. Two radiologists (MHŞ and Mİ) who had more than 8–9 years of experience in the musculoskeletal subject attended the study for the examination of groups. The MRI images to be examined were determined through consensus. All measurements were taken by a radiologist (MHŞ). The greater tubercle was divided into anterior and posterior by a virtual line drawn through the “12 o’clock” position with respect to the shaft of the humerus on the sagittal images (Figure 1(a)). Cysts identified as anterior and posterior to this line were defined as located in the “anterior” and “posterior” greater tubercle, respectively. Locations of anterior greater tubercle on coronal and axial planes are shown in Figure 1(b) and (c). This examination was standardized according to a previously published technique. 4,5 In the anterior greater tubercle, the cysts in the footprint were included in the evaluation of humeral head cysts. In the noncystic control group, there was no cyst in the humeral head. The cyst sizes were classified as smaller than 5 mm and larger than 5 mm (Figures 2(a) to (c) and 3(a) to (c)). In the previous literature, there is no study on the prognosis of cyst sizes. We performed this classification because we used suture anchors of 5 mm in diameter in all patients. There were one or two cysts in the group with cysts smaller than 5 mm. The total size of the two cysts was smaller than 5 mm. The time between the arthroscopic surgery and the prior diagnostic MRI was limited to 3 months.
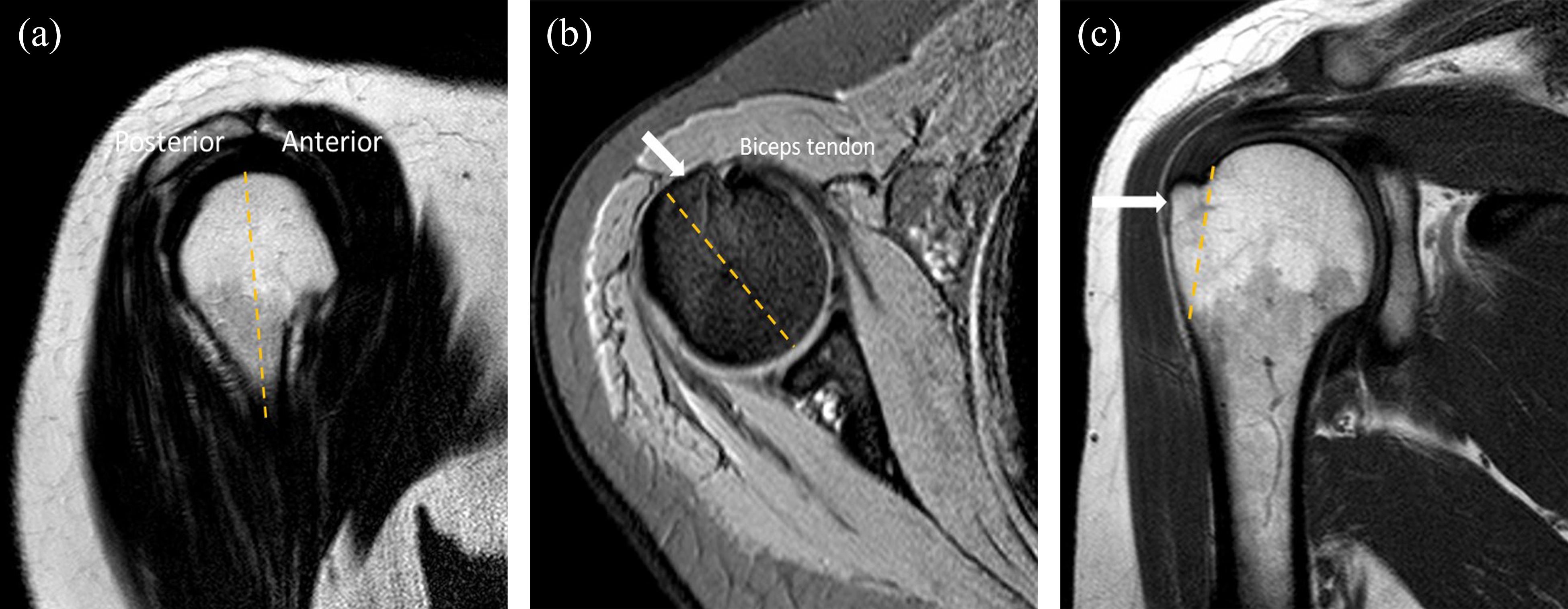
(a) T1-weighted sagittal image illustrating the division of humeral greater tubercle into anterior and posterior by the use of a vertical line drawn through the 12 o’clock position, (b) T2-fast-field echo axial image anterior greater tubercle is seen with the white arrow, and (c) T1-weighted coronal image anterior greater tubercle is seen with the white arrow.

A 50-year-old male patient; cysts less than 5 mm in size in T2-weighted fat-suppressed sagittal (a), axial (b), and coronal (c) images.

A 46-year-old female patient; cysts large than 5 mm in size in T2-weighted fat-suppressed sagittal (a), axial (b), and coronal (c) images.
Surgical technique
The patients were operated under general anesthesia and in the sitting position called the beach chair position. Initially, the acromion, distal clavicle, acromioclavicular joint, coracoid, and portals were marked with a surgical marker. The posterior portal was opened approximately 2 cm medial and 2 cm inferior to the posterolateral corner of the acromion. The anterior portal was opened approximately 2–3 cm anterior to the anterolateral corner of the acromion, and the lateral portal was opened approximately 2–4 cm lateral of the posterior to the acromioclavicular joint. An arthroscopic examination of the glenohumeral joint was performed through the posterior portal. The tear in the tendons forming the rotator cuff was fully displayed. Rotator cuff tears were assessed and were classified based on size, thickness (full or partial), and the number of tendons involved. The size of the tear was described according to the classification defined in the previously literature. 14,15 According to this system, the length of the greatest diameter was used to devise four categories of tears: small (1 cm or less), medium (1–3 cm), large (3–5 cm), or massive (>5 cm). Anterior and lateral portals were entered, and acromioplasty and subacromial bursectomy were performed with the assistance of shaver, burr, and radiofrequency. Subsequently, single-row repair was used to reconstruct the tear with two titanium suture anchors (5 mm diameter), which was fixed in the insertion. All arthroscopic rotator cuff repairs were performed by two orthopedic surgeons with 8 years of experience in shoulder surgery.
Evaluation of clinical outcomes
Evaluation of clinical outcomes was assessed at 6th and 12th months before and after the operation. The visual analog scale (VAS) was used to assess pain. 16 The VAS for pain ranges from 0 to 10, with 10 indicating the highest pain level. 16
In the evaluation of clinical and functional outcomes, modified University of California at Los Angeles (UCLA) and the Western Ontario Rotator Cuff Index (WORC) were used. The UCLA was evaluated in total of 35 pounds in five separate areas including pain (10 points), function (10 points), active forward flexion (5 points), strength (5 points), and satisfaction (5 points), with 34–35 excellent results, 28–33 good results, 21–27 fair results, and 0–20 results poorly interpreted. 16 The WORC is a health-related quality of life patient-administered questionnaire that has 21 items representing five domains, each with a VAS-type response option. The five domains are (1) physical symptoms, (2) sports and recreation, (3) work, (4) social function, and (5) emotions.
The WORC items are scored on a 100-point scale (ranging from 0 to 100). The most symptomatic score is 2100, and the best, or asymptomatic, score is 0. To present this in a more clinically meaningful format, the score can be reported as a percentage of normal by subtracting the total from 2100, dividing by 2100, and multiplying by 100. Total final WORC scores can, therefore, vary from 0%, the lowest functional status level, to 100%, the highest functional status level. 17 –19
Rehabilitation protocol
The same postoperative rehabilitation protocol was followed for all patients, including a 6-week period of immobilization with a shoulder sling. Passive limited movements were started in the 6th week and active movements in the 8th week. In the 3rd month, progressive resistance exercises limited to 1 kg were allowed. The weight restriction progressed to 2 kg in the 4th and 5th months. After 6 months, all the patients were permitted full free movement.
Statistical analysis
The level of significance was set at p < 0.05. Data were expressed as mean ± standard deviation after checking conformity to normal distribution with the Shapiro–Wilk test. Categorical variables such as genders and the distribution of groups were compared with the χ 2 test. The groups showed normal distribution, and the variances were homogeneous. One-way analysis of variance was used to compare VAS, UCLA, and WORC scores among the groups. For binary comparisons, Tukey’s post hoc analysis was done. These analyses were performed using SPSS software (Version 20.0 for Windows, SPSS, Chicago, IL, USA).
On the basis of power analysis, the minimum sample size of patients (27 patients) was calculated using a 20% difference in VAS scores at an α level of 0.05 and β level of 0.08. The study included a total of 68 patients, 38 patients with anterior greater tubercle cysts, taking into consideration the similar comparative retrospective studies performed in the literature. 1,15,19 –21
Results
Age, gender, and side of shoulder involvement distribution characteristics of the groups are summarized in Table 1. There was no significant difference between age, gender, and side of shoulder involvement distribution among the groups (p >0.05).
Age, gender, and side of shoulder involvement distribution characteristics among the groups.a

M: male; F: female; SD: standard deviation; D: dominant; ND: nondominant.
aValues are expressed as mean ± SD and range.
b p Value shows the results of χ 2 test.
c p Value shows the results of Tukey’s post hoc test.
There was a statistically significant difference in the clinical results of VAS, UCLA, and WORC among the cystic and noncystic groups in the anterior greater tubercle (p < 0.05). There was also a statistically significant difference in the clinical results of UCLA, WORC, and VAS scores according to the cyst sizes in the anterior greater tubercle cyst group (p < 0.05). The comparison of the preoperative and postoperative means of UCLA, WORC, and VAS scores among the groups is shown in Table 2.
Comparison of preoperative and postoperative results among the groups.a

SD: standard deviation; UCLA: University of California at Los Angeles Shoulder Rating Scale; WORC: Western Ontario Rotator Cuff Index; VAS: visual analog scale.
aValues are expressed as mean ± SD. p Value shows the results of Tukey’s post hoc test.
bSymbolizes the difference between cyst absent to cyst present (<5 mm).
cSymbolizes the difference between cyst absent to cyst present (≥5 mm).
dSymbolizes the difference between cyst sizes.
The comparisons of postoperative 6th month and 12th month UCLA and WORC results among groups with boxplot graph are shown in Figure 4.

Comparisons of postoperative 6th month and 12th month UCLA and WORC results among groups with boxplot graph. UCLA: University of California at Los Angeles Shoulder Rating Scale; WORC: Western Ontario Rotator Cuff Index
Discussion
In our study, the presence of anterior greater tubercle cysts negatively affects rotator cuff repair results. In comparison between the cyst sizes, the rotator cuff repair results of the patients with a cyst size greater than 5 mm are more affected.
In a work by Williams et al., 5 humeral cysts are most often located in the posterior aspect of the greater tubercle, communicate with the joint space, and in this location are not related to aging or rotator cuff tear. In a study by Suluova et al., 4 anterior greater tubercle cysts found a strong relationship regardless of the age of rotator cuff pathologies. Other studies have reported association between greater tubercle cysts and rotator cuff tears. 1,2,7 According to the studies, anterior greater tubercle cysts are reported to be associated with rotator cuff pathologies. 1,2,4,5,7
There is information about increased cystic changes in humeral head with age. 2,4,5,7 There are also negative effects of rotator cuff repair results in advanced age. It is known that cysts are associated with degeneration. 4,7 Studies have also reported that older age has a negative effect on rotator cuff healing and that the size of the defect in elderly patients leads to poor clinical outcomes. 22 –25 There was no difference in age distribution among the groups in our study.
There are many factors that affect rotator cuff repair. These include age, tear size, fatty infiltration and rotator cuff atrophy, surgical technique, rehabilitation protocols, and other patient-related factors (metabolic effects, diabetes, cholesterol, smoking, and various laboratory values), which affect the healing process. 22,26,27 Metabolic factors related to the patient were included in the study during the postoperative period as much as possible between groups with the same standards. All groups followed the same postoperative rehabilitation protocol.
The most commonly used UCLA score was used to assess outcomes 7 and was assessed with WORC, which received better responses in other assessment tools. 17,18 VAS was used for pain evaluation.
According to our results, anterior greater tubercle cysts have negative effects on rotator cuff repair. We believe that this negative effect depends on a few reasons. Firstly, the cysts in the humeral head are associated with increased porosity and poor bone quality. 9,10,28 –30 Secondly, anterior greater tubercle cysts may cause technical difficulties during repair of rotator cuff tears, especially of large cysts. A cyst in the rotator cuff footprint decreases the biological healing capacity of the repair and can compromise the fixation strength of suture anchors used in the repair. 9,10,31
Limitations of the study included the following: firstly, small sample size; secondly, detailed description of rotator cuff tears and no tendon separation; thirdly, no radiological comparison of results; fourthly, the evaluation period of clinical outcomes is short; and fifthly, adverse effects of patient-related metabolic factors during the healing process. Nevertheless, we believe that this study is meaningful. Additional comprehensive studies are required with comparisons of MRI results, detailed description of rotator cuff tears, and long evaluation period.
Conclusion
Rotator cuff repair results of patients with the cyst detected in anterior greater tubercle cysts in MRI are affected negatively. The effects of cysts larger than 5 mm on rotator cuff repair results were found to be more prominent and significant. An understanding of anterior greater tubercle cystic defects is of critical importance in planning rotator cuff surgery. Therefore, safe operation technique and secure suture anchor fixation must be addressed during rotator cuff repair in patients with anterior greater tubercle cysts.
Footnotes
Author contributions
Mehmet Hamdi Şahan contributed to planning, designing, data collection, literature survey, statistical analysis, and writing. Sancar Serbest and Uğur Tiftikçi involved in planning, designing, data collection, and literature survey. Erdogan Durgut contributed to planning, data collection, and literature survey. Mikail İnal involved in planning, designing, and literature survey.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.