
Abstract
Purpose:
The prevalence and distribution of air present in the leg in closed and low-grade open tibial shaft fractures are unknown on multidetector high-resolution computed tomography (CT). The purpose of this study was to determine the rate of surgical site infection (SSI) in cases where debridement was not performed in the area of air infiltration.
Methods:
Eighty-one closed and low-grade open tibial shaft fractures that underwent multidetector high-resolution CT on admission and were treated with an intramedullary nail were examined retrospectively.
Results:
Of the 36 Gustilo type I or II open fractures, all had local air around the fracture site (within 5 cm proximal and distal from the fracture center). Of these, 25 showed remote air (more than 5 cm away from the fracture center). The most frequent site of remote air was in the subcutaneous tissue, followed by the anterior compartment and deep posterior compartment. All open fractures were treated with local irrigation and debridement, regardless of the presence of remote air, followed by a reamed intramedullary nail. No SSI developed until bone union. Of the 45 closed fractures, 3 patients showed air in the leg on the CT. No debridement was performed for closed fractures. One patient who did not have air in the leg developed SSI. All fractures united eventually.
Conclusions:
In low-grade open tibial shaft fractures, air can spread far from the fracture site. Even in closed tibial shaft fractures, air can be identified in the leg. The debridement of the area of air infiltration, however, is not necessary for prevention of SSI.
Introduction
Open fractures of the lower extremity always lead to increased risk of surgical site infection (SSI). The disruption of skin introduces air and environmental bacteria into the depth of the extremity. 1,2 The presence of air in the subcutaneous tissues has also been considered to indicate severe degloving injuries, which require urgent irrigation and debridement in open fractures. 1 –3 However, the sensitivity of detection of air in soft tissues is not sufficient on plain radiographs. Further, there is no evidence in the literature to support that debridement of the area of air infiltration is essential to prevent SSI in open fractures. Recently, it has been reported that the presence of air in the leg was not rare on a computed tomography (CT) scan, even in closed lower extremity fractures. 4 Thus, there remains controversy whether air in the leg is representative of contamination.
Previously, CT was not routinely obtained in tibial shaft fractures for preoperative evaluation. However, several authors reported that tibial shaft fractures are commonly associated with both contiguous and noncontiguous intra-articular fractures. 5 –9 Thus, several authors recommended performance of CT for tibial shaft fractures. 6 –8 Although opportunities to obtain preoperative CT images of tibial fractures have increased, most attention has been paid to articular fragments. To the best of our knowledge, no study has focused on findings concerning air distribution of tibial shaft fracture on multidetector high-resolution CT images.
Given the controversy in the literature regarding the clinical meaning of air in the leg, we sought to determine the presence of air in tibial shaft fractures on multidetector high-resolution CT images. The objective of this study was twofold: (1) identification of the location and distance of air from the fracture site in low-grade open fractures and (2) prevalence of air present in closed fractures. We also examined the rate of SSI in case irrigation and debridement was not performed in the area of air infiltration. We hypothesized that air was not an indicator of bacterial contamination, and thorough debridement of the area of air infiltration was not necessary to prevent SSI.
Materials and methods
This retrospective cohort study was approved by an institutional review board. We performed a review of operation registries at a Level I Trauma Center between January 2012 and December 2016. Patients who underwent intramedullary nail of a closed or Gustilo type I/II open tibial shaft fracture were identified. Exclusion criteria in this study were patients who sustained suspected Gustilo type III open tibial fractures. 10 The length of open wounds of apparently more than 3 cm (almost equal to a diameter of the tibia) and/or apparent presence of subcutaneous degloving injuries were excluded. Patients with Arbeitsgemeinschaft für Osteosynthesefragen Foundation and Orthopaedic Trauma Association (AO/OTA) classification of 42C in open fractures were also considered as Gustilo type III injuries. 11,12 Patients whose axial CT images were not stored as volume data (0.5 mm slice thickness) in Picture Archiving and Communication System (PACS) as of this study due to exceeding storage limit were automatically excluded. Sixteen patients with 18 legs could not undergo CT scan for the tibia during the initial evaluation due to their hemodynamic status. Four patients with four legs who all sustained closed fractures were lost to follow-up until bone union. Finally, a total of 81 tibial shaft fractures treated with intramedullary nailing consisting of 36 low-grade open fractures and 45 closed fractures were included in this study.
Patient management
After initial resuscitation of patients according to the Advanced Trauma Life Support guidelines, deformity and open wounds were closely examined and recorded as photographs. In the emergency room, no cultures of wound specimens were obtained, and no temporary irrigation was performed. The open wounds were covered with a sterile gauze and compressed until debridement in the operation room (OR). All patients with tibial shaft fractures were treated under the protocol where a multidetector high-resolution CT scan for the tibia was desirable for evaluation of fracture extension, when patients’ vital signs were stable. The patients with open fractures were taken to the OR at the earliest opportunity afforded by the patients’ medical condition and OR availability; however, we did not adhere to the “six-hour rule” when patients sustain open fractures. 13 –15 Patients with closed fractures usually underwent surgical fixation within 24 h. In the OR, closed fractures were usually stabilized with a reamed intramedullary nail without open reduction of the fracture site. In open fractures, irrigation and debridement were performed with a few centimeters extension of an open wound proximally and distally. The area of debridement was not affected by the information of preoperative CT. Remote air was not irrigated or debrided. After adequate local debridement under direct vision and copious irrigation using a syringe with sterile saline, immediate reamed intramedullary nailing was usually performed. When patients sustained multiple injuries and were considered not suitable for immediate internal fixation, external fixation is chosen. In such cases, the conversion to a reamed intramedullary nail was usually performed within 1 week.
Research ethics and patient consent
This study was approved by the institutional review board of our hospital. Obtaining the informed consent from involved patients was waived by the institutional review board.
Data collection
The medical records of the 81 patients who underwent intramedullary fixation were reviewed, and all data, including age, sex, and fracture type according to AO/OTA classification, were collected. The presence of open wounds and type of open fracture according to Gustilo classification and performance of immediate intramedullary fixation or temporary external fixation prior to nailing were recorded from operative notes. The date of last plain radiographs of the affected tibia was considered as the final follow-up date. Mean ± standard deviation was used for continuous variables. Postoperative complications that required surgical intervention, such as nonunion and SSI, were also recorded.
Radiographic measurement
Radiographic images were reviewed and interpreted using PACS software (Centricity Enterprise Web V3.0 Internet Explorer; GE Healthcare, Little Chalfont, UK). For plain radiographs, anteroposterior view and lateral view were used to detect air density while changing window level and window width voluntarily. Two fellowship-trained orthopedic trauma surgeons (TS and YN) reviewed the plain radiographs independently. We assumed the presence of air with inter-reviewer agreement. When disagreement occurred, the final decision was made with the additional information from CT.
All CT images were obtained using a 64-row multidetector CT scanner (Aquilion 64; Toshiba Medical Systems, Japan). The presence of air was reviewed as 0.5 mm thickness slice axial CT images using window level:500 and window width:2300 as a standard contrast. A positive finding of air was defined as a minimum of 1 mm diameter decreased density consistent with air with −750 Hounsfield units or less as measured on PACS. The distance of air from the center of the fracture site was read by the slice number linking scout view. The most remote air was recorded as its distance. The open wounds were assumed to be located around the center of the fracture. We defined air within 5 cm proximal and distal from the center of the fracture (10 cm length in total) as local air. Air outside the 10 cm length centered at the fracture site was defined as remote air. Due to difficulty of identification of air location around the fracture site, its location was recorded only for remote air. The location of air was divided into (1) subcutaneous tissue, (2) anterior compartment, (3) lateral compartment, (4) superficial posterior compartment, (5) deep posterior compartment, and (6) bone marrow. Detection of remote air between plain radiographs and CT images was compared by statistical analysis using IBM SPSS 23 (IBM, New York, NY). Group comparison was performed using a χ 2 test. The level of significance was set at p < 0.05.
Results
The study group included 57 males and 24 females with a mean age of 47.9 ± 19.8 years. The mean follow-up period was 492 ± 217.5 days. According to the AO/OTA classification, there were 41 type A, 35 type B, and 5 type C fractures (Table 1). All the type C fractures consisted of closed fractures. Of the 36 open fractures, 15 were classified as Gustilo type I and 21 were classified as Gustilo type II. Of these, 18 patients underwent sequential intramedullary nailing following irrigation and debridement, whereas the other 18 initially underwent external fixation. Of the 45 closed fractures, 33 were immediately fixed with an intramedullary nail, whereas 12 underwent external fixation initially.
Characteristics of AO/OTA and Gustilo open fracture type.

AO/OTA: Arbeitsgemeinschaft für Osteosynthesefragen Foundation and Orthopaedic Trauma Association.
In the open fracture group, air on plain radiographs was observed in 18 of the 36 cases. In 11 cases, remote air was observed, all of which were located in the subcutaneous tissue. The other 18 cases showed no air on plain radiographs. In contrast, on CT axial images, more than one pocket of air was observed in all cases. Eleven showed only local air and consisted of six Gustilo type I and five Gustilo type II fractures. The other 25 (69.4%) showed remote air and local air. The detection of remote air on the CT group was more sensitive compared with the plain radiograph group with statistical significance (p = 0.001). Table 2 lists 25 cases with remote air in open fractures. Of these 25 cases, the most frequent location of remote air was in the subcutaneous tissue (80%), followed by the anterior compartment (11%) and deep posterior compartment (10%). The longest distance from the fracture site was 282 mm, which was classified as Gustilo type I (Figure 1). Bone union was obtained in 34 cases within 1 year from the injury. The remaining two were distal one-fourth shaft fractures and failed in aseptic nonunion due to the lack of sufficient stability. Augmentative plating and bone grafting or decortication of the nonunion site achieved bone union eventually. No SSI developed in the open fracture group.
Characteristics of patients with remote air in open fractures.

CT: computed tomography; PR: plain radiograph.
a Air location of the longest distance.
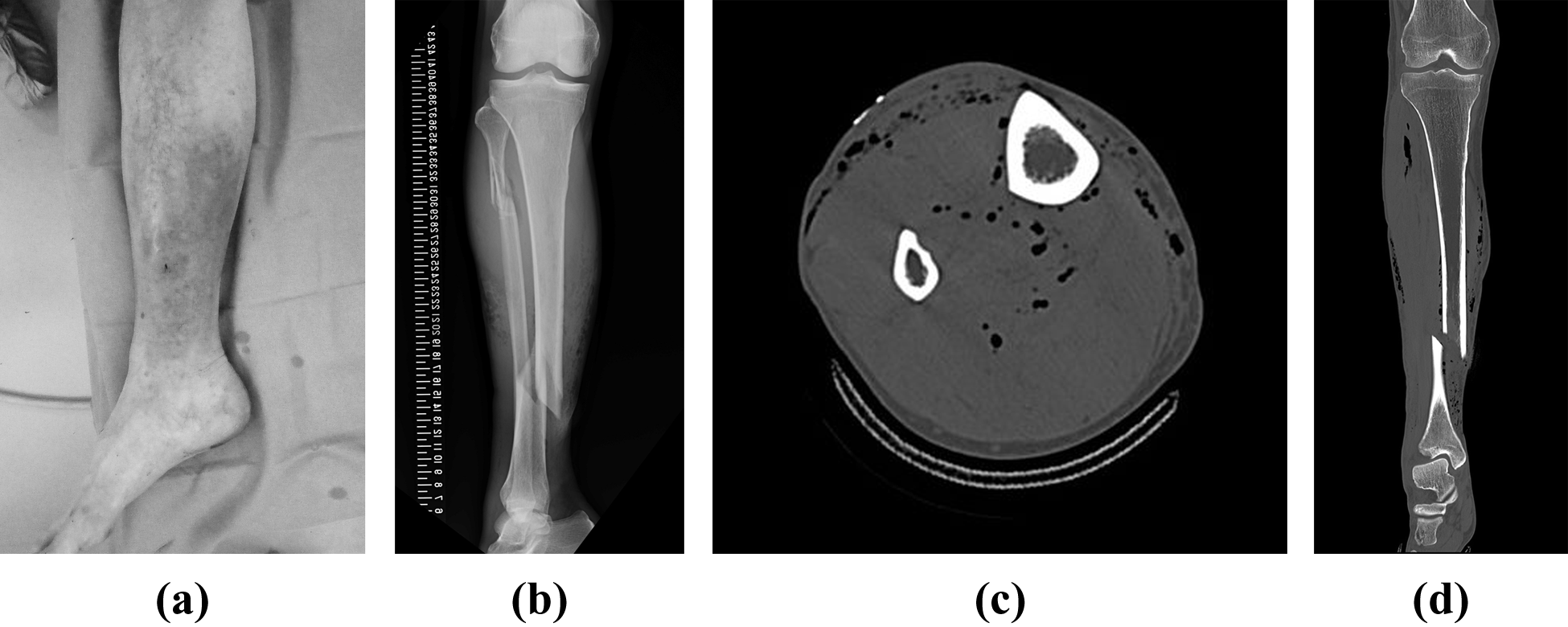
A 69-year-old male sustained a Gustilo type I open tibial shaft fracture on the right side by falling from standing height. (a) Picture showing a pinhole open wound on the distal one-third anteromedial side of the leg. (b) Anteroposterior radiograph of the tibia on admission. (c) Axial CT demonstrating multiple pockets of air in different compartments. (d) Coronal reconstructed CT showing linear air tracks connecting fracture site to deep soft tissues.
In the closed fracture group, there was no patient who showed air on plain radiographs. However, three cases with air on CT images were identified. One was an impeding open fracture, and three small pockets of air were observed just under the skin tented by a fracture. Another case showed a linearly aligned air track on multiplanner reconstructed CT images. Meticulous inspection of medical records and photographs revealed that this patient had sustained a 2 cm ipsilateral laceration on the dorsi-medial foot. In the remaining patient, one small pocket of air was identified in the anterior compartment 32 mm away from the fracture site, and no possible source of air could be found. In these three cases, SSI did not develop although there was no irrigation and debridement of the fracture site at intramedullary nailing. However, one case that did not show any air on CT images developed SSI. There was no nonunion in the closed fracture group.
Discussion
The determination of the area of irrigation and debridement in open fractures is crucial to prevent SSI. 1 –3,10 Air and foreign bodies can be sucked through an open wound into the fracture site and adjacent tissues. When an injury shock wave produces soft tissue stretching, tearing, or laceration, paths between an open wound and the deep tissues of a limb may develop at the fracture site and communicate with each other. To eradicate contamination and devitalized tissues, thorough debridement of soft tissue injuries ideally is required. There has been some expert opinion that air in the soft tissues in a puncture wound or small laceration indicates severe degloving injuries and needs to be irrigated and/or debrided completely. 1,2 However, to the best of our knowledge, no studies have been conducted to evaluate the necessity of extension of the open wound and fascia to the area of air infiltration. The present study focused on the presence of air on preoperative high-resolution CT images. At least more than one pocket of air is always present even if no air is visible on plain radiographs. Remote air far from the fracture site where routine irrigation and debridement cannot be achieved is commonly observed.
It has been reported that plain radiographs have low sensitivity for detecting air in the body and that the CT scan is a useful modality to detect ectopic air to identify occult injuries. Konda et al. reported that CT scan improved detection of periarticular open fractures. They revealed that, compared with plain radiographs, CT scans altered the management plan in 43% of their patients. 16 In another article, the authors have also reported that the CT scan has 100% sensitivity and is specific to detect traumatic arthrotomies and periarticular wounds not requiring surgical intervention. 17 Scolaro showed that CT scans found abnormal extra-luminal air to diagnose and manage open pelvic fractures. They revealed that only 36 of the 81 patients showed abnormal air on plain radiographs. 18 Due to its limited resolution in space and contrast, thick soft tissues or overlapping bone cause difficulties in detecting air on plain radiographs.
It has been presumed that the mechanism of remote air is a momentary vacuum that is produced when the exposed fracture is pushed back into soft tissues. 1 The present study revealed that air can easily spread along muscles, tendons, and subcutaneous fascia to distant sites. We showed that remote air was frequently seen in subcutaneous tissue, followed by the anterior compartment and deep posterior compartment. This finding seems to be reasonable since tibial shaft fractures usually create anteromedial open wounds by the in-side-out mechanism due to the limited soft tissue coverage of the tibial bone. The subcutaneous, anterior, and deep posterior compartments are adjacent to the tibia and easily continuous to the fracture site.
In the present study, the overall prevalence of SSI was 1.2% (1 of 81), which was comparable to the previous studies in which the infection rates of closed and low-grade open fractures including Gustilo type I and II have been reported to be 0–11.0%. 19 Interestingly, even in cases of no irrigation or debridement of the area of air, no SSI following a reamed intramedullary nail developed. If complete debridement of the area of air infiltration was required, one might need to extend open wounds all through linearly aligned small pockets of air in different compartments. This apparently creates large skin flaps, prevents adequate closure, and requires additional soft tissue procedures for closure. 20 Judging from our results, the presence of air does not always indicate a zone of injury that necessitates debridement and irrigation. 21
To date, it is generally accepted that there is no air in the leg of closed tibial fractures. Recently, Noble et al. reported that they found gas in as many as 23.5% (27 of 88) of closed tibial fractures using CT scans. 4 The authors speculated that the acute joint dislocation or a closed fracture produces negative pressure where dissolved gas from the solution results in gas accumulation, which is known as the vacuum phenomenon. In the present study, 3 of the 45 closed shaft fractures showed air in the leg. One was possibly an underestimation of micro-skin disruption. Another instance of unexpected air may be explained by the presence of a small open wound on the dorsomedial side of the foot and a linear air track along the tibialis posterior tendon visible on the CT scan in this patient. In the remaining case (2.2%, 1 of 45), isolated single air was observed in the anterior compartment. The patient sustained a closed tibial shaft fracture by falling from standing height, and the air may have been potentially caused by the vacuum phenomenon. Based on our results, the presence of air in purely closed tibial shaft fractures is not common in terms of vacuum phenomenon; however, air can be identified occasionally on multidetector high-resolution CT scan.
The present study has several limitations. One of the major weaknesses is its relatively small sample size. Next, due to the nature of a retrospective study, we could not analyze all the patients who underwent intramedullary nailing of the tibia during the study period. Third, only moderate reliability of Gustilo classification among different observers has been reported. 22,23 There must be some overlap among types of classification due to its limited reliability, and our strict inclusion criteria may have considered some of the Gustilo type II fractures as type III fractures. Further, it is widely accepted that the length of a wound in Gustilo type II ranges between 1 cm and 10 cm 24 while Gustilo did not describe maximum length in his classification. 10 Fourth, our results cannot be applied to high-grade open fractures. Due to the heterogeneous nature of Gustilo type III fractures, the spectrum of air distribution was diverse and prevented us from recording the location and distance objectively and numerically.
Conclusions
For the past decade, multidetector CT scans have been widely used and provided much information regarding fracture characteristics, severity, and even soft tissue injuries. The presence of more than one pocket of air in the leg without any other open wounds is indicative of an open fracture, while the air on CT images can be occasionally identified even in closed tibial shaft fractures. The presence of a wide area of air infiltration in Gustilo type I or II fractures with a small open wound is a common finding, and there is no need for thorough debridement of the area of air infiltration for prevention of SSI.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.